Peculiar Case of Mucocele of Appendiceal Tip
Sridhar M.1, Narayanaswamy Chetty Y.V.2, Bagalibaba Saheb3
1 Assistant Professor, Department of Surgery, M.S. Ramaiah Medical College, Karnataka, India.
2 Associate Professor, Department of Surgery, M.S. Ramaiah Medical College, Karnataka, India.
3 Professor of Surgery, Department of Surgery, M.S. Ramaiah Medical College, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sridhar M., No. 181, 11th cross, 3rd main, HIG colony, RMV 2nd stage, Bangalore, Karnataka–560094, India.
Phone: 9880190880,
E-mail: dr.sridhar.m@gmail.com
Mucocele of Appendix is a gross or clinical descriptive term for dilatation of the appendiceal lumen by mucus.It is a rare pathology with an overall incidence of 0.2 to 0.3% of all appendectomies. Majority of these cases present with mucocele involved whole length of the appendix. On extensive literature search,exact incidence of mucocele confined only to the tip of appendix is not known, though there are very few case reports. Here we report a peculiar case of large mucocele of appendix confined only to the tip, sparing significant length of proximal appendix and causing diagnostic dilemma pre-operatively in a 43 –years –old lady.
Mucocele, Appendiceal tip, Appendix
Case Report
A 43 –years –old lady presented to us with history of pain abdomen, in right lower quadrant of the abdomen with history of occasional fever since one year. There was no history of any other gastrointestinal, urinary or menstrual symptoms. There was no significant past history. On examination, patient had flat and soft abdomen. There was a solitary, mobile, non-tender, firm mass palpable in the right iliac region, measuring about 10x8 cm with smooth surface. Mass was intra–abdominal & intra–peritoneal. Patient’s ultrasound examination reported as mass appearance in close proximity to ascending colon, probably a colonic mass or intussusception. CT scan of abdomen reported as large peripherally calcified cystic mass lesion in close appreciation to ascending colon with probability of hydatid cyst or mucocele of appendix. Patient was subjected for diagnostic laparoscopy which revealed a large tense cystic mass in the paracaecal region, adherent to caecum and ascending colon.With the probability of either hydatid cyst or mucocele of appendix as per CT abdomen, to avoid inadvertent injury and spillage of the mass, we decided to convert to open procedure. On laparotomy, after careful dissection, we found a well circumscribed mass, measuring 11x8 cm, arising from only the tip of appendix. Surprisingly, proximal 8 cm from the lesion till the base of the appendix looked absolutely normal. There was no evidence of mesenteric lymphadenopathy or free fluid. Open Appendectomy without rupturing the wall of appendix was done. Histopathological examination of the specimen revealed benign mucocele confined to the tip of appendix, without any evidence of obstruction or malignancy in the proximal part. The patient was followed up regularly for one year without any untoward findings [Table/Fig-1 and 2].
Intra–operative image of mucocele at the tip of appendix

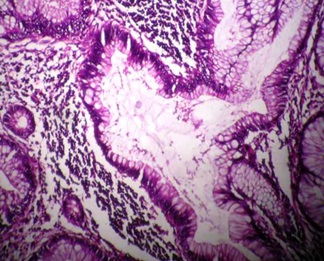
Histopathology picture showing hyperplastic and dilated mucus glands with mucin (200x)
Discussion
Mucocele is a term given to a group of appendicular lesions characterised by one or more of the following features: (1) dilatation of the lumen; (2) alterations of mucosal lining; (3) hyper secretion of mucous; and (4) occasional extension outside the appendix, either as peritoneal implants or, exceptionally, as distant metastasis [1]. It is caused by both benign and malignant pathologies in the appendix. Mucinous cystadenoma and cystadenocarcinoma account for 60-70% of all mucoceles. Rare causes are retention cyst, mucosal hyperplasia, carcinoid, appendicolith, endometriosis, adhesions, post inflammatory scarring, age-related atrophy, congenital obstruction of Gerlach’s valve, extra-mural compression and volvulus [2].
Majority of the appendiceal mucocele cases reported in literature described mucocele involving whole length of appendix. There are few case reports of mucocele of appendix sparing the base. However, exact incidence of mucocele involving only the tip is not known with extensive literature search. Peculiarity in our case is that the mucocele involved only the tip, sparing significant length of proximal appendix, both grossly and microscopically.
Mucocele of appendix is known for posing diagnostic dilemma, especially in women. Most of the cases are diagnosed at surgery. Approximately 23-50% of patients are asymptomatic, with lesions being discovered incidentally during surgery. Most of the patients can present with right lower quadrant pain, altered bowel habits, per rectal bleeding or palpable mass [3]. Our patient presented with history of vague right lower abdominal pain, on and off with a palpable mass in the right iliac region. Our clinical diagnosis was ovarian mass rather than appendicular lesion.
On ultra-sound, mucocele can be diagnosed by appearance of concentric echogenic layers within cystic mass in the right lower quadrant of abdomen in presence of normal ovary. This sign is known as ‘The Onion Skin Sign’ [4]. CT scan features showing cystic dilatation of appendix, mural calcification, and a luminal diameter greater than 1.3 cm. are suggestive of mucocele of appendix [5, 6]. It is preferred that a combination of sonographic and CT findings may aid in correct pre-operative diagnosis of mucocele of appendix [7]. In our case, ultrasound and CT findings were neither classical nor complementary, causing preoperative diagnostic dilemma.
Treatment for mucocele of appendix is always surgical. The extent of surgery depends upon factors such as:
PhysicaSize of the base,
Integrity of appendiceal wall,
Histopathological findings &
Lymph node involvement.
The treatment options are simple appendectomy,typhlectomy or right hemicolectomy with or without lymphadenectomy. Although it is technically possible to remove the intact appendix with free resection margins with laparoscopy, the advantage of open surgery is the release and exteriorization of the cecum, avoiding the contamination of the cavity in case of accidental rupture of the appendix [8].
Conclusion
Mucocele of appendix is a rare pathology. However, mucocele involving only the tip, sparing significant proximal portion of the appendix is probably not known. Majority of appendiceal mucocele cases create clinical and preoperative diagnostic dilemma. In our case this dilemma was further complicated by the peculiar situation of the mucocele.
[1]. Enrique Higa, Mucosal hyperplasia, Mucinous cystadenoma and mucinous cystadenocarcinoma of the appendix, A re-evaluation of appendiceal “Mucocele”Cancer 1973 Vol. 32:1525-41. [Google Scholar]
[2]. Ekinadoese Juliana Aghahowa, Appendicular Mucocele – A Case ReportKuwait Medical Journal Mar. 2008 40(1):78-80. [Google Scholar]
[3]. Ciprian Bartlett, Mucocele of The Appendix – A diagnostic dilemma: A case reportJournal of Medical Case Reports 2007 1:183doi: 10.1186/1752-1947-1-183 [Google Scholar]
[4]. Benjamin Caspi, The Onion Skin Sign – A specific marker of Appendiceal MucoceleJ Ultrasound Med 2004 23:117-121. [Google Scholar]
[5]. Jinxing Yu, Helical CT evaluation of acute right lower quadrant pain: Part II, Uncommon mimics of appendicitisAJR 2005 184:1143-1149. [Google Scholar]
[6]. Bennett Genevieve L, CT Diagnosis of Mucocele of the Appendix in patients with Acute AppendicitisAJR 2009 192:W103-W110. [Google Scholar]
[7]. Giampiero Francica, Giant Mucocele of Appendix – Clinical & imaging findings in 3 casesJ Ultrasound Med 2006 25:643-48. [Google Scholar]
[8]. Jandui Gomes De Abreu Filho, Mucocele of the Appendix – appendectomy or colectomyJournal of Coloproctology July/September, 2011 Vol. 31:276-84. [Google Scholar]