A Case of Bilaterally Elongated Styloid Process Differing in Osseo-Morphology
Hironmoy Roy1, Radharaman Mondal2, Kuntala Ray3, Maitreyee Kar4, Narayan Pandit5
1 Assistant Professor, Department of Anatomy, North Bengal Medical College, Darjeeling, West Bengal, India.
2 Demonstrator, Department of Anatomy, North Bengal Medical College, Darjeeling, West Bengal, India.
3 Assistant Professor, Department of Community Medicine, North Bengal Medical College, Darjeeling, West Bengal, India.
4 Assistant Professor, Department of Anatomy, North Bengal Medical College, Darjeeling, West Bengal, India.
5 Associate Professor, Department of Radiodiagnosis, RG Kar Medical College, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hironmoy Roy, Assistant Professor, Department of Anatomy North Bengal Medical College, P.O. Sushrutanagar, District Darjeeling, West Bengal-734012, India.
Phone: +91 9748828588,
E-mail: hironmoy19@gmail.com
In a cranium of a male cadaver styloid processes have been found to be unusually long with different lengths. Elongation of styloid process involvethe entire ‘Stylohyoid complex/chain’, though not rare as reported in earlier literatures, but the osseomorphological and radiological analysis of present case brings out a unique variety as its described in the article.
Elongated styloid process, Stylohyoid chain
Case Report
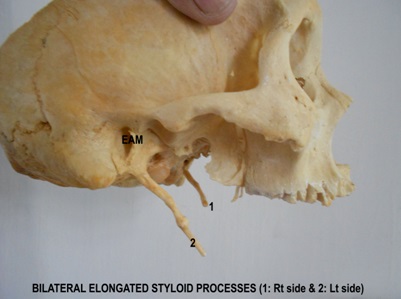
After preparation of bones from a 55-years-old male cadaver, in its cranium it has been found that styloid processes in both sides are elongated; 5.5 cm in right side and 3.8 cm in left side. On the right side, the elongated styloid process shows a nodulation (pseudo-articulation) 3.5 cm distant from its base [Table/Fig-1, 2].
Demonstrates the bilateral elongated styloid process (ESP) by marking ‘1’ for the left side and marking ‘2’ for right side. [EAM: External acoustic meatus]
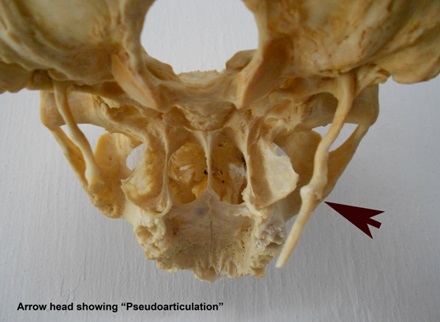
Showing “pseudoarticulation” by pointing black arrow in the right sided elongated styloid process
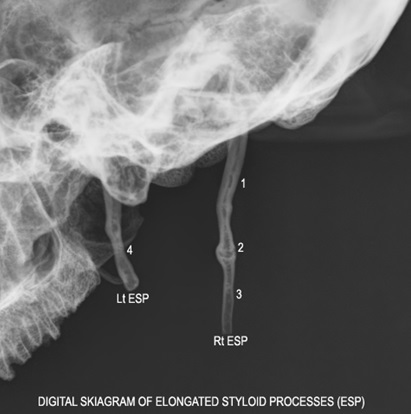
On the digital skaigram of the skull base, it got evident that in the whole of the elongated styloid process of left side was partially calcified. So, for the right side had the partially calcified proximal part with intermittent translucent core and in the distal part had only calcified in outline. The nodular portion i.e. the junction of the two parts of that of right side had a horizontal translucent gap seemed to be a joint without any movement [Table/Fig-3].
Above photograph showing the digital roentgenogram of the elongated styloid processes illustrating the type/nature of calcification
Rt ESP: Right sided Elongated styloid process
Lt ESP: Left sided elongated styloid process
[1] Showing the partial calcification of proximal part (stylohyal part) of the right elongated styloid process
[2] Showing the core of “pseudo-articulation” portion of the right elongated styloid process, where a translucent horizontal gap is noted
[3] Showing the ceratohyal part of the elongated styloid process; where the core is not ossified; only the outline is calcified
[4] Showing the stylohyal part of the left elongated styloid process where the core is partially ossified
Discussion
The styloid process is a thin and sharp bony structure, protruding downward and forward from the underside of the temporal bone having average length of 2.5cm; with a base or proximal part ensheathed by tympanic plate and shaft or distal part with muscle & ligament attachment. Length of the styloid process when exceeds 3 cm it is said to be “elongated” (Elongated styloid process or ESP) [1,2].
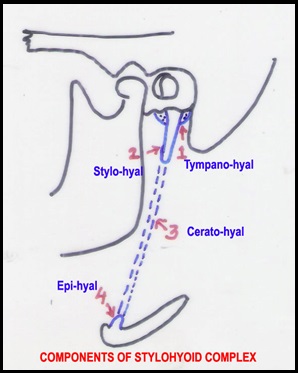
The entire ‘stylohyoid chain’ can be zoned as the tympanohyal (part enclosed by vaginal plates, or root of the styloid process), stylohyal (forming major portion or shaft of the styloid process), ceratohyal (the stylohyoid ligament) and hypohyal part (which is actually the minor horn of hyoid bone) [Table/Fig-4], derived embryologically from Reichert’s cartilages (of second branchial arch) [1–6].
Showing the different components of ‘Stylohyoid Complex’
In the adult the styloid ligament, normally composed of dense fibrous connective tissues may retain some of its embryonic cartilage and this have the potential to become partially or completely ossified in later life. Such as the ossification can get triggered by a pharyngeal trauma in form of hyperplasia or metaplastic alteration in cells of stylohyoid ligament. Another possibility is the mineralization of the ligament as a result of ageing and degenerative processes along with the spondylosis of cervical vertebra [6–10].
The incidence of elongated styloid process is reported to be 4 to 7% as a whole. Whereas amongst them only 4%0 to 10.3% presents with of glossodynia, dysphagia, dysphonia in combinations enmarking the Eagles’ syndrome [10,11]. Even earlier studies have reported that elongated styloid process might lead to carotid compression to transient ischemic attack [12–15] and even it has been reported in a case of Turner’s syndrome [14].
Morphologically the elongated styloid process has been classified in three types-Type I (elongated/unsegmented), II (pseudo-articulated segments), and III (completely segmented). Depending on the calcification of the core it gets categorized in four as-category A (only outline calcified with continuous translucent core), category B (core partially calcified), category C (nodular calcification of core) and category D (core completely calcified) [16].
Following this here is the left sided elongated styloid process belongs to morphologically Type I (elongated styloid process) and in category B by calcification (partially calcified). On the other hand in right side it is of pseudo-articulated variety (Type II) with proximal part partially calcified (category B) and distal part having only outline calcified (category A). So, far the pertinent literature searched such un-equivocal mineralization in different part of same elongated styloid process, not been reported earlier.
Conclusion
Elongated styloid process or the calcified stylohyoid chain not only bears importance for an anatomist but also have implication to ENT surgeons. Although majority are accidental in diagnosis, but each of them carries a potentiality for Eagle’s syndrome. Bilateral existence of it is though reported in some articles but bilateral asymmetrical pattern rarely found in literature till searched for.
[1]. Standring S, External skull. Head & Neck (Sec 4, Ch 26). In, Standring S (eds.)Gray’s Anatomy The Anatomical Basis of Clinical Practice 2008 40th ednPhiladelphiaChurcill livingstone Elsevier:412 [Google Scholar]
[2]. Standring S, Temporal bone. External and Middle ear (Sec 4, Ch 36). In, Standring S (eds.)Gray’s Anatomy The Anatomical Basis of Clinical Practice 2008 40th ednPhiladelphiaChurcill livingstone Elsevier:617 [Google Scholar]
[3]. Collins P, Second pharyngeal arch. Embryology & Development (Sec 3) In, Bannister LH, Berry M, Dayson M (eds.)Gray’s Anatomy 1995 38th ednPhiladelphiaChurcill livingstone:284 [Google Scholar]
[4]. Mukherjee P, Palit S, Tapadar A, Roy H, Asymmetrical bilateral ossification of stylohyoid chains – a case report with embryological reviewInternational Journal of Anatomical Variation 2011 4:134-6. [Google Scholar]
[5]. Bagoji IB, Hadimani GA, Patil BG, Bannur BM, Bharatha A, Bilateral Elongated Styloid Process: Its Anatomical Embryological And Clinical ImplicationsInternational Journal of Medical Research and Health Sciences 2013 2(2):273-6. [Google Scholar]
[6]. Hollinshed WH, Styloid process and variationsIn, Anatomy for surgeons 1982 3rd volumePhiladelphiaJ.B. Lippincott Co.:54-3. [Google Scholar]
[7]. Keurr JJ, Campbell JPS, McCarthy JF, The clinical significance of the elongated styloid processOral surgical oral med oral pathol 1986 61:399-404. [Google Scholar]
[8]. Murtagh RD, Caracciolo T, Fernandez G, CT findings associated with Eagle syndromeAJNR Am J Neuroradiol 2001 22:1401-2. [Google Scholar]
[9]. Piagkou M, Anagnostopoulou S, Kouladouros K, Piagkos G, Eagle’s syndrome: a review of the literatureClin Anat 2009 Jul 22(5):545-8. [Google Scholar]
[10]. Eagle WW, Elongated styloid processArchives of otolaryngology 1937 25Chicago:584-7. [Google Scholar]
[11]. Harma R, StylalgiaActa Otolaryngol, supple (Stockh) 1967 224:149-55. [Google Scholar]
[12]. Song JH, Ahn SK, Cho CB, Elongated Styloid Process as a Cause of Transient Ischemic AttacksJAMA Neurol 2013 Jun 24:1-4. [Google Scholar]
[13]. Sveinsson O, Kostulas N, Herrman L, Internal carotid dissection caused by an elongated styloid process (Eagle syndrome)BMJ Case Rep 2013 Jun 11 :13-5. [Google Scholar]
[14]. Evlice B, Tatli U, Yazicioglu I, Evlice A, Oztunc H, A unique case of Turner syndrome accompanying prolactinoma and unexpected elongated styloidprocess: Clinical and cone-beam computed tomographic featuresImaging Sci Dent 2013 Jun 43(2):129-34. [Google Scholar]
[15]. Yamamoto S, Todo K, Kawamoto M, Kohara N, Carotid artery dissection associated with an elongated styloid processIntern Med 2013 52(9):1005-6. [Google Scholar]
[16]. Langlais RP, Miles DA, VanDis ML, Elongated and mineralized stylohyiod ligament complex: proposed classification and report of a case of Eagle’s SyndromeOral surgical oral med oral pathol 1986 61:527-32. [Google Scholar]