Water Borne Hepatitis A and Hepatitis E in Malwa Region of Punjab, India
Deepak Arora1, Neerja Jindal2, Ravinder K Shukla3, Renu Bansal4
1 Associate Professor, Department of Microbiology, G.G.S Medical College, Faridkot Punjab, India.
2 Professor & Head, Department of Microbiology, G.G.S Medical College, Faridkot Punjab, India.
3 Controller of Examination, BFUHS, Faridkot Punjab, India.
4 Associate Professor, Department of Microbiology, G.G.S Medical College, Faridkot Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepak Arora, Associate Professor, Department of Microbiology, G.G.S Medical College, Faridkot Punjab, India. Mobile: 09781566786, Email: drdeepakarora78@gmail.com
Introduction: Hepatitis-A virus infection (HAV) and Hepatitis E virus infection (HEV) are faecally contaminated water borne infection of great public interest in developing countries. HAV has a world-wide /dablestribution and affects infant and young children in developing countries and its epidemics are not very common. HEV is restricted to tropical countries and affects older children and young adults and its epidemics are common. Studies suggested that HEV is etiologically responsible for 10%–95% of admitted cases of hepatitis. Exposure rates over a period of time are different in different parts of the country and in different socio-economic groups.
Aim of the study 1. To study the prevalence of HAV and HEV in the outbreak of hepatitis in certain areas of Malwa region of Punjab, India.
2. To determine the age specific prevalence rates of HAV and HEV.
3. To determine any change in the epidemiology of these infections.
Material and Methods: This study was conducted in the Department of Microbiology in GGMC and Hospital Faridkot, A leading Tertiary care hospital and the major referral centre of malwa region of Punjab,India.
Collection and Serological Tests: 1.Venous blood samples of patients of acute hepatitis were taken.
2.Relavent information regarding their Age, Sex Education, Socio-economic status, personal and community hygiene were recorded. All of the sera were screened for IgM Antibody to HEV and HAV using IgM capture ELISA Kit (ASIA-LION Biotechnology for HEV and GENERAL BIOLOGICAL CORPORATION for HAV ) in accordance with the manufacturer’s instructions.
Result and Conclusion : 1.The outbreak was due to hepatitis A &E virus(HEV predominating resulting from fecal contamination of drinking water). 2.Hepatitis E is more widely prevalent 3.There is a change in the epidemiology of HAV so,more cases are seen in age group of more than 20 years.
Infections, Punjab, Hepatitis, Water
Introduction
Hepatitis-A virus infection (HAV) and Hepatitis E virus infection (HEV) are enterically transmitted viral diseases of great public health importance in the developing countries like India. HAV has a world-wide distribution and affects infants and young children in developing countries but its epidemics are rare; whereas HEV is restricted to tropical countries and affects older children and young adults and its epidemics are common [1–2]. In developing countries like India, HAV and HEV both are endemic. Exposure rates over a period of time are different in different parts of the country and in different socio-economic groups [1]. Hepatitis E virus (HEV), an emerging pathogen [3,4], causes significant disease in endemic countries and is the leading cause of enterically transmitted viral hepatitis illness globally [3]. Large annual epidemics are attributed to HEV [5], and studies suggested that HEV is etiologically responsible for 10%–95% of admitted cases of hepatitis across South Asia [6,7]. Globally, prevalence rates of antibody to Hepatitis-E virus (anti-HEV) vary by region, population, and circulating genotypes of HEV, with unexpectedly high seropositivity in some developed settings [8,9]. It is unknown why age-specific seroprevalence rates of HAV and HEV are dissimilar in the same country and why antibody acquisition rates are different in different countries with similar environmental conditions.
HAV has a world-wide distribution and affects infant and young children in developing countries and its epidemics are not very common.
Acute infection primarily affects young adults and is generally mild, except in women during late pregnancy, among whom 20% mortality has been reported [10]. HEV infection usually does not become chronic, but chronic infections have recently been reported in transplant recipients [10].
HEV infection in pregnant women is more common and more fatal in the third trimester. The mortality rate due to HEV-induced hepatitis is as high as 15-20% [10].
Aim and Objectives
To study the prevalence of HAV and HEV in the outbreak of hepatitis in certain areas of Malwa region of Punjab,India .
To determine the age specific prevalence rates of HAV and HEV.
To determine any change in the epidemiology of these infections.
Material and Methods
This study was conducted in the Department of Microbiology in GGMC and Hospital Faridkot, which is the centre for Intergerated Disease Surveillance Programme (IDSP) receiving samples from surrounding areas too. During 2011 there was an outbreak of water borne hepatitis in Bathinda,India and the samples were send to GGMC Faridkot for testing . Detailed history about the areas with the maximum number of cases, their presenting complaints and other relevant history was taken from Civil Hospital Bathinda, India”.
In 2012, because of the preventive measures taken after the outbreak, (nil) cases were reported proving the preventable nature of the disease.
Collection and Serological Tests
Venous blood samples of patients of acute hepatitis were taken.
All of the sera were screened for IgM Antibody to HEV and HAV by using IgM capture ELISA Kit (Asia-Lion Biotechnology for HEV and GENERAL BIOLOGICAL CORPORATION for HAV ) in accordance with the manufacturer’s instructions.
Results
The serum samples of 81 patients of jaundice and hepatitis were diagnosed with HAV and HEV infection by demonstrating the IgM antibody by capture by Elisa.
Most of the patients presented within one week of onset of symptoms to the hospital with the major presenting complaints of Pain abdomen, fever ,vomiting, jaundice and fatigue.
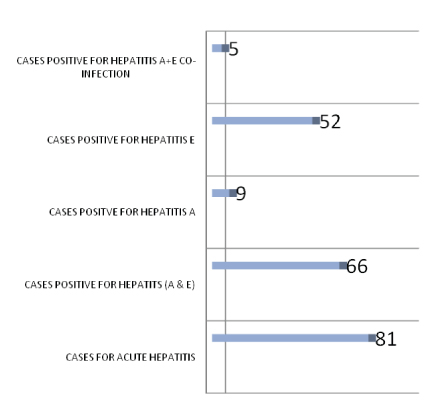
Total 81 cases of acute hepatitis were reported out of which 66(81.48%) cases were positive for Hepatitis A and E [Table/Fig-1]. Nine cases (13.63 %) were positive for Hepatitis-A [Table/Fig-1] , 52 cases(78.78%) were positive for Hepatitis-E [Table/Fig-1] and 5 cases (7.5%) were positive for Hepatitis -A+ E co-infection [Table/Fig-1].
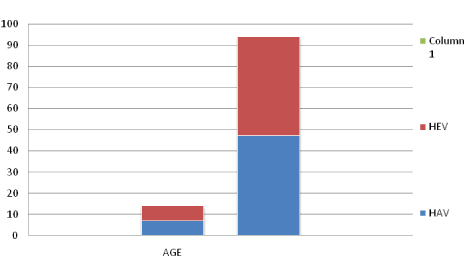
Of the 14(9+5) patients of HAV infection 7(50%) were in the age group≥ 20 years and 7(50%) were in the age group of ≤20 years . Of the 57{52+5} patients of HEV 10(17.54%) were in the age group of≥ 20 and rest 47(82.45%) were in the age group of ≤20 yrs. as shown in [Table/Fig-2].
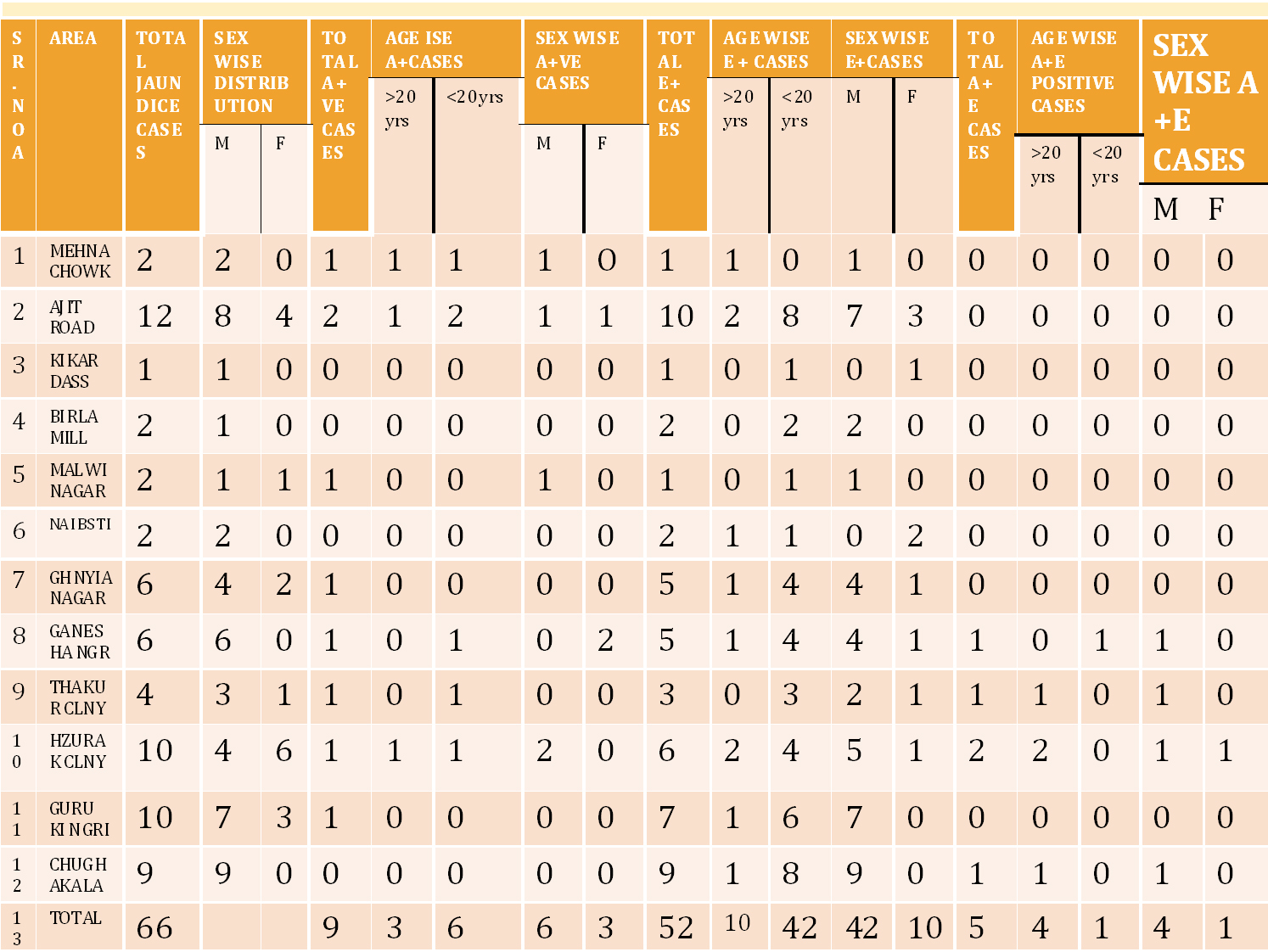
Out of 9 HAV positive cases Males were 6( 9.09%)and 3(4.54%) were females , of the 52 cases of HEV 42(63.63%) were males and 10(15.15%) were female . Of the 5 cases with co-infection of HAV and HEV 4( 6.06%) were males and 1(1.5%) was female as shown in [Table/Fig-3].
Showing positive cases of hepatitis a, e & co-infection (a+e)
(HAV) & 3(HEV) Age wise distribution of cases
Area wise distribution of cases
Discussion
India is considered to be a hyper endemic region for HAV [11]. In the present population-based study, prevalence of HAV is 13.63% as compared to 81.48% of total prevalence as shown in [Table/Fig-1]. In the present study, the trend of the decrease in the prevalence was in accordance with shifting patterns of sero-prevalence over the past 20 years seen in South-east Asia and China that reflected improved living standards and environmental hygiene [12–14].
However many recent reports indicate a global change in sero-epidemiological patterns of hepatitis A infection [15]. In Delhi (India), sero prevalence in people younger than 35-year–old was similar to that of the more developed European countries and in many Western European countries [16], followed by the improvement of the standard of living in the industrialized world,
HAV seroprevalence remained high in all age groups and changed under the age of five years old. This finding confirmed that the greatest exposure still occurs early in life and that individuals acquire HAV immunity at a very young age, but these findings are not correlating with us as in our case out of the 14 cases of HAV 7 are in age group of >20year and 7 cases are in age group of <20 years as shown in [Table/Fig-2].
Regarding socio-demographic variables, our findings are consistent with several previous studies showing a clear inverse correlation between exposure to HAV and socio-economic level [17–19]. It is a well known fact that HAV infection is strongly correlated with poverty and inadequate sanitation. Increasing household income, education, water quality and quantity, sanitation, and hygiene lead to decreased HAV prevalence. Indeed, the prevalence of HAV infection could even be used as an index of the level of development in a given country. Prevalence of the disease varies widely, as a consequence of basic sanitation conditions. The maximum number of cases which are found in our study were from underdeveloped area of Bathinda,India as shown in [Table/Fig-3].
Hepatitis-A virus (HAV) is a health problem in countries where sero-epidemiology shows changes from hyperendemicity to intermediate endemicity [20]. Then,there are different patterns with pockets of low prevalence; some studies indicate a decline of anti-HAV prevalence and the possibility of an outbreak of HAV infection among this population.
HEV mainly affects young adults of 15-40 years of age and relatively spares children [21]. In India, HEV is responsible for 50-70% of all cases of sporadic acute viral hepatitis [22,23], and also, is responsible for large outbreaks with source of infection mainly being contaminated water supplies [21]. The occurrence of large epidemics of HEV in disease-endemic areas, as it was the case in the present study, suggests the possibility of doubtful protection from the antibody, gradual decline in the protective level of the antibody or infection from divergent strains of the virus [21].
In most disease-endemic areas like India, HEV seroprevalence is high in the population under the age of 10, it is less ,but increases up to 30 % among adults > 25 years of age [1]. The results of the present epidemiological study showed the presence of an overall high endemicity of HEV infection (78.78 %) as shown in [Table/Fig-1]. and a significantly lower seroprevalence in the age groups <10 years and <50 years. Compared to other series, the higher rate of HEV seroprevalence in the population under the age of 10 was seen from Andaman-Nicobar (32.9%) [12] and in one from Northern India (>60%) [24]. This was in sharp contrast to our studies as in our study as maximum no.of cases out of 57, 47(82.45%) of the cases are found in age group of more than 20 years as shown in [Table/Fig-2]. These differences might be due to either varying environmental conditions in different geographical areas or the differences in the diagnostic tests used.
Another, important finding which we got was the 5(7.5%) cases out of the total 66 cases of hepatitis were the patients with co-infection of HAV+HEV [Table/Fig-1].Out of these 5 patients of co-infection of HAV and HEV 4 (80%)are in age group of less than 20 and only 1(20%) is in age group of more than 20 .This, is the paradoxical finding as in case of HEV positive cases. Out of 57, 47(82.45%) were in age group of more than 20 years and also against the finding of Parana R et al., [25] as study by them states that Patients with acute viral hepatitis due to hepatitis A also have high frequency of anti-HEV, probably because of similar routes of transmission for hepatitis A and E viruses This finding also supports the that HEV is encountered early in childhood as HAV infection.
Although the major route of transmission of HAV and HEV is feco-oral route and poor sanitation and contaminated food/water supplies are frequently cited as a source of infection; changes in exposure rates of HAV and HEV in all age groups suggest either a difference in mode of transmission. A difference in the characteristics of virus (virulence-infectivity/ viability/ transmissibility) or a difference in sensitivities and concordance rates of various anti-HEV assays [2,21]. Sex wise distribution show that males incidence of HAV,HEV and HEV+HEV co-infection were more as shown in [Table/Fig-4].This can might be because major route of transmission of HAV and HEV is feco-oral route and poor sanitation and contaminated food/water supplies and as male go out more for work ,so chances of eating outside also increases as shown by other studies [22,23,26].
| Male | Female | %Age |
|---|
| HAV | 6 | 3 | 9 |
| HEV | 42 | 10 | 52 |
| HAV+HEV | 4 | 1 | 5 |
| TOTAL NO. OF CASES POSITIVE | 52(78.78) | 14(21.21) | 66 |
Conclusion
Even though sample size is less but, it will definitely act as the eye opener because at present, there is no system available which can track the quality of water supplied to the population. The situation is just like a tip of iceberg.
IN 2012, as nil cases were reported after the outbreak of 2011 thus, showing the preventable nature of the disease. So, in this situation, it is necessary to keep water supply free from fecal contamination to prevent outbreak of water borne diseases.
[1]. Arankalle VA, Chadha MS, Chitambar SD, Walimbe AM, Chobe LP, Gandhe SS, Changing epidemiology of Hepatitis A and Hepatitis E in urban and rural India (1982-98)J Viral Hepat 2001 8(4):293-303. [Google Scholar]
[2]. Emerson SU, Purcell RH, Running like water--the omnipresence of hepatitis EN Engl J Med 2004 351(23):2367-8. [Google Scholar]
[3]. Balayan MS, Andjaparidze AG, Savinskaya SS, Braginsky DM, Savinov AP, Poleschuk VF, Evidence for a virus in non-A, non-B hepatitis transmitted via the fecal-oral routeIntervirology 1983 20(1):23-31. [Google Scholar]
[4]. Reyes GR, Purdy MA, Kim JP, Luk KC, Young LM, Fry KE, Isolation of a cDNA from the virus responsible for enterically transmitted non-A, non-B hepatitisScience 1990 247(4948):1335-39. [Google Scholar]
[5]. Labrique AB, Thomas DL, Stoszek SK, Hepatitis E: an emerging infectious diseaseEpidemiol Rev 1999 21(2):162-79. [Google Scholar]
[6]. Sheikh A, Sugitani M, Kinukawa N, Hepatitis E virus infection in fulminant hepatitis patients and an apparently healthy population in BangladeshAm J Trop Med Hyg 2002 66(6):721-24. [Google Scholar]
[7]. Acharya SK, Panda SK, Saxena A, Acute hepatic failure in India: a perspective from the EastJ Gastroenterol Hepatol 2000 15(5):473-79. [Google Scholar]
[8]. Abe K, Li TC, Ding X, International collaborative survey on epidemiology of hepatitis E virus in 11 countriesSoutheast Asian J Trop Med Public Health 2006 37(1):90-95. [Google Scholar]
[9]. Kuniholm MH, Purcell RH, McQuillan GM, Epidemiology of hepatitis E virus in the United States: results from the Third National Health and Nutrition Examination Survey, 1988–1994J Infect Dis 2009 200(1):48-56. [Google Scholar]
[10]. Kamar N, Selves J, Mansuy JM, Ouezzani L, Péron JM, Guitard J, Cointault O, Esposito L, Abravanel F, Danjoux M, Hepatitis E virus and chronic hepatitis in organ-transplant recipientsN Engl J Med 2008 358:811-17. [Google Scholar]
[11]. Tandon BN, Gandhi BM, Joshi YK, Etiological spectrum of viral hepatitis and prevalence of markers of Hepatitis-A and B virus infection in North IndiaBull World Health Organ 1984 62(1):67-73. [Google Scholar]
[12]. Murhekar MV, Sehgal SC, Murhekar KM, Padbhidri SP, Chitambar SD, Arankalle VA, Changing scenario of Hepatitis-A virus and Hepatitis-E virus exposure among the primitive tribes of Andaman and Nicobar Islands, India over the 10-year period 1989-99J Viral Hepat 2002 9(4):315-21. [Google Scholar]
[13]. Acharya SK, Batra Y, Bhatkal B, Sero-epidemiology of Hepatitis-A virus infection among school children in Delhi and North Indian patients with chronic liver disease: implications for HAV vaccinationJ Gastroenterol Hepatol 2003 18(7):822-27. [Google Scholar]
[14]. Barzaga BN, Hepatitis A shifting epidemiology in South-East Asia and ChinaVaccine 2000 18(Suppl 1):S61-4. [Google Scholar]
[15]. Ratanasuwan W, Sonji A, Tiengrim S, Techasathit W, Suwanagool S, Serological survey of viral Hepatitis-A, B, and C at Thai Central Region and BangkokSoutheast Asian. J Trop Med Public Health 2004 35(2):416-20. [Google Scholar]
[16]. Francesco C, Giampiero C, Travelers Age-Specific Anti-Hepatitis A Virus Sero epidemiology in Italian Travelers Indications for Anti-Hepatitis A VaccinationTravel Med 1996 3:214-18. [Google Scholar]
[17]. Zago MP, Stantolin GC, Perazzio S, Prevalence of antihepatitis A antibodies in children of different socioeconomic conditions in Vila VelhaRev Soc bras Med trop 2005 38:285-89. [Google Scholar]
[18]. Pereira FE, Gonçalves SC, Hepatite ARev Soc bras Med trop 2003 36:387-400. [Google Scholar]
[19]. Raharimanga V, Carod JF, Ramarokoto CE, Chrétien JB, Rakotomanana F, Talarmin A, Richard V, Age-specific seroprevalence of hepatitis A in Antananarivo (Madagascar)BMC Infect Dis 2008 Jun 6 8:78 [Google Scholar]
[20]. Letaief A, Kaabia N, Gaha R, Bousaadia A, Lazrag F, Trabelsi H, Age-specific seroprevalence of hepatitis a among school children in central TunisiaAm J Trop Med Hyg 2005, July 73(1):40-43. [Google Scholar]
[21]. Aggarwal R, Krawczynski K, Hepatitis E.An overview and recent advances in clinical and laboratory researchJ Gastroenterol Hepatol 2000 15(1):9-20. [Google Scholar]
[22]. Khuroo MS, Rustgi VK, Dawson GJ, Spectrum of hepatitis E virus infection in IndiaJ Med Virol 1994 43(3):281-6. [Google Scholar]
[23]. Amarapurkar DS, Agar Baijal P, Gupte P, Kamani N, Epidemiology of Hepatitis E Virus Infection in Western IndiaJournal of Hepatic Monthly Original Article Volume: 8 2008 8(4):258-62. [Google Scholar]
[24]. Aggarwal R, Shahi H, Naik S, Yachha SK, Naik SR, Evidence in favour of high infection rate with hepatitis E virus among young children in IndiaJ Hepatol 1997 6(6):1425-6. [Google Scholar]
[25]. Parana R, Cotrim HP, Cortey-Boennec ML, Trepo C, Lyra L, Prevalence of Hepatitis E virus IgG antibodies in patients from a referral unit of liver diseases in Salvador, BrazilAm J Trop Med Hyg 1997 57:60-1. [Google Scholar]
[26]. Rao P, Shenoy SM, Baliga S, Joon A, Prevalence of HAV and HEV in the patients presenting with acute viral hepatitisBMC Infectious Diseases 2012 12(Suppl 1):1471-2334-12-S1-P30. [Google Scholar]