Oral health is important to such an extent that it can hinder a person’s ability to work and concentrate on his routine. Dental problems can devastate a person’s physical as well as the psychological well–being.
Especially in the aged, oral problems are more chronic and severe as they have been always neglected in preference to other health problems. This tends to make them more irritable and to lose interest in life. Why oral health is so important? Does it really change the life of the elderly, and if so, in what ways? These are common questions which come to one’s mind when people talk about the ‘quality of life’ (QOL) in terms of oral health. Many researchers like Dolan [1] defined oral health broadly as “a comfortable and functional dentition which allows individuals to continue in their desired social role”. Cohen and Jago [2] called for a “sociodental indicator” or questionnaire that was capable of quantifying the impact of oral disorders from a psychosocial perspective, rather than from a biological perspective.
The population of the elderly, as well as the number of dependent elderly, is steadily increasing [3]. It is important to know the measures for improving their QOL, bringing solace and comfort in their lives.
The general health of the elderly gives an insight into their quality of life while the dental health also plays a very important role, as the dental problems interfere with the primary needs of life such as mastication of food, esthetics, speech etc. leading to irritability and loss of mental stability. At the same time, it gives rise to embarrassment when the appearance is affected. QOL is a dynamic and subjective blend of biological and psychosocial experiences influenced by our personal and sociocultural environments [4,5].
In the elderly, oral health status is generally poor due to several causative and controversial risk factors, and is usually characterized by increasing tooth loss, periodontal disease, and bad oral hygiene [6]. Various factors such as emotional issues, weak financial conditions, lack of family cooperation and awareness and multiple medication can worsen the oral health.
Health status, including oral health, is impacted by the interaction of four factors: (1) environment, (2) attitude/behavior, (3) public health services, and (4) genetics. For developing countries, the most important factors affecting oral health are environment and attitude/ behavior [7]. Attitude and behavior are one of the greatest influences on oral health status in developing countries, attitudes being emotionally charged pre–dispositions (positive or negative) to given object(s) or social situations, which persist over time [8]. Evans [9] reported that most elderly people hold negative attitudes towards oral health care, and that these attitudes will contribute to worsening oral health status.
The aim of the present study was to evaluate the problems in the elderly and their perception of dental well–being as a quality of life. At the same time the objective has been extended to assess the impact of oral health on the QOL.
Material and Methods
In this study a total of 63 patients were investigated before and after 6 months of their treatment. Institutional ethical board permission was acquired for conducting this study.
Sampling and data sources
The study was conducted and performed at SMBT (Sau. Mathurabai Bhausaheb Thorat) Dental College and Hospital in March 2012 and was carried out for 11 months.
Data was collected by giving questionnaires to the participants. They were briefed about the need and importance of precise information and made to fill the questionnaires. The first part of the questionnaire gathered the information regarding gender, age, marital and socio–economic status, education, monthly family income and dependency, while the second part comprised of different scales used to estimate the health ratings.
Participants
The participants were selected from the daily outpatient department, aged between 60–82 years. Informed consent was obtained from all the participants. The criterion for selection of subjects was completely edentulous status. Sample determination was done on the basis of monthly OPD of the institution for the complete denture category, which was 30–35 per month. We decided to restrict our sample size by stipulating the time period for a quarter of the year, which gave us 114 patients. After a thorough examination, there was a dropout of 39 patients on the ground of bad health while inability to attend the follow up visits made 12 to back out. Finally only 63 patients agreed and fulfilled the criterion for the study.
After 5 months the first interaction session was held where the selected patients were given two questionnaires, one, with a single item scale for assessment of the general health (National Health Interview Survey item) and the other one (GOHAI–12 converted to GOHAI–11 as the 12th item was excluded which was related to the sensitivity of teeth; present study is for edentulous subjects) before starting the prosthodontic treatment. The same questionnaire was administered again 6 months after completion of their treatment.
All the patients were treated in the special care department at SMBT Dental College and Hospital, by the specialists. Every step was assessed carefully to provide the best treatment to each and every participant patient. The dentures were delivered to the patients and a regular recall was attempted to check for any corrections if needed.
The scales of data collection
Oral Health–Related Quality of Life (OHRQoL) is measured by various scales, but GOHAI is one of the most commonly used scales in assessment of oral related quality of life in geriatric population. The data for this study is collected in different disciplines as follows:
I. Global self-rating scale: It was used for assessment of general health between the pre-treatment and the 6-month post-treatment period. Patients were asked to do self rating of their general health on the scale ‘excellent to poor’. This scale was given to all the participants before starting the treatment and 6 months after its completion. To estimate this rating, the patients were asked one single item; “In general, would you say your health is…” with the options excellent, very good, good, fair and poor. The score was calculated providing the information about the health. This is an item used in the National Health Interview Survey. In a number of studies self-rated health has been found to be an excellent predictor of future health.
II. GOHAI scale: The Geriatric Oral Health Assessment Index (GOHAI) consisting of 12 items, was developed by Atchison and Dolan [10] which was aimed at measuring the problems related to physiological, physical and psychological aspects. It measures the patient reported oral functional problems in a simple to administer manner. GOHAI gives greater weight to functional limitations and pain and discomfort, which are more immediate.
This questionnaire was given to the participants prior to the treatment at first visit. It consisted of 11 questions, with five Likert scale options, scoring as ‘often’, always’, ‘seldom ’or ‘sometimes’ and ‘never’ reflecting the aspects that are considered to have an impact upon the quality of life of the older population. As mentioned before, the 12th item that explains information about ‘sensitive to hot, cold or sweet foods’, was eliminated from this study after acknowledging its irrelevancy during the pilot study. It has been studied and pointed out that the questionnaire should include 11 questions only as per the relevancy of the study population. It could be relevant if many of those assessed were not totally edentulous [11]. In the year 2009, Shigli and Hebbal, conducted a study on elderly population in India, where the 12th question was not considered as all the patients were completely edentulous [12].
The GOHAI score is calculated by adding the score of the 12 items ranging from 0 to 60, (in present study it is calculated for 11 items). The scores were reversed for the three items ‘able to swallow comfortably’, ‘able to eat without discomfort’, ‘pleased with look of teeth’, so that a higher score was associated with a more positive oral health. Approximately 6 months following their final visit, the same questionnaire (GOHAI) was administered to the participants, which could provide us with the data as to what extent the patients’ quality of life was improved and the goal achieved.
Results
Statistical analysis
Qualitative data was represented in the form of frequency and percentages. Comparison between Pre & Post–treatment values of various scores was done with McNemar/ McNemar–Bowker Test.
Quantitative data was represented using Mean ± SD and Median, IQR (Interquartile range). Analysis of Pre & Post–treatment quantitative data was done using Wilcoxon Signed Rank Test as data were derived on a likert scale. A p–value, which was less than or equal to 0.05 (p< 0.05) was considered statistically significant. Results were graphically represented where deemed necessary. Data analysis was performed using SPSS V. 13 & MedCalc V. 11.3.3.0.
Demographic data
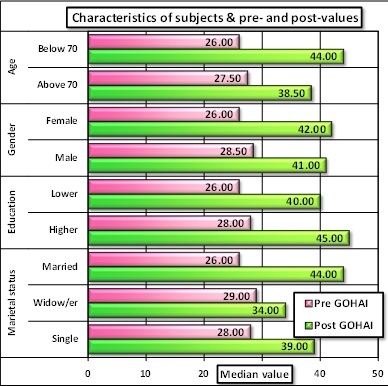
A comparative analysis was carried out among the demographic variables which were more significant in terms of age, gender, educational and marital status as long as the dental health was concerned. Subject characteristics are shown in [Table/Fig-1]. The age of the participants ranged from 60-82 years with the mean age 69.41. Out of total 63 participants, 55.6% were females while 44.4 % of them were males. The mean GOHAI score for females changed from 25.71± 7.45 to 41.00 ± 6.25 post–treatment, while in males it changed from 27.86 ± 10.00 to 38.68 ± 7.98. At the same time, the younger subjects who scored pre–treatment as 27.12 ± 8.60 abstracted higher post–treatment score i.e. 43.97 ± 3.93.The single and widows/ widowers were found to be having pre treatment GOHAI scores as 27.04 ± 8.89, which turned to 34.71 ± 6.92 post–treatment, on the contrary, married participants scored pre–treatment as 26.08 ± 8.24 and post–treatment as 43.83 ± 3.66.The GOHAI scores were noted to be higher in the higher education group 44.58 ± 4.07 than the lower groups 37.13 ± 7.12 [Table/Fig-1]. The difference from pre to post was statistically significant for all variables, except unmarried cases (p value=0.180) [Table/Fig-2].
Comparison of pre and post values
| Patient Characteristic | Frequency | GOHAI Score | Wilcoxon Signed Rank Test applied |
|---|
| | Pre | Post | Pre vs. Post |
| n | % (n=63) | Mean | SD | Mean | SD | z-value | p-value | Difference |
| Age | | | | | | | | | |
| Below 70 | 33 | 52.4 | 27.12 | 8.60 | 43.97 | 3.93 | -4.864 | 1.15E-06 | Significant |
| Above 70 | 38 | 60.3 | 26.17 | 8.87 | 35.57 | 7.26 | -3.840 | 0.00012 | Significant |
| Gender | | | | | | | | | |
| Female | 35 | 55.6 | 25.71 | 7.45 | 41.00 | 6.25 | -4.900 | 9.58E-07 | Significant |
| Male | 28 | 44.4 | 27.86 | 10.00 | 38.68 | 7.98 | -4.105 | 4.05E-05 | Significant |
| Education | | | | | | | | | |
| Lower | 39 | 61.9 | 26.00 | 8.07 | 37.13 | 7.12 | -4.773 | 1.81E-06 | Significant |
| Higher | 24 | 38.1 | 27.75 | 9.65 | 44.58 | 4.07 | -4.109 | 3.97E-05 | Significant |
| Marital status | | | | | | | | | |
| Married | 36 | 57.1 | 26.08 | 8.24 | 43.83 | 3.66 | -5.147 | 2.64E-07 | Significant |
| Widow/er | 24 | 38.1 | 27.04 | 8.89 | 34.71 | 6.92 | -3.211 | 0.00132 | Significant |
| Single | 3 | 4.8 | 30.67 | 14.19 | 35.67 | 12.34 | -1.342 | 0.180 | Not significant |
Characteristics of subjects and comparison of pre and post–treatment values
Self–rated general health score
It was assessed pre-treatment as well as 6 months post–treatment, by a single item questionnaire. There was only 5.55 % difference in the percentages when calculated excellent/ very good/ good vs. fair/poor (chi–sq uare value 0.522). The result for self rated general health was not significant statistically (p=0.470) [Table/Fig-3].
Changes in self-rated general health
| Scale | Pre–treatment | Post–treatment |
|---|
| No. | % | No. | % |
| Excellent ^ | 4 | 6.35% | 5 | 7.94% |
| Very good ^ | 8 | 12.70% | 10 | 15.87% |
| Good ^ | 20 | 31.75% | 23 | 36.51% |
| Fair # | 19 | 30.16% | 17 | 26.98% |
| Poor # | 12 | 19.05% | 8 | 12.70% |
| Total | 63 | 100.00% | 63 | 100.00% |
| McNemar-Bowker Test ^, # | Chi-Square Value | df | p-value | Difference is- |
| 0.522 | 1 | 0.470 | Not significant |
| Difference: 5.56%, 95% CI= -8.08% to 18.7% |
*(Test applied between ‘Excellent+V. Good+Good’ vs. ‘Fair+Poor’)
Responses to GOHAI Questionnaire
GOHAI scores were calculated by using an additive method, where the addition of GOHAI items was done (response set was always=5, often=4, sometimes=3, seldom=2, never=1) by combining them (a=always + often, b=seldom + sometimes, c=never).
GOHAI items and frequency distribution are shown in [Table/Fig-4]. As per the results, items 1, and 2, which describe the functional inability, scored highest. Majority of them i.e. 82.54 % (41.27 ± 2.25) respondents stated that they always or often had trouble biting and chewing the food (item 1), and about 80.95% (40.47 ± 14.59) respondents have noted that they always or often had trouble biting or chewing certain kinds of food, such as firm meat or apples (item 2). Incidentally, 36.51% (18.25 ± 14.59) of them always or often experienced problems swallowing food (item3). In response to item 4, 53.97% (26.98 ± 4.49) of the respondents quoted that they often or always had problems in speaking due to loss of teeth and dentures. The results are significant showing a clear-cut relationship between the first four GOHAI items which are related to functional problems in swallowing, speech and ingestion. The other two GOHAI items (item 5,and 8) describe the pain and discomfort, where about 49.21% of the respondents (24.60 ± 16.84) were not able to eat anything without discomfort, whereas about 36.51% (18.25 ± 7.86) participants agreed that they took medication for relieving pain and discomfort from around the mouth.
Percentage of patients reporting impact on quality of life prior to treatment and after 6 months
| Impact experienced due to problems with teeth, mouth or dentures | Per cent of patients reporting (n=63) [Frequency (%)] | McNemar-Bowker Test |
|---|
| (In the past three months) | Prior to treatment | 6 months after treatment | (Degree of freedom = 3) |
| a | b | c | a | b | c | Value | p-value |
| 1. Trouble biting or chewing | 52 (82.54) | 9 (14.29) | 2 (3.17) | 12 (19.05) | 16 (25.40) | 35 (55.55) | 40.143 | 9.94E-09 |
| 2. Limit the kinds of food | 51 (80.95) | 10 (15.87) | 2 (3.17) | 31 (49.21) | 22 (34.92) | 10 (15.87) | 21.000 | 0.00011 |
| 3. Problems to swallow comfortably | 23 (36.51) | 32 (50.80) | 8 (12.7) | 13 (20.63) | 29 (46.03) | 21 (33.33) | 15.273 | 0.002 |
| 4. Problems to speak clearly | 34 (53.97) | 17 (26.98) | 12 (19.05) | 16 (25.4) | 27 (42.86) | 20 (31.75 | 11.714 | 0.00843 |
| 5. Discomfort eating any kind of food | 31 (49.21) | 18 (28.57) | 14 (22.22) | 13 (20.63) | 32 (50.79) | 18 (28.57) | 13.560 | 0.00357 |
| 6. Limit contact with people | 22 (34.92) | 23 (36.51) | 18 (28.57) | 2 (3.17) | 14 (22.22) | 47 (74.6) | 28.000 | 8.32E-07 |
| 7. Pleased with look of teeth* | 2 (3.17) | 9 (14.29) | 52 (82.54) | 50 (79.37) | 11 (17.46) | 2 (3.17) | 56.333 | 3.57E-12 |
| 8. Used medication to relieve pain | 23 (36.51) | 30 (53.96) | 10 (15.87) | 10 (15.87) | 33 (52.38) | 20 (31.75) | 40.544 | 8.17E-09 |
| 9. Worried about teeth, gums or dentures | 29 (46.03) | 25 (39.68) | 9 (14.29) | 12 (19.05) | 19 (30.16) | 32 (50.79) | 40.810 | 7.18E-09 |
| 10. Self-conscious of teeth, gums or dentures | 20 (31.75) | 24 (38.1) | 19 (30.16) | 9 (14.29) | 14 (22.22) | 40 (63.49) | 12.996 | 0.0046 |
| 11. Uncomfortable eating in front of others | 43 (68.25) | 12 (19.05) | 8 (12.7) | 11 (17.46) | 13 (20.63) | 39 (61.9) | 37.530 | 3.55E-08 |
a. Impact reported ‘often’ or ‘always’(4+5); b. Impact reported ‘seldom’ or ‘sometimes’(2+3); c impact reported ‘never’ (1)
The rest GOHAI items describe the psychosocial aspect, where the appearance is an important criterion for the elderly, though it happens to be secondary, but obviously next to the function. The results were significant for all five items; where 34.92% (17.46 ± 2.25) respondents always or often limited contact with people because of the condition of their teeth and dentures (item 6), whereas17.46% (8.73 ± 5.61) of them were happy about their looks (item 7). This particular item is negatively scored as the participants were edentulous with missing all the teeth and so the appearance. The results revealed that about 46.03% (18.25 ± 7.86) respondents were often or always worried or concerned about the problems regarding their teeth, gums or dentures (item 9), while 31.74% (15.87 ± 6.73) respondents felt nervous or self conscious about their teeth, gums and dentures (item10). Another 68.25% (34.12 ± 10.10) stated that they felt uncomfortable eating in front of others (item 11) [Table/Fig-4]. These results are statistically significant and provide a clear picture about the functional, psychological and behavioral impacts of oral health in the elderly.
Change in GOHAI score
The GOHAI questionnaire was administered again 6 months after the treatment. The mean GOHAI was estimated and compared. An improvement in GOHAI score was observed 6 months after the participants received their new dentures. Patients who preferred the new prosthesis enjoyed a positive change in GOHAI scores. There was a statistically significant difference between participants’ satisfaction with the new dentures and change in GOHAI scores.
The results of the present study showed GOHAI scores increased from 28.90 ± 7.28 to 42.19 ± 7.60 which confirmed the significant change in GOHAI score from the pre–treatment time to the post –treatment period (p value< 0.001). Having a better GOHAI score was associated with having good dentures, where good implied the efficient mastication and the improved esthetic values. Though it did not make much change in a few, majority of them who were found to be satisfied with the treatment, have accepted that there was a difference in life before and after the treatment [Table/Fig-3].
Discussion
As per the present study, there was no significant difference between pre and post–treatment scores in self rated general health which showed that the improvement in dental health did not really have any impact on the general health status. Those who showed improvement to some extent were influenced more in psychological aspect, which certainly was improved after the treatment.
It was hypothesized that the younger subjects would have better GOHAI scores than the older subjects. Respondents who were better educated had higher GOHAI which clearly indicates a relatively better socio–economic status and awareness. There was significant difference between males and females with better GOHAI scores in females, which points out that females had higher acceptance of prescribed treatment. Marital status showed high impact on the QOL of elderly, as it was seen that the married subjects showed higher GOHAI scores than the single and widow/widowers. This was hypothesized again as the psychological well–being and companion support in life as a ‘feel good’ factor.
Majority of people above 60 years are lonely or dependant. As per the government data, about 65% of the aged had to depend on others for their day–to–day maintenance. Less than 20% of elderly women but majority of elderly men were economically independent. Among economically dependent elderly men 6-7% were financially supported by their spouses, almost 85% by their own children, 2% by grand children and 6% by others. Out of elderly women, less than 20% depended on their spouses, more than 70% on their children, 3% on grand children and 6% or more on others including the non-relations [13].
Many studies have documented that the overall health of the elderly was related to their oral health and vice versa. It is rightly said that, access to appropriate oral health care is likely to improve overall quality of life [14]. It has been observed by various researchers that oral health plays an important role in maintaining the general health not fully but to a certain extent. A study by Jenson (2008) states that, oral health related quality of life is associated with some (perceived need for dental treatment, poor self–rated health, worse mental health, fewer teeth, and relatively poor cognitive status) but not all (e.g., ADL (activities of daily living) and instrumental ADL dependence) measures of oral health, health, and disability status and not with life satisfaction, living alone, or low income [15]. On the contrary, as per Mack et al., prosthetic status has significant effect on the physical index of general health related quality of life. The reduced dentition without replacement of missing teeth by removable or fixed prosthodontics reduces the physical index of quality of life to the same extent as cancer or renal diseases [16]. One more study revealed that the general health–related quality of life was improved in the elderly patients who were treated by giving the implant supported mandibular overdentures [17].
A similar study [12], analysed 27 patients from the age group 60 – 84 where the GOHAI score was seen to be increased from 27.48 to 30.19 (p=0.002) which was highly significant; whereas the present study examined 63 patients from the age group 60-82, where the GOHAI score was seen to be increased from 28.90 ± 7.28 to 42.19 ± 7.60 (p value< 0.001) which was highly significant.
Though there are differing results on relationship between OHRQoL and general health, there are definite results for compromised dental conditions and OHRQoL. A study investigated the masticatory performance with oral health-related quality of life in independently living elderly Japanese subjects. It suggests that the masticatory performance has a direct influence on the quality of life [18].
Patient satisfaction is always related to their level of acceptance of the dental treatment which directly depends on their emotional and mental status. Sometimes the elderly require time to accept things which are new to them. Due to some reason, the elderly sometimes face depression which can negatively affect their physical functioning and well-being, which in turn affects their oral functioning. Individuals with more depressive symptoms reported worse oral quality of life, controlling for sociodemographic factors and self-reported oral health [19].
Though the quality of life for the elderly is assessed by many, there are very few studies conducted to assess the quality of life in completely edentulous population in India. GOHAI is translated in various languages; it was translated in Hindi by Deshmukh and Radke [20] to assess its validity and reliability for use among people in India and was proved to be a valuable instrument for measuring oral health-related quality of life. Oral health-related quality of life and nutritional status of institutionalized elderly population was studied in Mysore City, India, by using GOHAI data and their association with the Mini Nutritional Assessment (MNA) results to assess the relationship between oral health and malnutrition [21].
The present study evaluated the need of investigation before and after the prosthodontic care which can provide the exact picture of whether the elderly have been provided a better quality of life. It was noticed that the patients expected more attention and psychological support by the clinicians in the institutions. There is a need to understand the responsibility of the entire dental fraternity to acknowledge the problems of elderly and treat them so that it adds to their QOL.