Background: Sweepers are chronically exposed to dust raised during sweeping. Dust is regarded as the most influential agent and it is perceived as a frequent cause of respiratory system illness and may cause acute and chronic lung function impairment.
Aims: The aim of this study was to determine the acute lung function changes in sweepers exposed to dust generated from street sweeping.
Material and Methods: This study was conducted in central Karnataka, India, on 25 female sweepers and 25 healthy female control subjects who were comparable in age, height and weight. The pulmonary function test was performed in controls, sweepers before and after sweeping, by using RMS medspiror and results were compared by Student’s unpaired ‘t’ test.
Results: The results showed a significant reduction in percent predicted values and mean values of FVC, FEV1, PEFR, FEF25-75% and FEF 200-1200 between sweepers and their matched controls. Pulmonary function after sweeping also showed a significant decrease.
Conclusions: On comparing the pulmonary functions of sweepers before and after sweeping, it was concluded that inhalation of dust acutely affected the lung function of sweepers in India and that sweepers were at a risk of developing occupation related lung function impairment. We recommend that the workers should use protective face masks and do wet sweeping instead of dry sweeping during sweeping activity.
Forced vital capacity, Pulmonary function test, Street sweepers
Introduction
The prevalence of occupational health hazards and mortality has been reported to be unusually high among various workers in India. Occupational lung disease tops the list of major occupational illnesses. Developed countries take more precautions with respect to health of occupations, but in developing countries like India, where majority of workers work without proper protection, this aspect is quite neglected [1]. There is a widespread misconception that occupational health is mainly concerned with industries and industrialized countries. But in a country like India, millions of people are engaged in labour like street sweeping, stone grinding, paddy thrashing, weaving, etc. [2].
In India, street sweeping is considered as a job of the underprivileged class. Most of the street sweepers are below poverty line, without much education, dwelling in poor housing environments and without proper medical attention [3].
In developing countries, dust in the streets plays an important role in environmental pollution [4]. Dust is raised during sweeping with brooms and by vehicular movement, as well as through other human activities. Street sweepers are at a risk of exposure to complex mixtures of pollutants such as soil, dust, bioaerosols of biological origin like pollens, organic materials from plants, dust which results from vehicular movements and emission, which make them susceptible to occupational lung disease. Sweepers are prone to be affected by health hazards during their occupational activities [5]. Lungs, by virtue of their direct contact with the atmospheric air, are naturally first to bear the onslaught of air contaminants [6].
The inhalation of ambient particles and their deposition in the lung, can interact with lung cells and may have adverse effects. These interactions eventually lead to the release of various cytokines, causing inflammatory reaction and tissue injury [7].
Lung diseases which result from occupational exposure are most likely caused by the inhalation of dust and deposition of inhaled particles in lungs. The site of deposition is determined by a number of factors like the size, chemical and physical characteristics of the aerosol and the duration and frequency of exposure, along with the host response to the inhaled particles [8]. Reduction in lung functions has been reported in cotton workers, coal miners, grain and flour mill workers, quarry workers and workers who are exposed to tobacco dust, barley dust and talc dust [8].
In spite of the several reports on the acute effects of exposure to dust on lung functions, no study has been undertaken on the effect of acute exposure to dust which is raised by street sweeping, on the lung functions of the street sweepers in India. Hence, this study was undertaken to determine the acute lung function status of sweepers exposed to dust generated from street sweeping.
Material and Methods
The present study was conducted on 25 female sweepers in the age group of 20–50 years, engaged in street sweeping and 25 healthy female controls comparable in age, height and weight. These workers work for 4-5 hours per day and six days per week without using any self-protective measures. All the subjects gave informed consents. Detailed systemic examination was done to rule out the presence of any systemic illness. Subjects suffering from any diseases which affected the pulmonary functions, such as acute or chronic respiratory illnesses, established bronchial asthma, pulmonary tuberculosis, diabetes mellitus, hypertension, neuromuscular diseases, arthritis of spine and other systemic illnesses were excluded from the study.
Lung function test was performed using computerized RMS medspiror. This instrument has facility for calibration and gives reliable values of test, which are displayed in the computer screen with its graphical representation. It is equipped with a software which can predict the values of test on the basis of sex, age, height and weight. The test protocol, maneouver of test was explained to the subjects. Short time was given to the subjects to get accustomed to the instrument and the procedure was performed before the actual test. The tests were conducted while subjects were sitting comfortably on stools. Each test was repeated three times, with an interval of five minutes between the tests and the best of three readings was taken. All pulmonary function tests were carried out before and after sweeping. The lung function parameters were Forced Vital Capacity (FVC), Forced Expiratory Volume in first second of forced expiration (FEV1), Forced Expiratory Ratio (FEV1/FVC %), Peak Expiratory Flow Rate (PEFR), Forced Expiratory Flow during 25-75% of expiration (FEF 25-75%), Forced Expiratory Flow during 200-1200 ml of expiration (FEF200-1200) [9].
Statistical Analysis
The results were presented as Mean ± SD and percentage difference. Unpaired’ test was used for group wise comparisons. p-value of 0.05 or less was considered for statistical significance.
Results
[Table/Fig-1] shows the comparison of mean values of anthropometric parameters in controls and sweepers. There were no significant differences in the anthropometric parameters in terms of age, height and weight between the groups.
Anthropometric parameters of sweepers compared with their matched controls
| Parameters | Controls (n =25) | Sweepers (n =25) | Percentage difference (%) | Significance |
|---|
| Mean ± SD | Mean ± SD | *t-value | p-value |
|---|
| Age (years) | 39.64 ± 12.44 | 39.40 ±7.42 | 0.61 | 0.93 | NS |
| Height (m) | 1.55 ± 0.05 | 1.50 ± 0.06 | 3.33 | 0.001 | NS |
| Weight (Kg) | 54.20 ± 6.04 | 53.12 ± 10 | 2.03 | 0.65 | NS |
| BMI | 22. 52± 2.70 | 23.67 ± 4.02 | -4.86 | 0.24 | NS |
*unpaired’ test
p > 0.05, Not significant (NS) p < 0.01Significant (S),
p < 0.001, Highly Significant (HS)
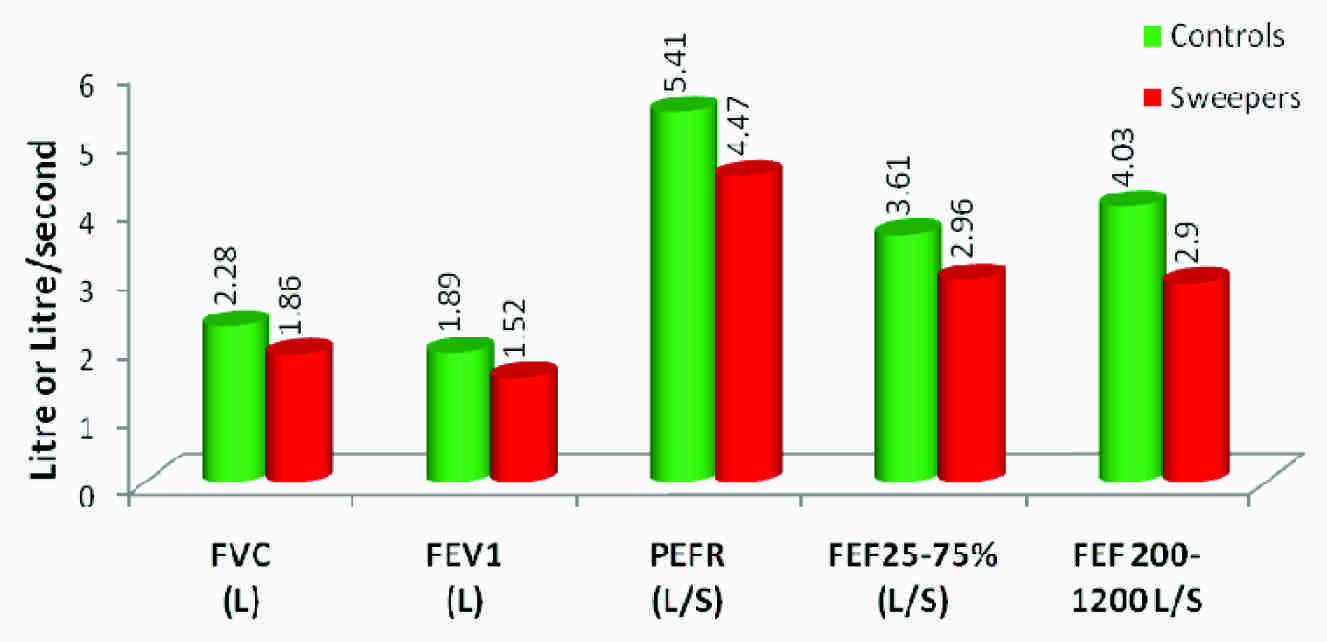
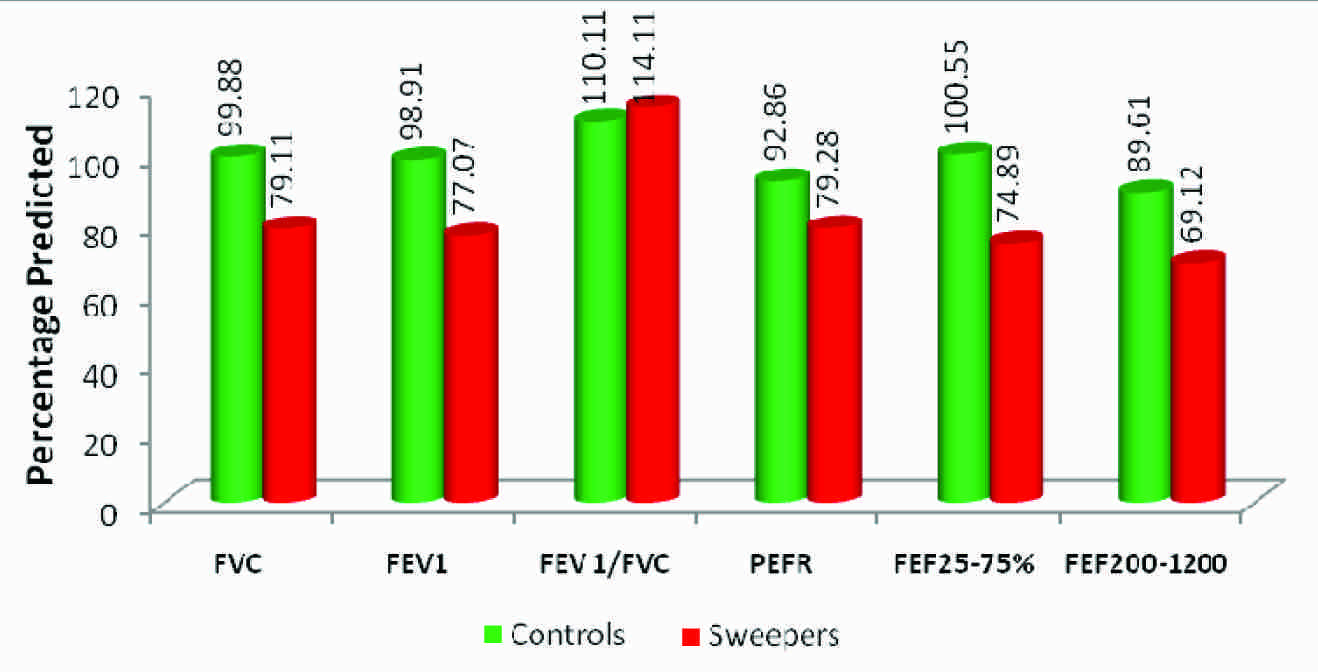
[Table/Fig-2, 3] depict the comparison of lung function parameters in sweepers and their matched control groups. All pulmonary function parameters were compared in terms of both mean values and percent predicted values adjusted for race, gender, height and age. Sweepers showed a significant reduction in mean values and percentage predicted values of FVC, FEV1, PEFR, FEF 25-75% and FEF 200-1200, as compared to their matched controls, but these workers showed a statistically significant increase in FEV1/ FVC% relative to controls. The mean duration of exposure to dust in sweepers was 7.5 ±4.1years (Range 2-16 years).
Comparison of mean values of lung function parameters between the sweepers and the controls
Comparison of percentage predicted values of lung function parameters between the sweepers and the controls
[Table/Fig-4, 5] summarize the acute lung function response to inhaled dust. Pulmonary functions before and after sweeping were compared. They showed a significant reduction in mean values and percentage predicted values of FVC, FEV1, PEFR, FEF25-75% and FEF 200-1200 after sweeping and increase in FEV1/ FVC% were compared with the values before sweeping.
Mean values of lung function parameters in sweepers before and after sweeping
| Parameters | Before sweeping (n =25) | After Sweeping (n =25) | Percentage difference (%) | Significance |
|---|
| Actual value |
|---|
| Mean ± SD | Mean ± SD | *t-value | p-value |
|---|
| FVC (L) | 1.86 ± 0.33 | 1.45 ± 0.35 | 28.28 | 7.69 | < 0.001, HS |
| FEV1 (L) | 1.52 ± 0.31 | 1.30 ± 0.38 | 16.92 | 3.82 | < 0.001, HS |
| FEV1/FVC (%) | 83.53 ± 16.59 | 92.07 ± 13.82 | -7.10 | 5.38 | < 0.001, HS |
| PEFR (L/s) | 4.47 ± 0.79 | 3.37 ± 1.02 | 32.64 | 9.80 | < 0.001, HS |
| FEF25-75% (L/s) | 2.96 ± 0.69 | 2.20 ± 0.55 | 34.55 | 8.04 | < 0.001, HS |
| FEF200-1200 (L/s) | 2.90 ± 0.97 | 2.34 ± 0.86 | 23.93 | 3.52 | < 0.001, HS |
*unpaired’ test
p < 0.05, Not significant (NS), p < 0.01Significant (S),
p < 0.001, Highly Significant (HS)
Percentage Predicted values of Lung function parameters in sweepers before and after sweeping
| Parameters | Before sweeping (n =25) | After Sweeping (n =25) | Percentage difference (%) | Significance |
|---|
| Percentage predicted |
|---|
| Mean ± SD | Mean ± SD | *t-value | p-value |
|---|
| FVC | 79.11 ±18.12 | 65.56 ± 16.09 | 20.67 | 7.38 | < 0.001, HS |
| FEV1 | 77.07 ±13.04 | 72.58 ± 12.50 | 6.19 | 2.17 | 0.03, S |
| FEV1/FVC (%) | 114.11±24.55 | 125.81±21.82 | -9.30 | 8.12 | < 0.001, HS |
| PEFR | 79.28±10.48 | 60.29 ±17.46 | 31.50 | 1.99 | 0.05 S |
| FEF25-75% | 74.89±12.71 | 66.55±11.06 | 12.53 | 5.14 | < 0.001, HS |
| FEF200-1200 | 69.12±16.11 | 59.12 ± 13.77 | 16.91 | 2.25 | 0.02 S |
*unpaired ‘t’ test
p > 0.05, Not significant (NS), p < 0.01Significant (S),
p < 0.001, Highly Significant (HS)
Discussion
In recent years, there has been increasing awareness in the developing countries on occupational health hazards, where most of the workers work without proper precautions. To the best of our knowledge, ours was the first study that had been carried out in India on the acute effect of dust on lung functions of street sweepers. In our study, in the central Karnataka region, no statistical significant difference was found in the major confounding factors like age, height and weight, that affected the lung function parameters between sweepers and their matched controls. Our study showed a statistically significant decrease in the mean values and percentage predicted values of FVC, FEV1, PEFR , FEF25-75% and FEF200-1200 in sweepers, as compared to the controls. But FEV1 /FVC ratio was increased and it was also significant. The parameters, FVC, FEV1 and FEV1/ FVC provide the best method of detecting the presence and severity of airway obstruction or restriction, as well as the overall respiratory impairment. In our study, FVC and FEV1 were decreased, but the FEV1 /FVC ratio was increased and it was more towards restrictive pulmonary impairment. PEFR values which are especially valuable in the diagnosis of obstruction were also reduced in our study. FEF25-75%, the more sensitive indicator of small airway obstruction was also found to be reduced. All the above findings suggested both restrictive and obstructive lung function impairments in sweepers, which may be attributed to inhalation of mixture of dust which affects the airways in different ways.
A study on Nigerian female sweepers reported an apparent reduction in all the mean lung function values, even though it is not statistically significant [4]. Similarly, a study on sweepers in inner and outer regions of Bangkok metropolis showed that the mean FVC, FEV1 and FEF25-75% of the street sweepers were significantly lower than the mean predicted values [10].
Our findings were similar to those of a population based study in Spain, which showed that pulmonary function parameters were lower in subjects highly exposed to dust, such as cleaners and road sweepers, with a decrease in FEV1 and FEF 25–75 % , but in contrast to our findings, they found a decrease in FEV1/FVC ratio. It was also reported that symptoms of chronic bronchitis and cough were more frequent in them [11]. Similarly, two other studies which were conducted on sweepers revealed that chronic respiratory diseases like chronic bronchitis, asthma and bronchiectasis were significantly high among street sweepers (5.9%) than among subjects of the comparison group [2,3].
Study which was conducted on sweepers who were working in dump sites showed significantly low pulmonary functions in sweepers as compared to those in loaders and drivers. Female workers had significantly lower pulmonary function values as compared to male workers. The pulmonary functions were significantly lower than their predicted values in workers than in residents who were living near the dump site [12]. The finding of our study, that chronic changes in the lung function observed in sweepers were caused by continuous exposure to the dust, were in line with the findings of the others.
The acute lung function changes were also studied by us, by comparing pulmonary function before and after sweeping. It showed a significant reduction in mean values and percentage predicted values of FVC, FEV1, PEFR, FEF 25-75% and FEF 200-1200 and significant increase in FEV1 /FVC ratio after sweeping, as compared to the values before sweeping.
Study on acute lung function changes and work-related symptoms in workers in the animal feed industry showed that all lung function variables showed a decrease after the work shift. Maximum Mid-Expiratory Flow (MMEF), Maximum Expiratory Flow rate at 50% of vital capacity (MEF50) and for Forced Expiratory Volume in 1 second (FEV1) were affected more as compared to other parameters [13]. The pulmonary function tests carried out before starting the shift and after 7 hours of exposure to cotton dust in textile industry showed a decrease FVC and FEV1 [14].
A study on acute respiratory effect of the occupational exposure to dust in cement workers, conducted in Tanzania, found a relationship between the exposure and acute response of lung to the dust and they also observed a significant decrease in the post shift PEF values. It also showed that high exposure groups had more significant respiratory symptoms like sneezing, stuffy nose, running nose and shortness of breath [15]. Acute cross-shift respiratory changes were evaluated in workers of wheat harvest in northeastern Colorado. Ten percent of the workers had moderate airway obstruction, as was indicated by the pre-shift spirometry test results. Sixty percent of workers experienced a cross-shift change in at least one respiratory symptom. Peak expiratory flow rate was found to decrease over the work shift in a manner which was similar to that which was experienced by cotton workers [16]. Acute airflow obstruction after an intense 5-month exposure to chrysotile asbestos has also been documented [17].
A significant correlation was found between the respirable fraction of peat dust and decrease in FVC and FEV after a work shift. Although the effects on lung function were less, the finding indicated that dust could act as a bronchoconstrictor, even in healthy subjects [18]. A study on acute effects of herbal tea dust extracts on lung function indicated mean decreases in all lung function parameters like FVC, FEV1, FEF25 and FEF50 following inhalation of various tea dust [19]. A study on acute lung function response to cotton dust in atopic and non-atopic individuals showed a significant decrease in FEV1 values after exposure to cotton dust, independent of atopic status. Significant exposure related decreases occurred in all spirometric indices like FVC, FEF25 and FEF50, independent of atopic status [20]. Yet another study showed that bronchial hyper responsiveness tended to be higher in cleaners who suffered from tight or wheezy chest at work. Chronic bronchitis and high chronic airflow limitation occurred more frequently in them. Lung functions in cleaners with asthma tended to be lower than in office workers with asthma, which was statistically significant for the PEF [21].
The results of the present study on street sweepers were similar to the findings of other researches on sweepers and others who were exposed to dust at work and they suggested that dust generated during sweeping adversely affected the pulmonary functions in the long term. Our results also suggest that exposure to dust causes acute decrease in the lung function, that it is a risk factor for post shift changes in the lung function and that it is associated with chronic changes in lung. The major advantage of evaluating the post shift changes in lung function parameters of sweepers, is that we can identify the individuals who are susceptible. Medical surveillance of early detection can contribute to reducing the burden of lung function impairment.
Conclusion
In conclusion, it may be said that exposure to dust in sweepers has an immediate irritating effect on the respiratory tract, leading to some degree of lung function impairment. Protection of the workers with appropriate respiratory protective masks and educating them suitably are recommended. Effective dust-control measures such as wetting the surface before sweeping, definitely reduce acute respiratory health hazards. Periodic assessment of pulmonary function by spirometry has to be done.
*unpaired’ test
p > 0.05, Not significant (NS) p < 0.01Significant (S),
p < 0.001, Highly Significant (HS)
*unpaired’ test
p < 0.05, Not significant (NS), p < 0.01Significant (S),
p < 0.001, Highly Significant (HS)
*unpaired ‘t’ test
p > 0.05, Not significant (NS), p < 0.01Significant (S),
p < 0.001, Highly Significant (HS)
[1]. Park K, Occupational healthIn: Park’s textbook of preventive and social medicine 2007 18th edJabalpurM/s Banarsidas Bhanot:608-10. [Google Scholar]
[2]. Yogesh D S, Sanjay PZ, A study of morbidity pattern in street sweepers: A Cross-sectional studyIndian J Community Med 2008 33(4):224-28. [Google Scholar]
[3]. Yogesh SD, Zodpey SP, Respiratory morbidity among street sweepers working at Hanumannagar Zone of Nagpur Municipal Corporation, MaharashtraIndian J Public Health 2008 52(3):147-49. [Google Scholar]
[4]. Nku CO, Peters EJ, Eshiet AI, Oku O, Osim EE, Lung function, oxygen saturation and symptoms among street sweepers in Calabar-NigeriaNigerian Journal of Physiological Sciences 2005 20(1-2):79-84. [Google Scholar]
[5]. Marziale MH, De Carvalho EC, The occupational risks in urban cleaning: street sweepingRev Gaucha Enferm 1989 10(1):71-81. [Google Scholar]
[6]. Morgan Seaton, SilicosisOccupational lung diseases 1995 3rd edPhiladelphiaWB Saunders Company:222-37. [Google Scholar]
[7]. Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL, Environmental lung diseasesIn: Harrison’s principles of Internal Medicine 2008 Vol.216th edNew YorkThe McGraw Hill Companies:1521-27. [Google Scholar]
[8]. Garshick E, Schenker MB, Dosman JA, Occupationally induced airway obstructionMed Clin North Am 1996 80(4):851-78. [Google Scholar]
[9]. Wagner NL, Beckett WS, Steinberg Using spirometry results in occupational medicine and research. Common errors and good practice in statistical analysis and reportingIndian Journal of Occupational and Environmental medicine 2006 10(1):5-10. [Google Scholar]
[10]. Wasuthep Boonchoo. A comparative study of lung function of street sweepers in inner and outer regions of Bangkok metropolis.Dissertation.Thailand: Mahidol University, 2005 [Google Scholar]
[11]. Sunyer Jordi, Kogevinas Manolis, Kromhout Hans, Antó Josep M, Roca Josep, Tobias Aurelio, Pulmonary ventilatory defects and occupational exposures in a population-based study in SpainAm J Respir Crit Care Med 1998 157:512-17. [Google Scholar]
[12]. Ramaswamy P, Balakrishnan Srinivasan K, Sambandam R, Paulsamy S, Thanasekaraan J V, Health hazards and pulmonary functions in solid waste management sector of ChennaiEpidemiology 2007 18(5):95-96. [Google Scholar]
[13]. Tjabe Smid, Heederik Dick, Houba Remko, Quanjer HP, Dust- and endotoxin-related acute lung function changes and work-related symptoms in workers in the animal feed industryAmerican Journal of Industrial Medicine 1994 25(6):877-88. [Google Scholar]
[14]. Parikh JR, Majumdar P K, Shah A R, Mohan Rao N, Kashyap S K, Acute and chronic changes in pulmonary functions among Indian textile workersOccup Med (Lond) 1990 40(2):71-4. [Google Scholar]
[15]. Mwaiselage J, Moen B, Bratveit M, Acute respiratory health effects among cement factory workersInt Arch Occup Environ Health 2006 79:49-56. [Google Scholar]
[16]. Viet SM, Buchan R, Stallones Acute respiratory effects and endotoxin exposure during wheat harvest in Northeastern ColoradoApplied Occupational and Environmental Hygiene 2001 16(6):685-97. [Google Scholar]
[17]. Harless KW, Watanabe S, Renzetti AD, The acute effects of chrysotile exposure on lung functionEnvironmental Research 1978 16(1-3):360-72. [Google Scholar]
[18]. Sandstrom T, Hedman BK, Ledin M, Bjermer L, Bylund SH, Stjernberg N, Exposure to peat dust: acute effects on lung function and content of bronchoalveolar lavage fluidBritish Journal of Industrial Medicine 1991 48:771-75. [Google Scholar]
[19]. Zuskin E, Kanceljak B, Witek TJ, Schachter E N, Acute effects of herbal tea dust extracts on lung functionChest 1989 96:1327-31. [Google Scholar]
[20]. Sepulveda M, Castellan RM, Hankinson JL, Cocke JB, Acute lung function response to cotton dust in atopic and non-atopic individualsBritish Journal of Industrial Medicine 1984 41:487-91. [Google Scholar]
[21]. Zock JP, Kogevinas M, Sunyer J, Jarvis D, Torén K, Anto JM, Asthma characteristics in cleaning workers, workers in other risk jobs and office workersEur Respir J 2002 20:679-85. [Google Scholar]