The pathogenic fungi and the mycoses which have emerged in the recent years in immune-compromised hosts have emphasized the importance of medical mycology. Although fungi are ubiquitous, only a few species are pathogenic to humans. The past few years witnessed an increase in the number of true pathogenic fungi and an emergence of various opportunistic fungi which were initially considered to be non-pathogenic. Increase in fungal infections is mainly caused by increased size of the population which is at risk, which includes transplant recipients, cancer patients, those who are on immunosuppressives, those who undergo prolonged hospitalization and are on broad spectrum antibiotics and those who undergo various invasive procedures [1]. Advances in medical and surgical therapies have helped clinicians in treating previously devastating or fatal diseases, resulting in increased longevity of immunocompromised individuals who become susceptible to various opportunistic fungi which were initially considered to be non-pathogenic or of low virulence. Infections in such patients are often severe, rapidly progressing, presenting difficulty in diagnosing them as clinical manifestations often mimic other common diseases. Moreover, an increased incidence of antifungal resistance makes treatment difficult [2]. The recovery of aetiological agent from clinical specimens in culture media is considered the “gold standard”, but it is often delayed because of slow growth rates of many fungal isolates. Successful treatment of fungal infections requires high index of clinical suspicion, knowledge on various aetiological agents and their susceptibility to available antifungal agents and familiarity with measures that can be taken to reduce the chances of spread or re-infections. The choice of drug selection depends on the physician’s knowledge of a drug, drug availability, patient’s condition, concomitant medications and cost [3]. The ability to identify the causative agent of the fungal infection to the genus or species level will help in determining the treatment option for the infection and minimize treatment failure or recurrent infections [4].
Material and Methods
This study was conducted in Pad. Dr. D.Y.Patil Medical College, Hospital and Research Centre, Pimpri, Pune-18, Maharashtra, India. It comprised of samples obtained in the Department of Microbiology (Mycology section) of a tertiary care hospital over a period of two and a half years, from Jan 2010 to June 2012. A total of 704 samples were obtained from patients suspected of having fungal infections from various clinical departments of our hospital.The manner in which the specimens were collected and transported to the laboratory, depended on the type of specimens. Plucked hair samples, nail clippings, skin and scalp scrapings (obtained after cleaning the area with normal saline) were collected in clean, dry, non-glazed paper (or aluminium foil) and sent to the laboratory. Sterile body fluids (gastric aspirates, peritoneal fluid, synovial fluid, vitreous fluid, etc), tissues, pus and swabs (like throat, vaginal and conjunctival swabs, etc) and invasive catheter tips and urine were collected aseptically and transported in sterile containers, syringes or test tubes. Sputum was collected and transported in clean dry containers.Blood was collected directly in brain heart infusion (BHI) bottles or Bact/Alert culture bottles. Corneal scrapings were directly inoculated on culture media, mounted on 10% potassium hydroxide solution (KOH) on slides and transported to the laboratory [5,6].
Microbiology
For direct microscopic examination, the samples were dissolved in KOH solution (10- 40 %) and observed under microscope for fungal elements. Sputum samples were decontaminated and concentrated and other body fluids were centrifuged and the deposit was used for examination. Gram staining was done to detect presence of yeast cells and Indian ink was used to check for capsulated yeasts [5,6]. Fungal cultures were carried out by conventional methods on routine media. Any growth obtained was further identified by its temperature requirement, rate of growth, colony morphology and lactophenol cotton blue mounts. Slide culture and additional tests were performed as required. For dimorphic fungi, conversion of morphological form was done using BHI and BHIA [7,8].
Yeast identification was done on the basis of Indian ink preparation, germ tube production, sporulation on corn meal agar, urease production, sugar fermentation and assimilation and colour production on CHROM agar [7–9]. All germ tube negative Candida spp. were speciated by the automated system (Biomerieux, Vitek 2 C) using YST identification, as well as AST, determined by YST-AST-01 card.
Results
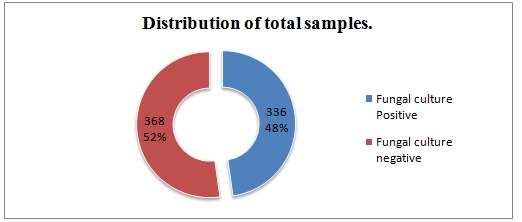
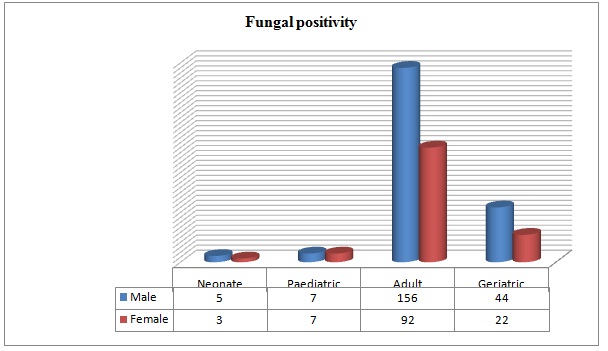
A total of 704 samples from various departments were included in the study. Among these, fungal growth was obtained in 336 samples (48%), while the rest of 368 (52 %) samples were negative [Table/Fig-1]. Maximum number of infections were observed in the adult age group [248(73.80%)], followed by the geriatric age group [66(19.64%)]. Male preponderance was observed in all age groups [Table/Fig-2].
Distribution of total samples
Age and sex distribution of fungal isolates (n=336)
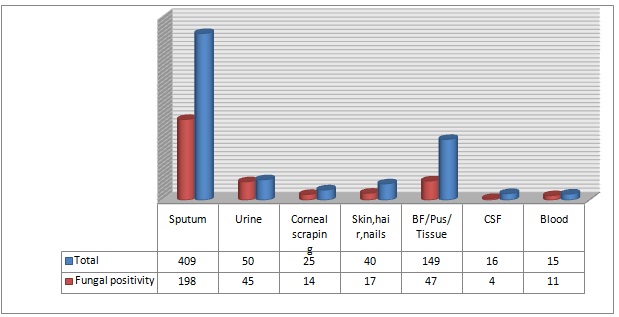
Majority of the samples received were sputum samples 409 (58.09%), followed by sterile body fluids (BFs)/pus/tissues/etc 149 (21.16%), CSF 16(2.27%), corneal scrapings 25(3.55%) and urine 50(7.10%). Skin, hairs and nails accounted for 40(5.68%) samples, while 15(2.13%) were blood samples. Most fungal species were isolated from sputum 98 (58.92%), followed by body fluids 47 (13.98%) [Table/Fig-3].
Distribution of fungal positivity from various samples
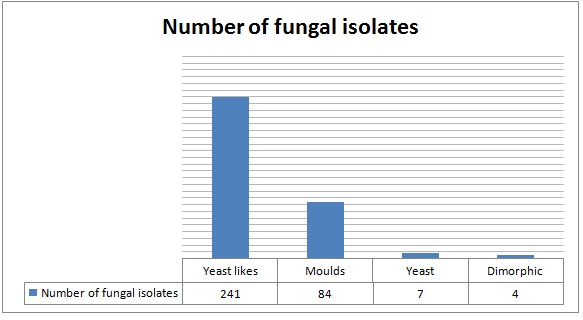
Of the 336 fungal isolates, 72.6% were yeast like organisms, followed by 24.1% moulds. Yeasts were identified in 7 cases and dimorphic fungi were identified in 4 cases [Table/Fig-4]. Among the yeasts, Cryptococcus spp. was identified in 4(1.19%) cases and Rhodotorula spp. was identified in 3 cases (0.89%). Among yeasts, Candida albicans was isolated from 173(51.4%) cases, while non albicans Candida was isolated from 68(20.23%) cases and in 3 cases, Malassezia spp. were isolated [Table/Fig-5]. Among the 81 moulds, Aspergillus spp were isolated in 47 cases, zygomycetes in 13 cases, Penicillium in 5 cases, Fusarium and dermatophytes were isolated in 4 cases each, while Fonsecaea, Madurella and Scopularis were isolated in 1 case each,. Among the dimorphic fungi, Sporothrix was isolated in 3 cases and Blastomyces spp. was isolated in 1 case.
Morphological distribution of fungal isolates
Spectrum of isolates among various samples
| Organism | Blood | CSF | BF/Pus/Tissue | Skin/Hair/Nail | Cornea | Urine | Sputum | Total |
|---|
| C. albicans | 1 | - | 21 | 1 | - | 32 | 118 | 173 |
| C.tropicalis | 2 | - | 7 | - | - | 3 | 21 | 33 |
| C. glabrata | - | - | - | - | - | 10 | 7 | 17 |
| C. parapsilosis | 4 | - | 2 | - | - | - | 8 | 14 |
| C. krusei | 3 | - | - | - | - | - | - | 3 |
| C. rugosa | 1 | - | - | - | - | - | - | 1 |
| Rhodotorula | - | - | 1 | 1 | - | - | 1 | 3 |
| Cryptococcus | - | 4 | - | - | - | - | - | 4 |
| Malassezia | - | - | - | 3 | - | - | - | 3 |
| A. fumigatus | - | - | 7 | 1 | 6 | - | 11 | 25 |
| A. flavus | - | - | 1 | 1 | 2 | - | 3 | 7 |
| A. niger | - | - | - | 2 | - | - | 10 | 12 |
| A. nidulans | - | - | 1 | - | - | - | 1 | 2 |
| A. glaucus | - | - | - | - | - | - | 1 | 1 |
| Zygomycetes | - | - | 1 | 1 | 2 | - | 9 | 13 |
| Penicillium | - | - | 1 | 2 | - | - | 2 | 5 |
| Fonsecaea | - | - | 1 | - | - | - | - | 1 |
| Fusarium | - | - | - | - | 2 | - | 2 | 4 |
| Madurella | - | - | - | - | - | - | 1 | 1 |
| Dermatophytes | - | - | 1 | 3 | - | - | - | 4 |
| Scopularis | - | - | - | - | - | - | 1 | 1 |
| Sporothrix | | - | - | 1 | 2 | - | - | 3 |
| Blastomyces | - | - | 1 | - | - | - | - | 1 |
| Unidentified | - | - | 2 | 1 | - | - | 2 | 5 |
| Total | 11 | 4 | 47 | 17 | 14 | 45 | 198 | 336 |
Discussion
Mycotic infections do not rank with bacterial, viral, helminthic and protozoal infections as causes of human suffering. However, they may still be a cause of major distress or disability in affected individuals. Their added presence may aggravate or add to the underlying disease process. Also, in the past two decades, major advances in health care management has lead to an increase in life threatening infections caused by true pathogenic or opportunistic fungi. For many years, only a few species of fungi (yeasts, moulds and dimorphic fungi) were known to cause human infections. But an increase in size of the population at risk, along with the ubiquitous presence of fungi, has lead to a great expansion in the fungal aetiology. Fungal infections are often insidious and their diagnosis are often delayed due to co-existing illnesses. The emergence of these infections has created a challenge in their diagnosis and management [10]. The risk factors or predisposing conditions of mycotic infections are well known. One group includes individuals who are susceptible due to their geographic locations. The second group is of healthcare associated. It includes individuals who are on immunosuppressive therapies, who are severely ill, who are immuno-compromised or malnourished individuals, to name a few [11]. A total of 704 samples received from various suspected cases were processed. The commonest were sputum and nasal secretions (in 409 samples). Of these, 198 were culture positive. Candida albicans was the commonest isolate (in 118 samples), while Aspergillus spp were isolated in 26 cases. 36 isolates were non-albicans Candida. A complete history, proper collection and direct microscopic correlation are essential for clinical correlation of isolates. Chronic lung conditions are usually associated with these infections. Of the culture positive sputum samples, 44 cases were diagnosed tuberculosis cases. Among them, Candida spp. were isolated in 35 cases, Aspergillus was isolated in 7 cases, and Rhizopus and Scopularis were isolated in 1 case each. Among nosocomial blood stream infections, Candidal infections have steadily increased. Candidia spp. has been reported as the fourth leading cause and most common among fungal pathogens in critical care settings. Candidaemia was associated with high crude mortality rate of above 60 %, while attributable mortality was reported to be around 49% [12,13]. Among 15 samples received for fungal aetiology studies, 11 were positive, C. parapsilosis being the most common isolate. Non- albicans Candidia are increasingly being implicated, which was reflected in the present study. Among non-albicans Candidia spp., triazoles had diminished activities against C. glabrata and C. krusei. Also, in C. parapsilosis, higher MICs were seen for Echinocandins. Hence, speciation and AST testing will help in improving patient management [14]. Of the urine samples received (50), 45 grew yeast like organisms on culture. All were Candida, among which C. albicans was seen in 32 cases and C. glabrata was seen in 10 cases. UTIs caused by fungal agents are most commonly nosocomial. Among catheter associated UTIs, fungal aetiology was most commonly seen. In community acquired UTIs, it could occur in pregnant women.
Of the 25 corneal scrapings processed, 14 were found to be positive on culture. While processing corneal scrapings, the importance of direct microscopy as a useful diagnostic tool needs to be highlighted. Among the 14 culture positive cases, direct microscopy revealed mycelial forms in 12 cases. Filamentous fungi were common. Aspergillus was the commonest [A. fumigatus (6) and A. flavus (2)]. 2 cases each revealed presence of Sporothrix, Zygomycetes and Fusarium spp. [15–17]. Cryptococcal meningitis was commonly associated with immunocompromised patients [18]. In our study also, among CSF samples, Cryptococcus neoformans was isolated in 4 cases, all of whom were immunocompromised. Of the 4 Cryptococcus neoformans isolates, two were positive by India ink preparations on direct microscopy.
Body fluids, pus and tissue samples reflected soft tissue infections. They included some cases which were unusual to the region: a case of white grain mycetoma caused by A. nidulans and a case of chromoblastomycosis of face caused by Fonsecaea pedrosii [19,20]. Dimorphic fungi, Blastomyces, was isolated from vitreous fluid in a case of endophthalmitis with history of road traffic accident. He was advised intravitreal Amphotericin B injection.
Conclusion
The role of diagnostic mycology laboratory is important in the management of fungal infections. An understanding of fungal infections in each set-up will help greatly in improving diagnostic and therapeutic approaches. Non-albicans Candida infections are also increasing globally making speciation necessary. Culture and identification of mycotic infections to the genus and species level, is essential, for commencement of suitable antifungal therapy. The clinician-microbiologist collaboration will help in improving patient care.