Diverticulum of the gall bladder is an important but distinct anatomical entity with significant clinical implications. Congenital diverticulum of the gall bladder is one of the rarest of all anomalies, corroborated by its very low incidence and infrequent reports and references in the literature [1]. Diverticulum can be of congenital or acquired variety. The congenital type contains all three layers of gall bladder wall [2], whereas the acquired variety is a result of the disease process and has little or no smooth muscle in its wall [3]. Diverticulum of the gall bladder may remain silent or present with an array of signs and symptoms. It is often associated with cholelithiasis [4] and carcinoma has been reported in congenital diverticulum of gall bladder [5]. In this following article, diverticula of the gall bladder, found in course of study of 100 gall bladders, has been described.
Material and Methods
This morphological study was carried out on one hundred specimens of human gall bladders collected from 10% formalin fixed human cadavers during routine undergraduate dissection in the Department of Anatomy, Jawaharlal Nehru Medical College, Sawangi (Meghe), Wardha, and Department of Anatomy, Subharti Medical College, Meerut during a four-year period i.e., 2008-2012. The age of the cadavers was between 40-75 years. Out of the hundred, 90 were male cadavers and 10 were female. Necessary permission from the Institutional Ethical Committee was obtained for the study. Histology of the diverticulum using Haematoxylin and Eosin staining was also done. Slides were studied under low (10x) medium (40x) and high (100x) magnification. Cadavers with abdominal surgery and crush injury to the abdominal organs were excluded from the study.
Results
Diverticulum of gall bladder was found in a total of nine (9%) cadavers out of one hundred. All of these were found in male cadavers. These diverticulum were studied with respect to their number, position, dimensions, shape, changes in the lining mucosa of the diverticulum and that of the luminal surface of the whole gallbladder and histology. Presence of any other congenital anomaly of gall bladder and extrahepatic biliary apparatus was also looked into. The specimens with diverticulum were labelled as D1, D2, D3, D4, D5, D6, D7, D8 and D9 respectively and are individually summarised in [Table/Fig-1].
Description of the Diverticula of Gall Bladder with reference to their Number, Position, Appearance and Dimensions
| Specimen no. | Number | Site | Shape | Length (cms) | Maximum transverse diameter (cms) | Diameter of luminal orifice (cms) |
|---|
| D1 [Table/Fig-2] | Solitary | Neck | U shaped | 2.4 | 1.8 | 1.2 |
| D2 | Solitary | Neck | Conical | 1 | 0.6 | 0.4 |
| D3 [Table/Fig-3] | Solitary | Body | Thumb-shaped | 5.2 | 2.8 | 1.5 |
| D4 | Solitary | Body | Pyriform | 2.4 | 1.2 | 0.4 |
| D5 | Solitary | Body | Cylindrical | 2 | 1.2 | 0.4 |
| D6 [Table/Fig-4] | Solitary | Fundus | Conical | 1.7 | 0.8 | 0.4 |
| D7 | Solitary | Fundus | Conical | 2.5 | 1.2 | 0.6 |
| D8 | Solitary | Fundus | Conical | 1.5 | 0.8 | 0.7 |
| D9 | Solitary | Tip of the Fundus | Comma shaped | 2.6 | 1.2. | 0.7 |
I. Number: All of these nine diverticula were solitary ones.
II. Position: Out of the nine diverticula, two (2%) diverticula, i.e. D1 [Table/Fig-2] was at the medial side of the neck, and D2 also at the neck was found more superiorly. D3 [Table/Fig-3], D4 were at the lower half of the body, located on its inferior serosal surface and D5 was found at a lateral aspect near the lateral margin of the gall bladder fossa again at the lower part of the body . Four (4%), i.e., D6 [Table/Fig-4], D7, D8,and D9 were found at the fundus of the gall bladder. D6 [Table/Fig-4] D7, and D9 were found at the tip of the fundus , whereas D8 was medial to the tip of fundus.
shows a solitary U-shaped diverticum at the neck of the gallbladder

shows a solitary, thumb-shaped diverticulum at the lower half of the body of gallbladder

shows a solitary cone-shaped diverticulum at the fundus of the gallbladder

III. Dimensions of the diverticulum: The length of the diverticula, and hence the depth of the pouches formed, were between 0.9-5.2 cm. The maximum external diameters varied from 0.6 cm to 2.8 cm.
IV. Shapes of the diverticula: The diverticula were conical in four (4%), i.e., D2, D6 [Table/Fig-4], D7, D8 specimens. In the other five they were either pyriform (1%), cylindrical (1%), thumb-shaped (1 %) [Table/Fig-3] comma-shaped (1%) or U-shaped (1%,[Table/Fig-2]. They are summarised in [Table/Fig-1].
V. Luminal surface of the diverticulum: Internally, all five diverticula appeared as isolated solitary pouches connected to the main gall bladder chamber through a narrow orifice [Table/Fig-5], the luminal diameter of which ranged from 0.4 cm to 1.5 cm. Naked eye appearance of the whole gall bladder mucosa in general and that of the diverticula in particular as seen in all specimens were normal, showing the normal honeycomb appearance. There were no breaches of the gall bladder mucosa anywhere in any of the specimens. Thickening of gall bladder wall was also not evident in any of them. Stones/calculi were not found in the pouches formed by the diverticula or anywhere in the gall bladders.
shows luminal orifice of the pouch formed by the diverticulum

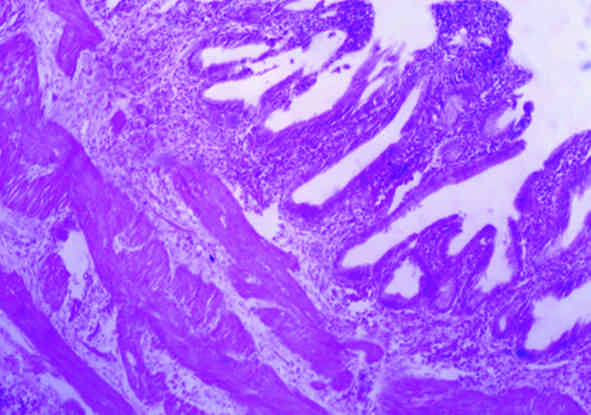
VI. Histology of the diverticulum: Histology of all the specimens was consistent with that of the normal undiseased gall bladder as seen in [Table/Fig-6]. The mucosa was thrown into folds. It was lined by a single layer of tall columnar pale staining cells with basal nuclei; numerous short irregular microvilli lined the apical surface of the cells. The underlying lamina propria contained loose connective tissue with blood vessels, few lymphocytes and occasional mucus glands, arterioles and venules. The muscularis showed randomly arranged layers of smooth muscle fibers. Externally they were covered by a serosa in all the specimens, thereby confirming the diagnosis of congenital (true) diverticula.
Histology of the gallbladder diverticulum (D6) under medium magnification (40x). It shows mucosa consisting of the tall columnar with basal nuclei cells and the muscularis with the intact muscle layer .Serosa or adventitia is not visible in the slide
All the above findings confirm the diagnosis of congenital, i.e., congenital (true) solitary fundic diverticula.
Discussion
A gallbladder diverticulum is a rare and an uncommon entity rarely discussed in the literature [2], usually in the form of case reports. It has been reported to be one of the rarest congenital anomalies of the gall bladder [1]. As already stressed, these can be either of congenital or acquired variety. Congenital gall bladder diverticulum should be differentiated from acquired or pseudo or false variety which is a result of underlying pathology. In this context, it will be pertinent to discuss briefly the anatomy and embryogenesis of extra hepatic biliary apparatus including the gall bladder.
The extra hepatic biliary apparatus comprises of the extra hepatic bile ducts and the gall bladder. The most unique feature of the so called normal anatomy of the extra-hepatic biliary system is its high degree of variability, wherein classical textbook anatomy of the biliary tract is seen in less than 50 % of cases [6].
The human gallbladder is a pyriform sac that lies in the gall bladder fossa, on the inferior surface of the right lobe of the liver. It is described as having a body neck and fundus. It is between 7 and 10 cm long in adults [7]. The liver, gall bladder and the biliary ductal system develop from the hepatic diverticulum of the foregut, in the beginning of the fourth week of development. This diverticulum rapidly proliferates into the septum transversum dividing into two parts – the cranial part being primodium for the liver and the bile ducts, while the caudal part gives rise to the gall bladder and the cystic duct. Initially the extra hepatic biliary apparatus is patent in the early uterine life but becomes solid later on by epithelial proliferation. Eventually it gets recannalised subsequent to degeneration of these cells [8]. Studies by Roskams and Desmet [9] reveal this structure to be patent from the beginning and it remains in continuity with the developing liver at all stages. Kuffer cells, haemopoietic cells and connective tissue cells are derived from the mesoderm of septum transversum [8]. Bile begins to flow at about the 12th week of intra-uterine life. The in-growing capillary plexus from the vitelline and umbilical veins form the sinusoids [8]. Any arrest or deviation from the normal developmental process in the intra-uterine life results in some sort of anomaly of the gallbladder and the biliary system. This holds true for congenital diverticulum as well, the genesis of which has been discussed subsequently. Anomalies of biliary apparatus and liver may be associated with congenital lesions elsewhere, including cardiac lesions, polydactyly and polycystic kidneys. They have been related to maternal virus infection, such as rubella [8].
The incidence of congenital diverticula of gall bladder has been reported from 0.0008% of all resected gallbladders at the Mayo Clinic to 0.06% of a series of congenital anomalies of the gallbladder collected from the world literature [5]. Blalock [10] found diverticula in 0.2% of 727 surgically removed gall bladders. Gross [11] reviewed 148 cases of anomalies of the gallbladder, and found nine cases of congenital diverticula. Eelkema [12] in his case report of “Partial Duplication of Gall Bladder – Diverticulum type” cited Castro who reviewed 68 of 74 cases in the Mayo Clinic files up to 1944 that were suggestive of diverticulum of the gallbladder, and accepted only 3 cases as congenital diverticulum. Golob [13] reviewed 29701 surgically-removed gall bladders and found only 25 cases (0.08%) with diverticulum. In the present study we found diverticulum in nine (9%) out of a 100 cases. The incidence and findings of various workers is briefed in [Table/Fig-7].
Description of the Diverticula of Gallbladder with reference to their Number, Position, Appearance and Dimensions
| Sr. | Researchers | Type of diverticulum | Type of study | Remarks |
|---|
| 1. | Bogatko & Mehman [4] | Congenital | Surgical Case report | Cholelithiasis Cholecystitis |
| 2. | Chin & Chapman [5] | True | Case report Sonography | Malignancy |
| 3. | Parikh et al., [15] | Not mentioned | Case report Explorative laprotomy | Giant diverticulum |
| 4. | Sirakov et al., [17] | True diverticula 1.4%, n=22 Pseudo diverticula 8.2%,n= 22 | Surgical study | Cholelithiasis Cholecystitis |
| 5. | Garg and Dass [10] | Not mentioned | Surgical Case report | Multiple diverticula |
| 6. | Kramer et al., [18] | Not mentioned | Surgical Case report | Prolonged non -specific ailment |
| 7. | Basaranoglu & Balci [19] | True | Case report MRCP * | - |
| 8. | Lee et al., [5] | Pseudo diverticula | Case report Sonography + surgery | Acalculous Cholecystitis |
| 9. | Doganay et al., [2] | True | Case report Sonography +MRCP* | Recurrent Cholangitis |
| 10. | Peronne & Hernandez [20] | True | Case report Sonography | - |
| 11. | Present study (2008-2012) | True 9% n= 100 | Cadaveric study | - |
These diverticula can occur anywhere along the surface of the gall bladder from the fundus to the neck [14]. Parikh et al., [15] have reported cholecystitis and cholelithiasis in a fundic diverticulum. In the present study, a diverticulum was found at the fundus in four (4%) specimens. Fundic diverticula are thought to be a consequence of incomplete vacuolisation of the solid gallbladder during embryonic life, wherein an incomplete septum pinches off a small cavity at the tip of the gallbladder [8]. Two (2%) diverticula were found at the neck and two (0.02%) on lower part of the body of gall bladder. Diverticulum of the body and neck results from persistent cystohepatic ducts which run during embryonic life between the gallbladder and liver [8]. Arcomano and Barnett [1] believed that it was unlikely that congenital diverticulum had its origin from a single error of germ-plasm differentiation, as there were several representative types, the development of which were in sync with the previously established theories. The size of the diverticula varies greatly, ranging from about 0.6 cm in diameter [10,16] to giant ones almost the size of a man’s fist [16]. The largest congenital diverticulum reported is about 14 cm x 8 cm in a 51-year-old male patient of chronic cholecystitis and cholelithiasis [17] with complaints of pain in abdomen and epigastric mass of 6 months duration. In the present study, the largest diverticulum was 5.2cm x 2.8cm and smallest one was 1 cm x 0.6 cm.
Multiple small diverticula present all over the gall bladder have been reported by Garg and Dass [10] in a 32-year-old female patient, presenting with abdominal pain and jaundice of two weeks duration, with a stone in the common bile duct. The diverticula in our study were all solitary ones. In the present study all the diverticula were without any calculi or any perforation thereof. Their shapes as found in the present study were either conical, pyriform, cylindrical, comma-shaped, thumb-shaped and U-shaped. The luminal orifice was small and all the diverticula had a narrow neck consistent with the characteristics of congenital diverticulum of gall bladder. Histology of all the specimens was consistent with that of congenital or true diverticulum showing all the three layers of gall bladder wall.
Congenital diverticulum have been reported by Chin and Chapman [5], Sirakov et al., [17], Kramer et al., [18], Basaranoglu and Balci [19], Doganay et al. [2] and Perrone and Hernandez [20] in recent literature. Their relative incidences type and clinical correlation as found by various researchers are depicted in [Table/Fig-7].
Congenital diverticula (true) includes all three layers of the gallbladder wall and should be distinguished from pseudo diverticula developing in a diseased gall bladder as a result of partial perforation [8]. Pseudodiverticula have an acquired cause, multiple fundal lesions, internal saccular lesions without external hernia like protrusions and little or no smooth muscle in gall bladder wall [3]. They contain multiple stones and are more prevalent [21]. Roentgenographically, congenital diverticula visualized and contract normally following a motor fatty meal in absence of secondary inflammatory pathology, whereas the acquired diverticula visualized but does not contract normally because of inhibition by mechanical traction factors or because there is no muscularis mucosae present within the pseudodiverticula to respond to normal stimulus [1]. The diverticula found in the present study were congenital, i.e., true diverticula, as all of them were solitary, external out pouching of the gall bladder wall, without calculi and without any breach of mucosa. No internal saccular lesions were observed in the interior of the gall bladder as found in pseudo diverticula. Histological study also confirmed the diagnosis of congenital diverticulum.
Rokitansky-Aschoff sinuses should be differentiated from diverticulum. They consist of hernia like protrusions of gall bladder mucosa through the muscular layer (intramural diverticulosis). These though potentially congenital are particularly prominent with chronic cholecystitis, especially with the rise of intraluminal pressure in the viscus [8]. They can also occur because of the lack of a muscularis mucosa and the loose arrangement of the muscular bundles. They may extend to the muscular layer of the gall-bladder wall, penetrate into the intramuscular lacunae, or may progress through the muscular wall into the underlying connective tissue, even reaching the serosa occasionally [22]. Although structurally similar to diverticula of the small intestine, colon, and urinary bladder, they differ in their tendency towards folding and branching, a characteristic ascribed to the particular construction of the gall-bladder wall [23].
The diverticulum should not be confused with the folded gall bladders at the neck which many a times might mimic the former and the Hartmann’s pouch. Folded gall bladders are basically (i) kinking between the body and fundus – resulting in formation of retroserosal Phrygian cap or (ii) kinking between the body and infundibulum resulting in serosal Phrygian cap [8].
Hartmann’s pouch is a sacculation found in the neck of gall bladder [8]. It is frequent but inconstant feature of normal and pathologic human gallbladders. There is a significant association between the presence of Hartmann’s pouch and stones (p < 0.05). Adhesions between the cystic duct and the neck of the gallbladder are responsible for Hartmann’s pouch. Consequently, Hartmann’s gallbladder pouch is a morphologic rather than an anatomic entity [24].
This important anatomical as well as clinical entity poses a challenge for radiologists and laparoscopic surgeons and should be differentiated from other types of congenital anomalies and pathological states of gall bladder. It is interesting to note that true diverticula may or may not be involved in the pathology within the gall bladder although possible combination of diseases have been reported [1]. Association of diverticulum with non-specific prolonged ailments [18], acalculous cholecystitis [3], cholecystitis and cholelithiasis [4, 17], recurrent cholangitis [2] and carcinoma of gallbladder [5] have been reported in literature. It might press upon on the adjacent structures such as the duodenum or stomach. Rupture is a rare complication [1, 25]. It is not possible to assert whether these diverticula found in the present study were associated with particular clinical sign or symptoms related to this anatomical entity in the living state as the specimens were procured from cadavers, but no pathology was detected in these specimens.
Conclusion
In this cadaveric study, solitary diverticulum of the gall bladder, which is rare in itself, were found in nine (9%) out of hundred specimens. This entity might remain silent or might add to the considerable diagnostic and operative difficulties, especially in the presence of changes occurring as a result of the disease process itself. Knowledge of this entity is essential for radiologist and surgeons alike, for avoiding undue catastrophe at surgery and better management of patients suffering from ailments related to this important anatomical region.