Enteric Parasitic Infections in Relation to Diarrhoea in HIV Infected Individuals with CD4 T Cell Counts <1000 Cells/μl in Chennai, India
Anand B. Janagond1, G. Sasikala2, David Agatha3, Thyagarajan Ravinder4, P. R. Thenmozhivalli5
1 Assistant Professor, Department of Microbiology, Sri Muthkumaran Medical College, Chennai, India.
2 Assistant Professor, Department of Microbiology, Vinayaka Mission’s Kirupananda Variyar Medical College, Salem, India.
3 Assistant Professor, Department of Microbiology, Madras Medical College, Chennai, India.
4 Professor and Head, Department of Microbiology, Kilpauk Medical College, Chennai, India.
5 Dean, former Professor, Department of Microbiology, Chengalpattu Government Medical College, Chengalpattu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anand B Janagond, Assistant Professor, Department of Microbiology, Sri Muthukumaran Medical College, Chikkarayapuram, Chennai – 600 069 Tamil Nadu, India.
Phone: +91-98841 61551,
E-mail: anandbj@gmail.com
Aim: This study was conducted to estimate the prevalence of enteric parasites in HIV patients in Chennai and to correlate with CD4 counts and diarrhoeal status.
Material and Methods: Faecal specimens from 100 HIV infected individuals with CD4 < 1000/μl were screened for enteric parasites with wet mounts, modified acid-fast stain for coccidian parasites, modified trichrome stain for Microsporidia, before and after the stool concentration. Agar plate culture for Strongyloides was put up. Chi-square and ANOVA tests were used for statistical analysis.
Results: Study group comprised of 38 subjects with acute diarrhoea, 30 with chronic diarrhoea (> 2 weeks) and remaining 32 without diarrhoea. Enteric parasites were detected in 33% of subjects; Isoapora belli (21) being the commonest followed by E.histolyt/Entamoeba dispar (5), Entamoeba coli (2), Cryptosporidium spp (2), Hookworms (2), Strongyloides stercoralis (2), Giardia lamblia (1) and Microsporidium spp (1). There was a significant inverse relation between CD4 counts and duration of diarrhoea. Opportunistic parasites were isolated from the subjects with wide range of CD4 counts and different diarrhoeal status but most commonly from chronic diarrhoea patients.
Conclusion: The prevalence of intestinal parasitic infections in HIV patients is high in Chennai, India, especially at CD4 <1000/μl, I.belli infection being the commonest. Routine screening of all HIV patients with low CD4 counts for coccidian parasitic infections by using simple stool microscopic techniques can help in early diagnosis and treatment.
Enteric Parasites, HIV, Diarrhoea, CD4 T cell count, Isospora belli
Introduction
Parasites cause diarrhoea in almost 90% of the patients with Human Immunodeficiency Virus (HIV) infection in developing countries [1,2]. Diarrhoea is associated with weight loss and is often presenting illness of HIV-infected individuals. This diarrhoea wasting syndrome, in association with positive HIV serology test, is Acquired Immunodeficiency Syndrome (AIDS) defining illness in WHO’s classification [3].
Opportunistic coccidian parasites, Cryptosporidium parvum, Isospora belli, Cyclospora cayetanensis, and Microsporidia are important causes of chronic diarrhoea, which are associated with weight loss, in patients with HIV/AIDS. Endemicity of a particular enteric parasite in the community is likely to govern the incidence and prevalence of a particular parasitic infection in persons with HIV/AIDS [4].
The clinical course and pattern of opportunistic infections vary from patient to patient in different geographical areas of India. As the prevalence and spectrum of parasites causing opportunistic infections in a place can keep changing with time, studies to monitor the trend are useful. Opportunistic intestinal parasitic infections should be suspected in any HIV-infected patient with advanced disease presenting with diarrhoea. CD4 cell counts have been significantly lower in these individuals with diarrhoea than in those who are without [5].
The present study was undertaken to detect the intestinal parasites in HIV patients in Chennai, India and also to correlate with diarrhoeal status and CD4 T-cell counts. In this study, an attempt has been made to incorporate more sensitive techniques of detecting coccidian parasites such as formalin ether sedimentation concentration technique for all the specimens, agar plate culture method for Strongyloides stercoralis, modified trichrome stain for Microsporidia and also Lactophenol cotton blue wet mount in addition to usual saline and iodine wet preparations.
Material and Methods
This study was conducted after getting hospital ethical committee approval at public tertiary care hospitals in Chennai during January 2008 to June 2009. Hundred HIV seropositive individuals with CD4 T cell counts (estimated by BD FACS Calibur) less than 1000 cells/μl were randomly chosen and relevant clinical history was collected. Patients who had received antiprotozoals or anthelmintics in the past 1 month were excluded from the study. Most subjects were receiving HAART, and Cotrimoxazole Prophylaxis for Pneumocystis jirovecii.
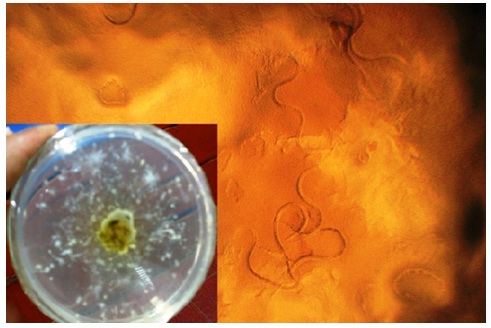
Three fresh faecal specimens were collected from each subject and were processed within 2 hours. All the specimens were subjected to wet mount Pneumocystis jirovecii using saline, iodine and lactophenol cotton-blue (LCB) [6,7]. Dry faecal smears were prepared and subjected to modified acid-fast staining (with 1% sulphuric acid as decolorizer) for coccidian parasites and Weber’s modification of trichrome stain for Microsporidia. All these microscopic techniques were repeated after concentrating the specimens by Formalin Ether concentration method. Agar plate culture [Table/Fig-1] was put up for all fresh specimens to detect Strongyloides spp. [8]. Statistical analysis was done using chi-square and ANOVA tests. Differences in the p-values which were <0.05 were considered as significant at 95% confidence intervals.
Strongyloides larvae in Agar plate culture (400x). Faecal inoculum at the centre surrounded by track marks formed by larvae inset)
Results
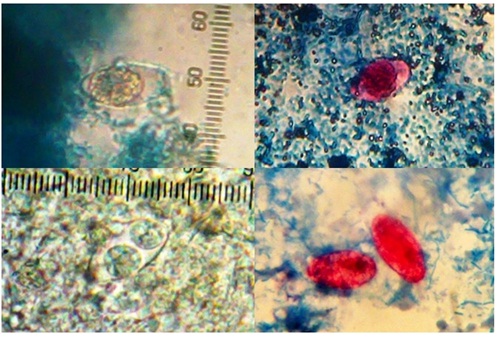
Study group comprised HIV seropositive individuals of whom 38 subjects were with acute diarrhoea, 30 with chronic diarrhoea (> 2 weeks) [5] and remaining 32 without diarrhoea. Thirty six parasites were detected from 33 subjects with the overall rate of enteric parasitic infection in the study group being 33% (33/100).Three subjects had simultaneous infection by two parasites (I. belli with E. histolytica, I. belli with Cryptosporidium spp. and I. belli with Strongyloides spp.). The parasites detected comprised of I. belli [Table/Fig-2] (21), E.histolytica /Entamoeba dispar (5), Entamoeba coli (2), Cryptosporidium spp (2), Hookworms (2), Strongyloides stercoralis (2), Giardia lamblia (1) and Microsporidium spp (1). Prevalence of infections were significantly varying in subjects with different diarrhoeal status [Table/Fig-3]; highest being in those with chronic diarrhoea (16/30; 53.33%) followed by those with acute diarrhoea (13/38; 34.21%) and without diarrhoea (4/32; 12.5%). CD4 counts ranged from 10 – 906 cells/μl. Mean CD4 counts were also significantly different (One-way ANOVA, p <0.05) in those without diarrhoea (319.93), with acute (239.26) and chronic diarrhoea (179.10); lowest among chronic diarrhoea patients [Table/Fig-4].
Isospora belli ;(Clockwise from top left) Immature oocyst (Lactophenol cotton blue), Immature oocyst (Acid-fast stain), Mature oocyst (Saline wet mount) and Oocysts with disintegrated sporocyst
Prevalence of parasites in HIV patients with different diarrhoeal status and mean CD4 T-cell counts
| Parasites and CD4 T cell counts | Diarrhoeal status of HIV patients | Total | p-value & significance |
|---|
| Without diarrhoea (n=32) | Acute diarrhoea (n=38) | Chronic diarrhoea (n=30) |
|---|
| Total parasitic infections | 4 (12.50%) | 13 (34.21%) | 16 (53.33%) | 33 | p<0.05, significant@ |
| Isospora belli | 2(6.25%) | 7 (18.42%) | 12 (40%) | 21 | p<0.05, significant# |
| Mean CD4 counts (cells/μl) | 320 | 239 | 179 | – | p<0.05, significant* |
@Total parasites: X2=11.717, p=0.02 (< 0.05)
#Isospora belli: X2=10.877, p=0.043 (<0.05)
*Mean CD4 counts: One way ANOVA, p=0.011 (<0.05)
Parasitic infection and CD4 T cell counts in HIV patients
| Parasites | CD4 T-cell counts (cells/μl) | Total | p-value & significance |
|---|
| <200 (n=48) | 200-499 (n=23) | 500-1000 (n=29) |
|---|
| Total parasitic infections | 19 (39.58%) | 8 (34.78%) | 6 (20.69%) | 33 | p>0.05, not significant# |
| Opportunistic parasites | 18 (37.50%) | 5 (21.74%) | 3 (10.34%) | 26 | p<0.05, significant@ |
| Isospora belli | 13 (27.08%) | 5 (21.74%) | 3 (10.34%) | 21 | p>0.05, not significant* |
# Total parasites: X2=2.962, p=0.227 (>0.05)
@ Opportunistic parasites: X2=7.211, p=0.027 (<0.05)
*Isospora belli: X2=3.063, p=0.216 (>0.05)
Prevalence of enteric parasitic infection was highest among those with CD4 <200/μl (19/48; 39.58%) compared to those with CD4 T cells 201 – 500/μl (8/23; 34.78%) and 501-1000/μl (6/29; 20.69%) but the difference was statistically not significant. I. belli was the commonest (63%) parasite detected. I.belli was seen in subjects with a wide range of CD4 counts and the difference in the prevalences among different CD4 ranges was not statistically significant. I. belli was isolated significantly (p 0.012, chi-square test) more from (12/30; 40%) chronic diarrhoea, followed by acute diarrhoea (18.42%; 7/38) and in apparently normal subjects (6.25%; 2/32). Nine out of 21 patients (42.86%) with Isosporiasis were on cotrimoxazole prophylactic therapy for P. jeerovecii infection. Cryptosporidium spp, S. stercoralis and Microsporidium spp were detected in persons with CD4 T cells < 200/μl only.
Discussion
HIV infection causes progressive damage to both limbs of the immune system, which results in a plethora of opportunistic infections [4]. Opportunistic spore forming protozoan parasites such as I. belli, C. parvum, C. cayetanensis and Microsporidia play major role in causing chronic diarrhoea, accompanied with weight loss in them. Endemicity of a particular enteric parasite in the community is likely to govern the incidence and prevalence of a particular parasitic infection in HIV/AIDS [4]. Early detection of parasitic infections is essential to reduce the morbidity and mortality.
Studies have shown regional diversity in CD4 counts in healthy young adults. The mean CD4 T cell counts in South Indian healthy adults has been reported to be 931 – 1048 cells/μl [9,10]. CD4-T cell counts are considered as surrogate markers of immune status of an individual [10]. In the early stage of HIV infection, individuals are known to have normal CD4 counts, are not immunocompromised and hence are not prone for opportunistic infections. The present study was aimed at studying the enteric parasitic infections in HIV patients with less than normal CD4 counts. Overall prevalence was found to be 33% for enteric infections. The prevalence of coccidian parasites was 24%. Protozoan infections (32) outnumbered helminth infections (4). Isospora belli was the commonest parasite detected irrespective of diarrhoeal status and CD4 counts in this study, though it was significantly more common in chronic diarrhoea. In North and Western parts of India Cryptosporidium is the commonest intestinal parasite among HIV-infected individuals [1,4,11]. A study conducted in Southern Tamil Nadu (Thirunelveli) also found Cryptosporidium as the commonest parasite among HIV patients (14). Higher prevalence of Isospora compared to other parasites among HIV infected patients in Northern Tamil Nadu (Chennai, Vellore) has been documented by studies conducted by Kumar SS et al., (14%), Vignesh R et al., (26.1%) and Mukhopadhya et al., [2,12,13]. Vignesh R et al., have found a statistically significant increase in Isospora belli and a decrease in number of Cryptosporidial infections in HIV patients in Chennai during 2003-2006. Changes in the trend with time was hypothesized to be due to changes in residence, patient population and weather conditions (rainfall and temperature) [12]. A wide variation in the spectrum of opportunistic parasites in HIV patients with respect to geographical areas and time emphasises the need for more studies to monitor their prevalence and changing trends.
Prevalence of Cryptosporidium (2%) and Microsporidia (1%) was low. Cyclospora was not detected in our subjects. These can be attributed to varying geographical distributions of the parasites. In spite of using more sensitive agar plate culture method in our study, Strongyloides infection was found to be low (2%).
In our study, CD4 T-cell counts were inversely proportional to the duration of diarrhoea. With decreasing CD4 counts, patients suffered from diarrhoea for longer duration. Unlike in other studies, in this study inverse relation between CD4 counts and prevalence of parasites, including I. belli was not significant. This might be because, all subjects had low CD4 counts (<1000/μl) and sample size was small. Multiple parasitic infections and infections by Cryptosporidium, Strongyloides spp. were seen only in subjects with CD4 counts <200/μl in our study. This may be because immunodeficient patients are either more susceptible to acquire particular parasites and/or are unable to clear them once acquired [5].
Carriage of opportunistic parasites was seen in 12.5% (4/32) asymptomatic subjects. Asymptomatic carriage can cause active disease in the same person in future if immunity is lowered and is also a source of infection to community. This necessitates routine screening of all HIV-infected individuals for early detection of enteric parasites and initiation of specific treatment.
LCB wet preparations in addition to usual saline and iodine wet mounts for ova/cyst identification did not increase sensitivity of parasite detection. Since LCB mounts did not dry as quickly as the other wet mounts, they could be examined leisurely and preserved for a few days for second opinion or teaching purposes.
Diarrhoea associated with Isospora infection is often self-limited in immunocompetent hosts but may be prolonged in immunocompromised individuals. Treatment for Isosporiasis is cotrimoxazole and higher doses need to be used in patients with AIDS [14]. Though cotrimoxazole is one of the preferred drugs for coccidian parasitic infections, prophylactic doses of the same targeted for Pneumocystis pneumonia does not seem to effectively prevent coccidian parasitic infections. Other reasons for poor outcome for Cotrimoxazole might be decreased bioavailability due to enteropathy or low patient compliance. In patients allergic to sulfonamides, pyrimethamine alone is given as treatment. In HIV /AIDS patients with recurrent-to-persistent infection, the therapy must be continued indefinitely [12,14]. Prevention of isosporiasis is possible with improved personal hygiene measures and sanitary conditions, to eliminate possible faecal-oral transmission from contaminated food, water, and possible environmental surfaces [8].
Since a limited study population was screened, the present study provides preliminary data for further evaluation using a longitudinal study with a larger sample size.
Conclusion
The prevalence of intestinal parasitic infections in HIV patients remains high in this region, especially at CD4 <1000/μl. I.belli infection should be primarily suspected in HIV patients in Chennai having chronic diarrhoea and low CD4 counts. Duration of diarrhoea is likely to be longer in HIV patients as the CD4 cell counts decrease. Routine screening of all the HIV patients with low CD4 counts for coccidian parasitic infections by using simple stool microscopic techniques can help in early diagnosis, initiation of appropriate treatment and control of spread.
@Total parasites: X2=11.717, p=0.02 (< 0.05)
#Isospora belli: X2=10.877, p=0.043 (<0.05)
*Mean CD4 counts: One way ANOVA, p=0.011 (<0.05)
# Total parasites: X2=2.962, p=0.227 (>0.05)
@ Opportunistic parasites: X2=7.211, p=0.027 (<0.05)
*Isospora belli: X2=3.063, p=0.216 (>0.05)
[1]. Mamatha B, Rao AS, Asish PR, Opportunistic intestinal protozoal infections in HIV infected patients in a rural cohort population in Manipal, Karnataka (S. India)Indian J Pathol Microbiol 2005 48:287-8. [Google Scholar]
[2]. Kumar SS, Ananthan S, Lakshmi P, Intestinal parasitic infections in HIV infected patients with diarrhoea in ChennaiIndian J Med Microbiol 2002 20:88-91. [Google Scholar]
[3]. Pape JW, Verdier RI, Boncy M, Boncy J, Johnson WD Jr, Cyclospora infection in adults infected with HIV: Clinical manifestations, treatment and prophylaxisAnn Intern Med 1994 121:654-7. [Google Scholar]
[4]. Chawla R, Ichhpujani RL, Enteric spore-forming opportunistic parasites in HIV/AIDSTrop parasitol 2012 1:15-9. [Google Scholar]
[5]. Assefa S, Erko B, Medhin G, Assefa Z, Shimelis T, Intestinal parasitic infections in relation to HIV/AIDS status, diarrhoea and CD4 T-cell countBMC Infect Dis 2009 9:155 [Google Scholar]
[6]. Parija SC, Shivaprakash MR, Jayakeerthi SR, Evaluation of lacto-phenol cotton blue (LPCB) for detection of Cryptosporidium, Cyclospora and Isospora in the wet mount preparation of stoolActa Trop 2003 85:349-54. [Google Scholar]
[7]. Parija SC, Prabhakar PK, Evaluation of Lacto-Phenol Cotton Blue for Wet Mount Preparation of FecesJ Clin Microbiol 1995 33:1019-21. [Google Scholar]
[8]. Garcia LS, Diagnostic Medical Parasitology 2001 4th editionAmerican Society for Microbiology:60-105. [Google Scholar]
[9]. Thakar MR, Abraham PR, Arora S, Balakrishnan P, Bandyopadhyay B, Joshi AA, Establishment of refeeance CD4+ t cell values for adult Indian populationAIDS Research and Therapy 2011 8:35 [Google Scholar]
[10]. Srirangaraj S, Venkatesha D, Normal CD4 and CD3 counts in normal south Indian healthy adultsIndian J Med Microbiol 2010 28:183-4. [Google Scholar]
[11]. Vyas N, Pathan N, Aziz A, Enteric pathogens in HIV-positive patients with diarrhoea and their correlation with CD4+ T-lymphocyte countsTrop Parasitol 2012 2:29-34. [Google Scholar]
[12]. Vignesh R, Balakrishnan P, Shankar EM, High Proportion of Isosporiasis among HIV-Infected Patients with diarrhoea in southern IndiaAm J Trop Med Hyg 2007 77:823-4. [Google Scholar]
[13]. Mukhopadhya A, Ramakrishna BS, Kang G, Enteric pathogens in southern Indian HIV-infected patients with & without diarrhoeaIndian J Med Res 1999 109:85-9. [Google Scholar]
[14]. Kappagoda S, Singh U, Blackburn BG, Antiparasitic therapy.Mayo Clin Proc 2011 86:561-83. [Google Scholar]