Smoking habit has been reported in almost 1.3 billion people around the world, which is associated with discolouration of teeth and prostheses. Acrylic resin teeth are the popular choice of prosthetic teeth in removable dentures. Therefore, the effect of cigarette smoke on the colour stability of commercially available acrylic resin teeth needs to be evaluated for clinical success.
Materials
Three Brands of commercially available acrylic resin teeth were selected. 20 upper left central incisors of each brand were selected randomly and grouped as Groups A (Premadent), B (Astra) and C (Sanyo-dent) respectively.
Specimens of each group were then divided into 2 subgroups (10 specimens each), as specimens which were not exposed to cigarette smoke i.e. control group (Sub-group1) and specimens which were exposed to cigarette smoke i.e. study group (Sub-group 2).
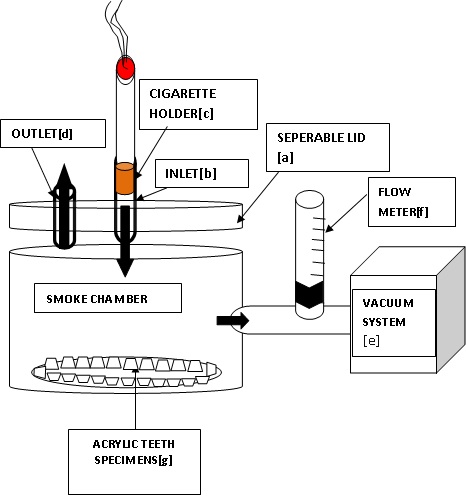
Custom made smoke chamber: It was made of insulating material. It had a separable lid [a], which when in place, closed the chamber hermetically. Volume of smoke chamber was kept as minimum as possible. For entry of cigarette smoke; an inlet [b] was designed at the centre of the lid of the chamber to fit cigarette holder [c] in which lit cigarette could be snugly fitted. Another opening of same diameter was made on the periphery of the lid of the chamber, as an outlet for smoke [d].
To mimic the process of smoking in-vivo -
The smoke chamber was connected to a vaccum system [e] through a control for vaccum system [h], which was adjusted to maintain a steady flow rate of 30 cm3/s of smoke and a flow meter [f] to monitor the same.
For active filling of cigarette smoke in smoke chamber, outlet[d] was closed and vaccum system was switched on for 2 sec, so as to mimic active inhalation of smoke in-vivo (puff duration).
To maintain passive exhaust of smoke, outlet [d] on lid was left open for 60 sec before the next smoke cycle was performed, so as to mimic passive exhalation of smoke in-vivo.
Arrangement of specimens [g]: Inside the chamber, arrangement was made in such a way that the labial surfaces of all the specimens were arranged as facing towards the inlet.
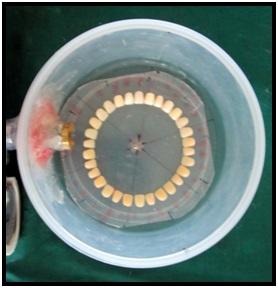
For equal exposure of all specimens to cigarette smoke, specimens were fixed at equal distances from inlet. For that.
They were fixed with carding wax in a circular manner on separate sheets at the bottom of the chamber, in such a way that the centre of the circle and the chamber coincided.
The 3 brands were also sequenced alternatively as A-B-C-A-B-C.
Further, the sheet was rotated by 60° angulations, horizontally, 6 times daily.
All 60 specimens were then stored in artificial saliva at 37°C for 24 hours to simulate clinical conditions. After 24 hours, baseline colour measurements of all specimens were performed by using a spectrophotometer, according to the CIELAB colour system [1]. Specimens from sub-group 2 were then exposed to tobacco smoke of 6 cigarettes [2] daily for 21 days [1,3] in a smoke chamber [4,5]. For each cigarette, 9 puff cycles were carried out. Each cycle contained a puff duration of 2 seconds [6] and a puff frequency of 1 puff every 60 seconds [6].
After each cycle of exposure, specimens were washed with distilled water for 1 min and they were then immersed in the artificial saliva (37°C). Control group specimens were stored in artificial saliva at 37°C for same time period of 21 days.
After a period of 21 days, colour measurements were performed in the same way as baseline colour measurements were performed. Before measurement, each specimen was rinsed with distilled water for 1 minute and dried with adsorbent paper. The total colour variation (E) was calculated before and after staining [Table/Fig-1,2,3,4 and 5].
Study group specimens inside smoke chamber and 6 division markings of smoke chamber
Smoke chamber with vaccum system

Smoke chamber filled with smoke


Results and Statistics
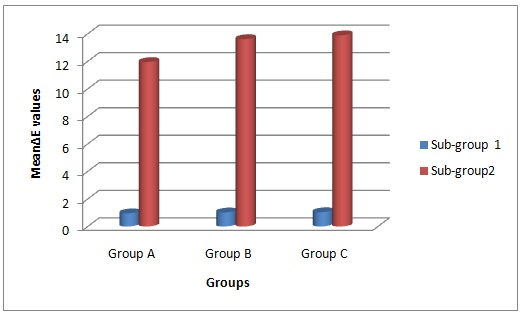
[Table/Fig-6] shows Comparison of mean change in E values of Group A, Group B and Group C specimens.
Comparison of mean change in ΔE values of Group A, Group B and Group C specimens.
| Group | Sub-Group | Mean | Std. Deviation | N |
|---|
| Group A | A1 | .9551 | .21334 | 10 |
| A2 | 11.9481 | 2.47108 | 10 |
| Total | 6.4516 | 5.89201 | 20 |
| Group B | B1 | 1.0198 | .19275 | 10 |
| B2 | 13.6106 | 2.97498 | 10 |
| Total | 7.3152 | 6.77699 | 20 |
| Group C | C1 | 1.0374 | .24138 | 10 |
| C2 | 13.8882 | .96288 | 10 |
| Total | 7.4628 | 6.62763 | 20 |
| Total | Sub-group 1 | 1.0041 | .21221 | 30 |
| Sub-group 2 | 13.1490 | 2.38509 | 30 |
| Total | 7.0765 | 6.34962 | 60 |
[Table/Fig-7] shows Results of Two-way ANOVA for comparison of mean change in E values of Group A, Group B and Group C specimens after 21 days, which were relative to baseline values.
Results of Two-way ANOVA for comparison of mean change in ΔE values of Group A, Group B and Group C specimens after 21 days, relative to baseline (p<0.05)
| Source | Type III Sum of Squares | Df | Mean Square | F | Significance |
|---|
| GROUP | 11.935 | 2 | 5.967 | 2.234 | .117 |
| SUBG | 2212.466 | 1 | 2212.466 | 828.387 | .000 |
| GROUP * SUBG | 10.119 | 2 | 5.060 | 1.894 | .160 |
| Error | 144.224 | 54 | 2.671 | | |
| Total | 5383.372 | 60 | | | |
| Corrected Total | 2378.743 | 59 | | | |
The results of the study indicated that,
On comparing staining after exposure to cigarette smoke to staining after immersion in artificial saliva, a higher mean total colour change was observed on exposure to cigarette smoke, which was statistically highly significant and clinically not acceptable.
On comparing 3 groups, an increase in mean total colour change was observed for all groups. Group C showed maximum mean total colour change, followed by Group B and least mean total colour change was observed with Group A.
In control group, after immersion in artificial saliva, a slight increase in total colour change was observed in all groups, which was clinically acceptable.
[Table/Fig-8] depicts Comparison of mean change in E values of Group A, Group B and Group C specimens after 21 days, which were relative to baseline values.
Comparison of mean change in ΔE values of Group A, Group B and Group C specimens after 21 days, relative to baseline
Discussion
Exogenous sources of discolouration of resin based materials were present in the patient’s diet or they had resulted from the smoking habit [1]. In dental literature, the staining of various aesthetic dental materials like composite resin [1,3–5,7] and maxillofacial silicone [8] by cigarette smoke has been reported,. Also, there is a good amount of literature which have reported staining which was caused by food colourants, like staining of artificial teeth [9,10], aesthetic restorative materials [11,12], denture base resin [13] and acrylic resins for provisional restoration [14]. Some authors had evaluated colour stabilities of denture teeth as was affected by both polymerization methods and thermal cycling [15].
However, available literature lacks information on staining of acrylic resin teeth by cigarette smoke, which is one of the commonly used tobacco forms. Against this backdrop of information scarcity, this in vitro study was undertaken, to analyze the effect of cigarette smoke on colour stabilities of 3 brands of commercially available acrylic resin teeth.
Main constituent of tobacco, which causes staining, is ‘tar’.1 Tar is the particulate matter which is inhaled when the smoker draws on a lighted cigarette. Approximately 0.2% of the tar composition is represented by brown pigments [3].
Other than the tar, thermal effects of the smoking habit might be another area of concern [1,16]. Thus; in this study, smoking chamber was of minimum possible volume and of insulating material, to better reproduce the temperature that is actually produced inside the mouths of smokers.
According to Coresta Recommended Method N° 226, standard conditions which were used were as follows:-
Puff Duration- 2.0sec, with a standard deviation of ≤0.05sec for individual puffs.
Puff Frequency- 1 puff every 60sec with a standard deviation of ≤0.5sec.
Maximum flow rate- 25 cm3 sec-1 to 30 cm3 sec-1
According to Graça LM [2] et al, chronic smokers smoke a minimum of 6 cigarettes per day. So, in present study, 6 cigarette smoking cycles were carried out per day. Strasser A, et al. [17] reported a strong positive correlation between number of puffs and intensity of tar stain.
To detect colour change, instrumental techniques are preferred, as they eliminate the subjective interpretation [9,15,18,19]. Among them, spectrophotometers are preferred, as they can generally provide more systematic, reliable and precise measurements [15]. On the downside, this approach has some disadvantages. Systemic errors can occur on more curved or on translucent specimens [20]. So, to overcome these problems, teeth with relatively flat surfaces were chosen and measurements were made from less translucent midlabial surfaces.
Spectrophotometers often report colour by using the CIELAB colour system, which represents the international standard for colour measurement. It is currently one of the most popular and widely used colour spaces. It is well suited for the determination of small colour differences [9]. American Dental Association (ADA) recommends the use of this system.
In this system, any colour is a combination of 3 spatial co-ordinates, which are designated as L*, a* and b*.
L* represents the brightness of a shade and its value ranges from 0 (blackest) to 100 (whitest).
Value in postion(+) Value in negative(-)
a*(amount of red-green colour) Shift towards red region Shift towards green region
b*(amount of yellow-blue colour) Shift towards yellow region Shift towards blue region
This colour system has a meaningful correlation with the visual perception and clinical significance of colour differences [9,15,21].Thus, CIELAB measurements evaluate the colour of each specimen at a given time and they also enable the calculation of the amount of colour change (ΔE) between two time intervals by using a formula:

Where, ΔL*, Δa* and Δb* are the differences in L*, a* and b* values which are measured before and after exposure to cigarette smoke. ΔE is the shortest distance in the CIELAB colour system between the colours which are compared [22].
In dentistry, a discolouration that is more than visually perceptible (ΔE > 1.0)[10] will be referred to as clinically acceptable, up to the E value of 3.3 [5,15,23,24]. A discolouration which is above this level is referred to as unacceptable in subjective visual evaluations [23].
Among denture teeth, resin teeth are known to have sidelined ceramic teeth in the market recently [9]. On the downside, conventional acrylic teeth are inferior to porcelain teeth in maintaining an adequate aesthetic appearance with wear and discolouration, and they thus have a shorter durability period and service life [9]. To overcome these problems, high-strength acrylic teeth have since been developed. They are made of crosslinked resin. Since they are still susceptible to staining with pigments, it has been observed that the aesthetics of dentures which are made from such acrylic teeth are gradually impaired [9]. So, both conventional and crosslinked types of acrylic resin teeth were taken up for this study, considering that presence and/or degree of crosslinking might affect the degree of discolouration.
In the crosslinked type of acrylic resin teeth, the gingival or body portion may not be as highly cross-linked as the incisal or occlusal portion [24,25]. So, in this study, mid labial surface was chosen for colour analysis.
It has been pointed out in previous literatures which had reported on aesthetic dental materials that, the lighter materials discolour more markedly than darker ones. So, teeth of lighter shade were selected.
Results of this study were consistent with those of studies which were done by Mathias P, et al., [1] Wasilewski MA, et al., [5] and Mathias P, et al., [7]. These studies had evaluated the effect of tobacco smoke on the colour of composites.
A small colour change occurred in all control group specimens, which was relative to baseline, this was assumed to be due to the thermal effect of the immersion temperature and/or due to water absorption [26] and/or due to mucin, which is one of the components of the artificial saliva [3].
According to Craig [24], polymeric teeth are insoluble in oral fluids, but they are soluble to some extent in aromatic hydrocarbons. According to Mathias P, et al., [7] tar contains aromatic hydrocarbons. So, it was deduced from this study, that such surface dissolving substances may be causative factors of discolouration.
Also, there was a possibility that the cigarette smoke mixed saliva may have produced an acidic pH solution, which might have damaged the surface integrity of the materials, thus producing favourable conditions for discolouration.
According to Assunção, et al., [15] acrylic resin teeth which show less colour change, may have a higher degree of cross-linking than the others. The results of present study showed that conventional teeth got more discoloured. So, the inference of this study is that, the presence and/or degree of crosslinking may be the factor/s which affect degree of discolouration inversely.
According to Mutlu-Sagesen L, et al., [10] less colour stability of acrylic denture teeth could be explained by the water sorption property.
According to Mathias P, et al., [1] irregular surfaces can be easily pigmented. Also, they stated that surfaces became more stained after being submitted to thermal variations. In the same study, authors mentioned that the staining susceptibility seemed to be related to intrinsic factors. Intrinsic factors include loss of fillers and matrix, which might happen following a period of storage in water or saliva [1]. According to Craig [24], in polymeric teeth/acrylic resin teeth, fillers can be added to increase resistance to wear. So, it could be deduced that the cause for discolouration in the present study might have been loss of fillers from polymeric teeth.
Colour change may alter the organic matrix. Inhibition, hydrolysis, and breakdown of polymeric chains may result in division of main chains and separation of cross-linking. The teeth which were evaluated in this study may have had different quantities of cross-linking agents, which might explain the variation in colour change for each brand of artificial teeth [15].
Limitations of the Study
Between the daily exposure intervals, the experimental tooth specimens were not subjected to any cleaning procedure. In vivo cleaning action, continuous flow of saliva and pressure drop were not taken into consideration, which may not accurately reflect clinical conditions. To overcome this, an in vivo evaluation is needed, which is ethically unacceptable. Hence, this in vitro study was done. Thus, the results which have been obtained herein, may serve in revealing the consequences of a low quality denture care.
Conclusion
A marked increase in total colour change of acrylic resin teeth was observed for all groups on exposure to cigarette smoke, which was statistically highly significant and clinically not acceptable.
On comparing 3 groups, Group A (crosslinked acrylic resin teeth) was found to be more colour stable and more resistant to the discolouration which was caused by cigarette smoke, followed by Group B (crosslinked). Group C (non-crosslinked) was least colour stable and most susceptible to discolouration which was caused by cigarette smoke.
It can be deduced from above results that presence of crosslinking in acrylic resin teeth might increase resistance to discolouration.
Clinical implication of this study is that when long term maintenance of the matched colour for the entire length of its service life is required; the smoking habits of the patients must also be considered, while the commercially available acrylic resin teeth are being chosen and patients should be advised against excessive cigarette smoking. Also, manufacturers of acrylic resin teeth can make necessary changes in composition and manufacturing process, to increase colour stability of acrylic resin teeth.