Perception on the Relationship between Cancer and Usage of Tobacco and Alcohol in Hail, Saudi Arabia
Ibrahim Abdelmageed Ginawi1
1 Vice Dean, Department of Family and Community Medicine, College of Medicine, University of Hail, Kingdom of Saudi Arabia.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ibrahim Abdelmageed Ginawi, College of Medicine, University of Hail, Kingdom of Saudi Arabia. Ph: +966 506771772,
E-mail: iginawi71@gmail.com
Aim: Increasing alcohol consumption in many countries is an important cause of cancer worldwide. The aim of this study was to evaluate the burden of tobacco use and alcohol consumption and its related perception among population of Hail, Saudi Arabia.
Methodology: A cross-sectional survey from March to April 2012 covering 451 participants, in the city of Hail, Northern Saudi Arabia.
Results: Out of 451 respondents, 355(78.7%) were male and 96 (21.3%) were female giving a male to female ratio of 3.7:1. The age range of respondents was 11 – 77 years with a mean of 32 years. Prevalence of tobacco use and alcoholic beverages consumption were 30.3% and 7.5%, respectively. Most of the tobacco users and alcohol consumers showed positive knowledge concerning the relation between tobacco use and/or alcohol consumption and cancer.
Conclusion: It is evident that the prevalence of tobacco consumption is rising in the Hail region. Female participation in tobacco and alcohol related studies in the Hail – Saudi Arabia represent a major obstacle since it is considered as social stigma due to complete prohibition by law.
Alcohol, Tobacco, Cancer, Tobacco consumption
Introduction
A relationship between alcohol consumption and cancers of the oral cavity, pharynx, oesophagus, liver, colon, rectum, and, in women, breast has been established [1]. The importance of alcohol as a human carcinogen is often underestimated and consumption is rising in many countries as a result of both increasing numbers of alcohol drinkers and intake of alcohol, especially for women and in regions of rapid economic growth such as East Asia [2]. Alcohol is probably the main factor responsible for increased risk of head and neck cancer recorded in various countries, particularly in central and Eastern Europe [3]. Evidence suggests that genetic susceptibility plays an important part in alcohol-related cancer, and knowledge of possible mechanisms of the carcinogenic action of alcohol has increased in recent years.
Tobacco is the second major cause of death in the world [4]. Now a days, the mortality due to tobacco smoking has been estimated to be more than 5 million deaths annually which is expected to double by 2020. This significant impact is not only due to morbidity and mortality, but also attributed to the social and the economic cost of smoking [4]. Reports have indicated that the real impact of tobacco smoking could be underestimated because of high level of exposure of “secondhand” smoke, increased smoking among youths and the increase in smoking among non-smokers [5]. On the other hand, a review showed that most Non-Communicable Diseases NCDs are strongly associated and causally linked with four particular behaviors: tobacco use, physical inactivity, unhealthy diet and the harmful use of alcohol [6]. These behaviors lead to four key metabolic/physiological changes: raised blood pressure, overweight/obesity, hyperglycemia and hyperlipidemia. In terms of attributable deaths, the leading NCD risk factor globally is raised blood pressure (to which 13% of global deaths are attributed), followed by tobacco use (9%), elevated blood glucose (6%), physical inactivity (6%), as well as overweight and obesity (5%) [7]. However, in the developed world, a strong inverse relationship between socio-economic status and smoking exists such that the poorest and least educated populations are more likely to smoke [8].
Alcohol use is related to a wide variety of negative health outcomes including morbidity, mortality and disability. Alcohol-abuse and alcoholism are one of the major public-health problems in both developed and developing countries. In 1979, the 32nd World Health Assembly declared that “problems related to alcohol and particularly to its excessive consumption rank among the world’s major public health problems and constitute serious hazards for human health, welfare and life” [9]. The World Health Organization (WHO) estimated that there are about two billion consumers of alcoholic beverages and 76.3 million people with diagnosable alcohol-use disorders worldwide [10]. Alcohol consumption accounts for nearly 3.2% of all days and 4% of all disability-adjusted life-years (DALYs) lost [11]. In addition to chronic diseases, such as cancer of the mouth, esophagus and larynx, liver cirrhosis, and pancreatitis, social consequences, such as road-traffic accidents, workplace-related problems, family and domestic problems, and interpersonal violence, have been receiving more public or research attention in recent years [12].
A causal relation between increased alcohol consumption and squamous-cell carcinoma of the oral cavity, pharynx, larynx, and esophagus has been noted since the mid 1950s. And epidemiological studies of these tumors have shown a neoplastic effect of heavy alcohol intake and a linear correlation with both duration and amount of consumption. A synergism between alcohol intake and tobacco smoking was reported since 1970s, and has become a paradigm of interaction of two environmental factors in human carcinogenesis [1]. A carcinogenic effect of alcohol independently from that of smoking (i.e., an increased risk in the non-smokers) was first reported in 1961 [13] and has been reported again [14,15]. These subsequent studies have shown a fairly consistent dose-response relation between alcohol consumption and risk of cancer in the upper aerodigestive tract for nonsmokers.
This study is very important because about 75% of head and neck cancers diagnosed in Europe, the United States, and other industrialized regions are attributable to the combination of cigarette smoking and alcohol drinking [16]. However, the respective contributions of these risk factors to head and neck cancer risk are difficult to study because these two habits are strongly associated with each other [17]. So understanding of the independent associations between cigarette smoking and alcohol drinking and the risk of cancer has important role to explain the mechanisms of carcinogenesis and for assessing the effects of interventions to modify these risk factors.
This study is aimed to identify the frequencies of tobacco use and alcohol intake among different population settings in Hail – Saudi Arabia to provide data, so that it might be beneficial in planning, implementation, and evaluation of appropriate programs for the elimination of these harmful habits.
Material and Methods
This is a community-based, cross-sectional study conducted in Hail – Saudi Arabia, during the period from March to April, 2012. Data was collected as part of the medical students’ activities in research methodology module. Volunteers in schools, health centers and malls were asked to fill the study questionnaire about tobacco and alcohol habits and other information regarding their attitudes towards these factors.
Statistical Analysis
Statistical analysis was performed by proportion. The Microsoft Excel Office 2007 and the SPSS software (version 16) were used for statistical analysis.
Ethical Consent
Written informed consent was obtained from each respondent, ensuring strict anonymity. The Ethical Committee of the Deanship of Scientific Research – University of Hail, has approved the study.
Results
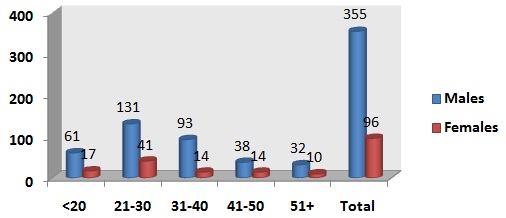
A total of 451 adults were responded to this study. Out of 451 subjects, 355(78.7%) were male and 96 (21.3%) were female giving a male to female ratio of 3.7:1. The age range of respondents was 11 – 77 years with a mean of 32 years as shown in [Table/Fig-1].
Distribution of age and gender
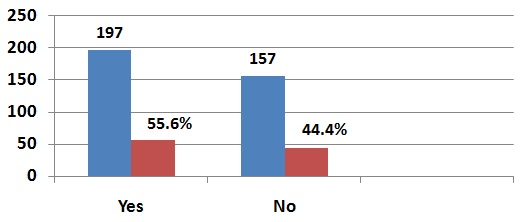
In this survey 143 (30.3%) of the respondents were smokers while 35 (7.5%) were alcohol consumers and 25 (72%) from alcohol users were smokers also. On the other hand, 332 (69.7%) and 440 (92.5%) of respondents had never smoked tobacco and never consumed alcohol, respectively in their lifetime. But among the 332 (70%) who never smoked tobacco, we found that 197 (55.6%) were living with tobacco smokers, while 157 (44.4%) of them were not living with smokers as shown in [Table/Fig-2].
Percentage of respondents who are living with smokers
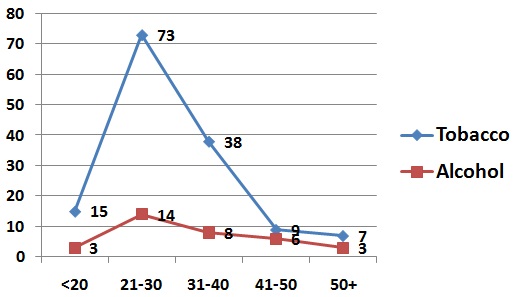
With regard to age, among tobacco smokers, higher percentages were observed among middle age groups, 21-30 and 31-40 years, constituting 51% and 27%, respectively. Higher alcoholic consumption was observed among middle age groups also, 21-30 and 31-40 years representing 40% and 23.5% respectively, as shown in [Table/Fig-3].
Using of tobacco and alcohol in regards to age
[Table/Fig-4] summarizes, tobacco and alcohol habits among different education levels. Individuals at high school and graduate levels represented the highest proportions in smoking and alcohol drink. 57/154 (37%) from high school and 64/141 (45.4%) from graduated were smokers, while 16/137 (11.7%) from high school and 15/183 (8.2%) from graduated were alcohol users.
Tobacco and alcohol habits among different educational levels
| Type of habit | Educational level |
|---|
| Illiterate | Primary School | Intermediated School | High School | Graduate | Post-Graduate |
| Tobacco | 0 | 1 | 12 | 57 | 64 | 5 |
| Alcohol | 0 | 0 | 1 | 16 | 15 | 2 |
[Table/Fig-5] summarizes tobacco and alcohol habits by occupation which revealed that the highest percentage of tobacco and alcohol users were observed among teachers and employee constituting, 26/69 (37.7%) and 30/78 (38.5%) for tobacco using and 4/60 (6.7%), 8/69 (11.6%) among alcohol users respectively.
Tobacco and alcohol habits by occupation
| Type of habit | Type of Occupation |
|---|
| Farmer | House wife | Labour | Student | Teacher | Employee | Others | No. Job | Faculty Member |
| Tobacco | 1 | 0 | 2 | 13 | 26 | 30 | 17 | 16 | 4 |
| Alcohol | 0 | 0 | 0 | 1 | 4 | 8 | 4 | 2 | 2 |
Concerning knowledge level towards the risk of tobacco and alcohol in causing cancer, 96% respondents knew that tobacco can cause cancer and 98.2% of them agreed that alcohol consumption can cause cancer.
Discussion
World Health Organization (WHO) reported Saudi Arabia as one of the nine countries that has a complete ban on alcohol. The other countries include Afghanistan, Brunei Darussalam, the Islamic Republic of Iran, Maldives, Mauritania, Pakistan, Saudi Arabia, Somalia and Sudan. And other four countries report partial bans: Bangladesh, Comoros and India (in five states), and Qatar [18]. So there is a lack of population based data on alcohol consumption in Hail – Saudi Arabia and even all regions of Saudi Arabia which give this study a unique and pioneer situation, because it is important to do studies to provide data to improve the local understanding of tobacco and alcohol burden which is a scientific and evidence based to an effective strategies to prevention and control program. Therefore, the aim of this study was to carry out an epidemiological survey on tobacco and alcohol use in Hail – Saudi Arabia. However, there is many studies on tobacco use performed in Saudi Arabia but no study conducted in Hail. There is study carried out in 2010 in Eastern province, Saudi Arabia [19], and it reported that The prevalence of current smoking (smoked > 100 cigarettes or any tobacco products including water pipe in lifetime and still smoking daily or occasionally for 1 month or more) among 196 268 respondents was 16.9% (28.7% among men and 4.5% among women). There was a significantly higher prevalence of smoking at younger ages in men and older ages in women. Multiple logistic regression analysis showed that factors independently associated with smoking were lower socio-economic status, lower education, being divorced and occupations such as the military and self-employed. On the other hand another tobacco survey conducted in two medical schools in Riyadh [4] showed that 19% of the male students have smoked tobacco at the time of the study which raises the prevalence among male students to 24%. And they mentioned that tobacco smoking was practiced by males more than females (p value <0.0001) and by senior more than junior students (<0.0001). About 94% of the study samples indicated that smoking could cause serious illnesses. Despite good knowledge about the hazards of tobacco consumption, about 25% of the medical students in this study continue to smoke. About 90% of the students indicated that they would advice their patients to quit smoking in the future and 88% thought that smoking should be banned in public areas. Sad enough that (20%) of students thought that smoking has some beneficial effects, mainly as a coping strategy for stress alleviation. Concerning alcohol consumption in Saudi Arabia data collected by the WHO Regional Office for the Eastern Mediterranean in 2003 estimates that the extent of alcohol use in Saudi Arabia is considerable and that data from the last five years suggest a stable trend in the use of alcohol [10]. On the other hand a cross-sectional study conducted in Al-Amal Hospital in Riyadh in March 1998 of 160 male patients aged 20 years or older found that alcohol was used by 23.75% of the patients [20]. Also in a study of 120 male inpatients in a hospital for treatment of male substance abusers in Dammam in Saudi Arabia’s eastern region, it was found that 12.5% of the sample abused alcohol singularly (without abuse of other drugs). DSM-IV criteria for the diagnosis of substance abuse was used in this study [21].
In this study, it was very clear that the use of tobacco related to low socio-economic status and most of the users are less educated although we can notice some users among highly educated, such as teachers and employee. Concerning alcohol consumption, Saudi Arabia is one of the nine countries mentioned above that the use of alcohol is completely prohibited by law. This situation makes it very difficult to know the real number of alcohol users and also the percentage revealed by this study can be just an ice berg. However the unrecorded alcohol consumption in Saudi Arabia is estimated to be 0.6 liters pure alcohol per capita for population older than 15 for the years after 1995 (estimated by a group of key alcohol experts) [22]. As we said before, alcoholic drinks are banned in Islam and the rules in Saudi Arabia set out in Quran and Hadith - the sayings of Prophet Mohammed (peace be upon him) - are strictly applied. And the punishment for drinking alcohol is a public lashing. But alcohol can be bought easily in some Muslim countries bordering Saudi Arabia - Jordan for example which give a chance for those who want to drink to bring it from those countries on illegal ways or some of them may go to locally prepared alcohol [23].
Conclusion
A limitation of this study is the problem of alcohol stigma which leads to less prevalence than the real and it may need a mixed method rather than self administered questionnaire such as highly recommended investigations to know the level of alcohol in the blood. On the other hand it is a cross-sectional design and the sample size need to increased, so the use of longitudinal studies of this population in the future might give up insight into developments in the results of future alcohol and tobacco control measures.
[1]. Boffetta Paolo, Hashibe Mia, Alcohol and cancer reviewLancet Oncol 2006 7:149-56. [Google Scholar]
[2]. World Health Organization. Global status report on alcohol. Geneva: World Health Organization. 1999 [Google Scholar]
[3]. Bray I, Brennan P, Boffetta P, Projections of alcohol- and tobacco related cancer mortality in Central EuropeInt J Cancer 2000 87:122-28. [Google Scholar]
[4]. Al-Haqwi AI, Tamim H, Asery A, Knowledge, attitude and practice of tobacco smoking by medical students in Riyadh, Saudi ArabiaAnn Thorac Med 2010 5:145-8. [Google Scholar]
[5]. Warren CW, Jones NR, Peruga A, Chauvin J, Baptiste JP, Costa de Silva V, Global youth tobacco surveillance, 2000-2007MMWR Surveill Summ 2008 57:1-28. [Google Scholar]
[6]. (10 Facts on Physical Activity)http://www.who.int/features/factfiles/physical_activity/facts/en/index.html(03.04.2013) [Google Scholar]
[7]. World Health Organization, Geneva. Global health risks. 2009; mortality and burden of disease attributable to selected major risks [Google Scholar]
[8]. Wipfli H, Samet JM, Global economic and health benefits of tobacco control: part 1Clin Pharmacol Ther 2009 86(3):263-71. [Google Scholar]
[9]. WHO: Problems related to alcohol consumption Technical Report Series. 1980; 7: 650, 10-16 [Google Scholar]
[10]. World Health Organization/ EMRO. Questionnaire for Regional Situation Analysis on Drug Abuse. 2003; Cairo, WHO Regional Office for the Eastern Mediterranean [Google Scholar]
[11]. World Health Organization. The world health report 2002—reducing risks, promoting healthy life. Geneva: World Health Organization. p. 250 [Google Scholar]
[12]. World Health Organization Global status report. 2004: alcohol policy. Geneva: Department of Mental Health and Substance Abuse, World Health Organization. p. 209 [Google Scholar]
[13]. International Agency for Research on CancerAlcohol drinkingIARC monographs on the evaluation of carcinogenic risks to humans 1988 vol 44LyonIARC [Google Scholar]
[14]. Ng SK, Kabat GC, Wynder EL, Oral cavity cancer in non-users of tobaccoJ Natl Cancer Inst 1993 85:743-45. [Google Scholar]
[15]. Bosetti C, Gallus S, Franceschi S, Cancer of the larynx in nonsmoking alcohol drinkers and in non-drinking tobacco smokersBr J Cancer 2002 87:516-18. [Google Scholar]
[16]. Blot WJ, McLaughlin JK, Winn DM, Austin DF, Greenberg RS, Preston-Martin S, Smoking and drinking in relation to oral and pharyngeal cancerCancer Res 1988 48:3282 [Google Scholar]
[17]. Waddell WJ, Levy PS, Interaction between tobacco and alcohol consumption and the risk of cancers of the upper aero-digestive tract in BrazilAm J Epidemiol 2000 152:193-4. [Google Scholar]
[18]. World Health Organization. Global status report on alcohol and health. 2011; World Health Organization. [Google Scholar]
[19]. Al-Turki KA A-BN, Al-Ghamdi AJ, El-Zubaier AG, Al-Ghamdi R, Alameer MM, East Mediterr Health 2010 16(6):671-6.PMID: 20799597 [Google Scholar]
[20]. Al-Nahedh N, Relapse among substance-abuse patients in Riyadh, Saudi ArabiaEastern Mediterranean Health Journal 1999 5(2):241-46. [Google Scholar]
[21]. Amir T, Comparison of patterns of substance abuse in Saudi Arabia and the United Arab EmiratesSocial Behaviour and Personality 2001 29(6):519-30. [Google Scholar]
[22]. Alcohol per capita consumption, patterns of drinking and abstention worldwide after 1995. Appendix. 2European Addiction Research 2001 7(3):155-57. [Google Scholar]
[23]. Hawwari A, Getting a drink in Saudi ArabiaBBC News Online 2001; 8 February [Google Scholar]