An Unusual Type II Dens Invaginatus with Calcified Canals in a Maxillary Lateral Incisor – A Case Report
Arunajatesan Subbiya1, Nagarajan Geethapriya2, Angambakam Rajasekaran Pradeepkumar3, Paramasivam Vivekanandhan4
1 Professor, Department of Conservative Dentistry and Endodontics, Sree Balaji Dental College, Chennai, India.
2 Post Graduate Student, Department of Conservative Dentistry and Endodontics, Sree Balaji Dental College, Chennai, India.
3 Professor and Head, Department of Conservative Dentistry and Endodontics, Thai Mookambigai, Dental College, Chennai, India.
4 Professor, Department of Conservative Dentistry and Endodontics, Sree Balaji Dental College, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Arunajatesan Subbiya, Conservative Dentistry and Endodontics, Sree Balaji Dental College, Velachery Main Road, Pallikaranai, Chennai–600 100, India.
Phone: 9840197437,
E-mail: drsubbiya@gmail.com
Dens invaginatus is a developmental malformation resulting from the invagination of enamel organ into the dental papilla. Management of dens invaginatus is an endodontic challenge. Presence of calcified canals in dens invaginatus makes it even more complicated. Modification of the treatment plan is required to treat such cases. This case report deals with the management of a Type II Dens Invaginatus in a lateral incisor with calcified canals.
Dens in dente, Calcification, Endodontic treatment, Maxillary lateral incisor, Two canals
Introduction
Dens invaginatus is a rare developmental malformation of teeth resulting from the invagination of enamel organ into the dental papilla. Oehlers classified these defects according to their severity-Type l, confined within the crown not extending beyond the amelocemental junction; Type ll, an enamel-lined form which invades the root but remains confined as a blind sac. Type lll a form which penetrates through the root perforating at the apical area showing a ‘second foramen’ in the apical area [1].
Case Report
A male patient aged 16 years, reported to the dental clinic with the chief complaint of pain in left upper anterior region for the past 4 days. History revealed a trauma 2 years back. Clinical examination revealed pain on palpation and percussion in the upper left lateral incisor. No discoloration was present and the tooth did not respond to vitality tests. The tooth was wider mesio-distally but without any remarkable change in the lingual surface. Radiographic examination revealed a bulbous root with a periapical lesion in its relation to 22. Radiographic evidence of pulp chamber or root canal was absent, but there was a central circular radiolucency in the middle third of the root. It was provisionally diagnosed as dens invaginatus with calcified root canal of a non-vital lateral incisor.
Access cavity was opened under the rubber dam and the orifice of the invagination was located with an endodontic explorer towards the mesial aspect of the access opening. A radiograph was taken after negotiating the invagination with path finder. A constant search led to the orifice of the main canal. This canal was found to be calcified.
After carefully negotiating the invagination up to 10mm, the ISO #10 K-file was found to be buckling, as the file could not go through the calcified canal beyond the invagination. So, the coronal part was first enlarged up to size of 45. Groping of the apical surface of the invagination for a while, with a profinder, a small dip was felt with a tug back. This was identified as a possible entry into the apical part of the canal beyond the invagination. Careful wiggling of the profinder with a rotation not more than quarter turn resulted in a slow progress of the file into the canal. The apical movement was facilitated with EDTA (Ethylene Diamine Tetraacetic Acid) paste. The point of entry of the canal was memorized in the fingers by repeated short inward and outward movement into the apical part of the canal. This was done, so that the canal can be renegotiated, after the removal of instrument from the apical part of the canal. Once the apical part of the canal had been negotiated with slow and careful movement, a size 8 followed by size 6 file was used to reach the apex.
After scouting up to ISO #25 hand files, the canal was prepared up to #25 rotary NiTi files with 4% taper. The canal was copiously irrigated with 5.25% sodium hypochlorite and saline. A 30 gauge needle was taken up to the entrance of the apical part of the canal and irrigated so that the irrigant effectively reached the apical portion of the canal.
The main canal was negotiated carefully and was found to be joining the mesial canal at the apical third. This canal was then slowly enlarged up to #25 with 4% taper. After drying the canals with paper points, the invagination till the apex was obturated with thermoplastic gutta–percha and the other canal with #25, 4% tapered gutta–percha point using AH plus as sealer.
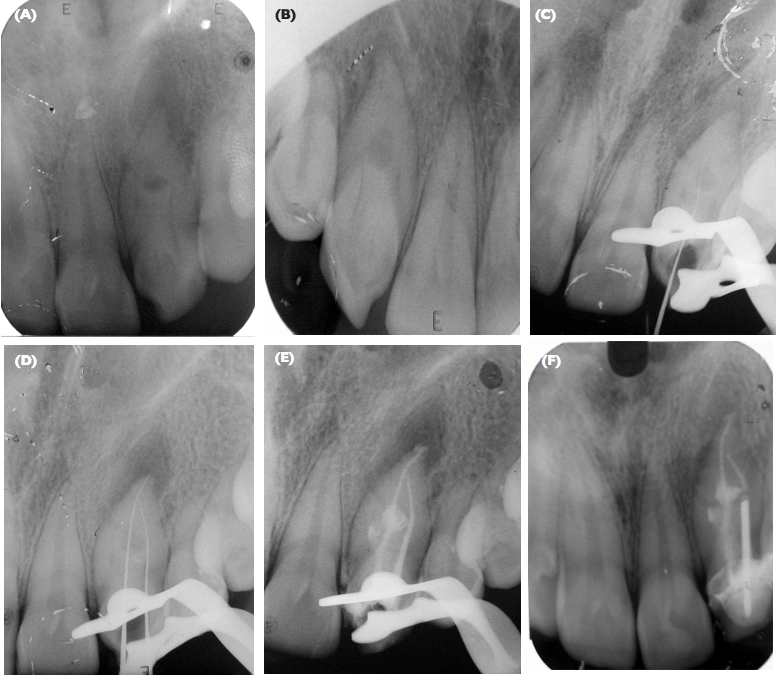
The patient returned asymptomatic after one week. A ceramic crown was given & he was periodically reviewed after 3 months and six months. The patient reported with fracture of the tooth due to trauma in 6 months. A pre–fabricated post was placed in the distal canal and a new crown was given. The radiograph was taken after one year showed a complete resolution of the lesion and the patient was asymptomatic [Table-Fig-1A-F] and [Table/Fig-2, 3].
A and B, Pretreatment radiographs of the affected tooth in different angulations showing complex internal anatomy. C, K-File not able to penetrate the canal beyond the internal resorption. D, Working length determination with instruments placed in two canals. E, Obturated canals. F, Follow up radiograph taken after one year showing resolution of the lesion.
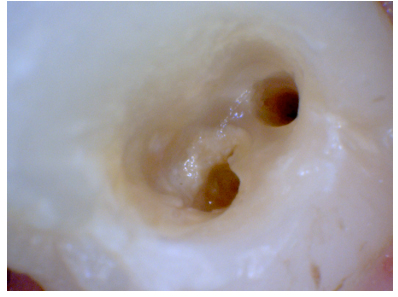
Access cavity showing two orifices located mesio-distally
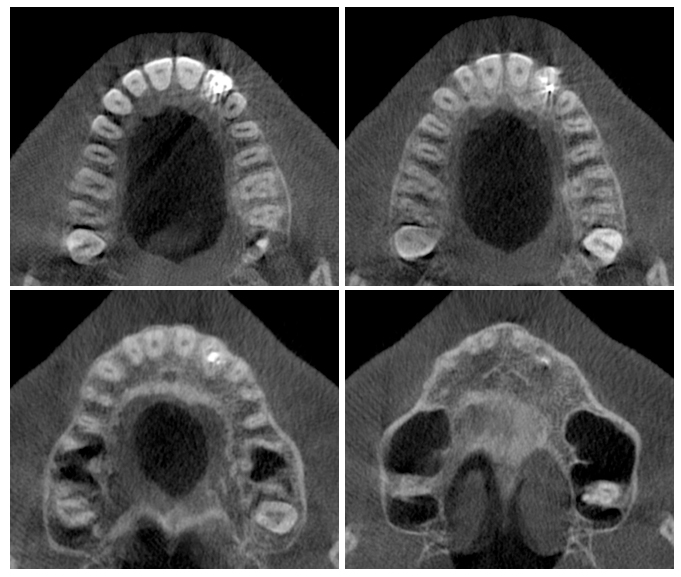
CBCT Images of the maxilla showing complete resolution of the periapical lesion in relation to upper left lateral incisor
Discussion
Knowledge of the complexity of root canal morphology and careful pretreatment evaluation of the radiograph is essential for diagnosing the unusual canal anomalies.
Focal failure of growth of internal enamel epithelium, infection, aggressive proliferation of internal enamel epithelium, distortion of the enamel organ during tooth development, fusion of two tooth-germs, trauma, deep folding of the foramen coecum during tooth development can be considered as aetiologic factors of DI. Generic factors and ectomesenchymal signaling systems can also contribute [2,3].
Dens invaginatus is often diagnosed by chance on the radiograph. As seen clinically, an unusual crown morphology including dilated, peg shaped or barrel–shaped crown or a deep foramen caecum may be considered as important hints in diagnosing DI.
The invagination allows entry of irritants into an area which is separated from pulpal tissue by only a thin layer of enamel and dentin and predisposes to the development of dental caries. In some cases the enamel-lining is incomplete. Channels may also exist between the invagination and the pulp [4]. Hallet introduced the term dens invaginatus to show that enamel is located centrally and the dentin peripherally due to the invagination [5].
Calcification occurs as a natural process of aging. But, it can also occur as a response to trauma or infection. In this case, trauma could be the reason for the obliteration of the root canal. According to Kronfeld, on eruption, the invagination will contain remnants of the dental papilla or periodontal connective tissue [6]. These elements become necrotic and become a nutrient rich environment following bacterial contamination. This case presents with a narrow invagination with a dental sac in the middle third of the root, which appeared as radiolucent area. This was a Oehler’s Type II Dens Invaginatus which communicates with the main canal. Some authors have described that, interruptions in the invaginated surface could potentially acts as a portal for irritants to the pulp [6]. Such irritation could also arise from the communication leading to stimulation of the cells in the pulp resulting in obliteration of root canal space. This case has become unique because, here calcification had occurred in a tooth with dens in dente.
Conclusion
Recognition of the developmental anomalies and complexities of root canals is essential for long term success in endodontic therapy. Modification of the conventional treatment procedure is often required for an unusual canal anatomy. This case report highlights the modification required for negotiating, cleaning and shaping a canal showing Dens Invaginatus type II and calcification which is different from managing a canal with either Dens Invaginatus or calcification alone.
[1]. Oehlers FA, Dens invaginatus-Variation of the invagination process and associated crown formsOral Surgery Nov 1957 10:1204 [Google Scholar]
[2]. Hulsmann M, Dens invaginatus: aetiology, classification, prevalence, diagnosis and treatment considerationsIntEndod J 1997 30:79-90. [Google Scholar]
[3]. Rushton MA, A collection of dilated composite odontomasBr Dent J 1937 63:65-85. [Google Scholar]
[4]. Alani A, Bishop K, Dens Invaginatus. Part 1:Classification, prevalence and etiologyInt Endod J 2008 41:1123-36. [Google Scholar]
[5]. Hallet GEM, The incidence, nature and clinical significance of palatal invaginations in the maxillary incisor teethProc Soc Med 1953 46:15 [Google Scholar]
[6]. Kronfeld R, Dens in denteJ Dent Res 1934 14:49-66. [Google Scholar]