A chondroid syringoma or a mixed tumour of skin, is a rare, benign skin adnexal tumour of sweat gland origin, which is most commonly seen in the head and neck region of patients who are in the sixth and seventh decades. These tumours usually present as asymptomatic, slowly growing masses. We are reporting a rare case of a chondroid syringoma of Rt. ala nasi in a 50 years old female. The swelling had started 4 years back as a small nodule and it had gradually increased in size to 2x2 cms. It was located subcutaneously and it was projecting into the anterior nares. A clinical diagnosis of a benign adnexal tumour (adenoma) or a solitary neurofibroma was made and an excision was planned. Histopathology revealed features of a chondroid adenoma. We are reporting this case because of its rare and unusual site of occurrence and so far, in the available literature, no such case has been reported on tumours of alanasi.
Introduction
A chondroid syringoma, an uncommon skin adnexal tumour which is of sweat gland origin, is also referred to as a cutaneous mixed tumour, because it consists of both epithelial and myoepithelial cell types. The incidence of chondroid syringomas among primary skin tumours is low and it is usually seen in the middle aged and older male patients as small, single dermal or subcutaneous nodules in the head and neck area. A malignant transformation is very uncommon [1,2]. No characteristic clinical features are seen and so, a definite diagnosis can be made only by doing a histopathological examination. We are presenting this case because of its rarity and unusual site of occurrence (ala nasi).
Case Report
A 50–year–old female presented with an asymptomatic, slowly growing painless swelling in the right alanasi, which had a duration of 4 years. She was referred from the ESI hospital with a diagnosis of ? a tumour of vascular origin or a sebaceous cyst. She had no history of trauma. Her physical examination revealed a firm, painless and a mobile nodule which was of size, 2 x 2 cm, which was covered by skin and was located in the right alanasi, which projected into the anterior nares without any overlying skin changes [Table/Fig-1]. A clinical diagnosis of a benign adnexal tumour (adenoma) or a solitary neurofibroma was made. An excision was done through an incision in the alar crease. The tumour was carefully separated from the overlying skin and the nasal mucosa, without damaging the true capsule and the tumour could be shelled out completely. After trimming the redundant skin, the skin was closed along the alar crease. The integrity of the alar base and alar rim and tip of the nose was maintained. The subcutaneous nodule was subjected to histopathology and a clinical diagnosis of an adenoma was made.
Preoperative photograph showing well circumscribed nodule over ala nasi

Gross examination revealed a grey white nodule which measured 2 x 2 cm, which was firm in consistency. Cut section showed an encapsulated solid grey white appearance with focal translucent areas [Table/Fig-2].
Gross and cut surface showing encapsulated solid gray white translucent areas with tiny cystic spaces

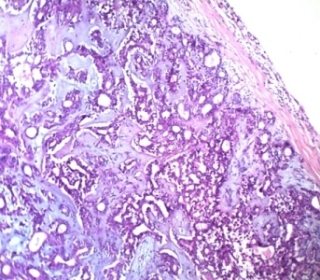
Histopathologic examination revealed a well- encapsulated lesion which was composed of numerous, small, non branching tubules which were set in a myxoid and cartilaginous stroma [Table/Fig-3 & 4]. Based on this morphology, a definitive diagnosis of a chondroid syringoma was made.
H&E X10 showing encapsulated biphasic tumor composed of epithelial and mesenchymal elements
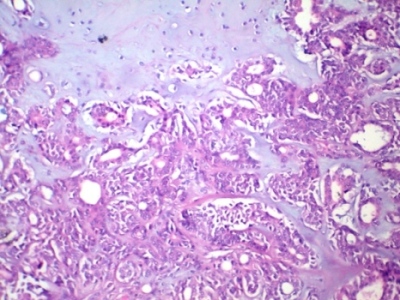
H&E X40 showing biphasic tumor with epithelial component arranged in tubules and sheets admixed with chondromyxoid background
Discussion
A chondroid syringoma, which is also known as a mixed tumour of the skin, is a rare, benign adnexal tumour of sweat gland origin, which is composed of both epithelial and mesenchymal components and it is histologically similar to benign mixed tumours of salivary glands [3]. The aetiopathogenesis of these tumours is unknown, but some authors suggest the hypothesis of an epithelial and a mesenchymal origin [2–5].
The first case is believed to have been reported by Nasse et al., in 1892. In 1961, Hirsch and Helwig reported a large series in which they coined the term, ‘chondroid syringoma’ for these tumours, owing to the presence of a sweat gland like epithelial component and frequent cartilaginous like stroma. They proposed the following five histological criteria for diagnosis: 1. Nests of cuboidal or polygonal cells; 2. Interconnected tubuloalveolar structures which were lined with two or more rows of cuboidal cells; 3. Ductal structures which were composed of one or two rows of cuboidal cells; 4. Occasional keratinous cysts and 5. A matrix of varying composition. Chondroid syringomas may have all five characteristics or they may manifest only one characteristic [1].
In 1961, Headington recognised 2 types, apocrine and eccrine. The apocrine type demonstrates irregular branching tubules (tubulocystic pattern) which are lined by at least a 2 cell thick epithelium. The eccrine type is charecterised by rather uniform, small, round tubules that are evenly spaced within a myxoid–chondroid matrix.
The reported incidence of chondroid syringomas among primary skin tumours is less than 0.01% and a greater incidence of 0.098% was reported by Yavuser et al., Lesions are typically located on the head and neck, and they are are non-ulcerating, slowly growing and subcutaneous or dermal nodules [1–4]. However, Sungur et al., reported a benign tumour where rapid growth, ulceration, and necrosis were evident at the tumour site [6]. These tumours have also been reported in other parts of the body, which include the chest, abdomen and extremities. Rarely, they are located on the scrotum, eyelids or orbits [7].
It was reported from the Department of Pathology of Gazi university, Ankara, Turkey, that among 16,200 excised skin lesions (during 1986 to 2002), there were 16 cases of chondroid syringomas. Department of Pathology, Gaziantep School of Medicine, Turkey, reported 13 cases of benign chondroid syringomas among 1921 skin lesions (during 1995 to 2001) and 10 which were situated in the head and neck region. Henry Ford Hospital reported 25 cases of chondroid syringomas from Surgical Pathology files of 1985 to 1997.
Chondroid syringomas may be confused clinically with various skin lesions which include benign tumours of epidermal or mesenchymal appendages like dermoid or sebaceous cysts, neurofibromas, lipomas, etc.
Although most are benign, malignant forms have been reported [6,8]. Unlike its benign counterpart, the malignant form occurs predominantly in females, it has no age related predilection, and it is observed more commonly in the extremities. Histological findings such as cytological atypia, infiltrative margins, satellite tumour nodules, tumour necrosis, and involvement of deep structures are considered as signs of a malignant transformation [2,5].
Because of its malignant potential, complete excision of a chondroid syringoma must be done. The patient should be followed carefully for both local recurrence and metastasis.
Conclusion
We are reporting this case because of its rarity, particularly its location in the nose and ala nasi. So far, no such case has been reported in the world literature. A skin incision was made along the natural alar crease line and with a careful dissection, the tumour, could be completely and successfully excised without disturbing the aesthetic appearance of the nose.
Histologically, chondroid syringomas share similarities with pleomorphic adenomas, which are mixed tumours that arise from the salivary glands. In contrast to pleomorphic adenomas, chondroid syringomas arise from sweat glands.
Optimal treatment of benign chondroid syringomas is surgical excision. Fine needle aspiration cytology has been used for diagnostic purposes and it may prove to be useful, to determine pathology before excision. However, examination of the excised tissue is most reliable in establishing a definitive diagnosis.
Chondroid syringomas are rare and usually benign and most often, they are seen in the head and neck region. This tumour should be included in the differential diagnosis of cutaneous head and neck tumours, especially in middle aged individuals and a close follow-up is recommended, to check for chances of recurrence and a risk for malignant transformation.
[1]. Hirsch P, Helwig EB, Chondroid syringoma. Mixed tumor of skin, salivary gland typeArch Dermatol 1961 Nov 84:835-47. [Google Scholar]
[2]. Yavuzer R, Basterzi Y, Sari A, Chondroid syringoma: a diagnosis more frequent than expectedDermatol Surg 2003 Feb 29(2):179-81. [Google Scholar]
[3]. Mills SE, Mixed tumor of the skin: a model of divergent differentiationJ Cutan Pathol 1984 11:382-86. [Google Scholar]
[4]. Sungur N, Uysal A, Gumus M, Kocer U, An unusual Chondroid syringomaDermatol Surg 2003 29:977-9. [Google Scholar]
[5]. Bates A W, Baithun S I, Atypical Mixed Tumor of the Skin: histologic, immunohistochemical, and ultrastructural features in three cases and a review of the criteria for malignancyAm J of Dermatopathol 1998 20:35-40. [Google Scholar]
[6]. Sheikh SS, Pennanen M, Montgomery E, Benign chondroid syringoma: report of a case clinically mimicking a malignant neoplasmJ Surg Oncol 2000 Apr 73(4):228-30. [Google Scholar]
[7]. Kaushik V, Bhalla RK, Nicholson C, de Carpentier JP, The chondroid syringoma: Report of a case arising from the external auditory canalEur Arch Otorhinolaryngol 2005 262(10):868-70. [Google Scholar]
[8]. Harrist TJ, Aretz TH, Mihm MC, Jr., Evans GW, Rodriquez FL, Cutaneous malignant mixed tumorArch Dermatol 1981 Nov 117(11):719-24. [Google Scholar]