A Rare Case of Renal Tumour
K. Valarmathi1, A. Jamila2, S. Ravi3, Selvambigai4, Muthulatha5
1 Associate Professor, Department of Pathology, Chengalpattu Medical College, Chengalpattu, Tamilnadu–603001, India.
2 Associate Professor, Department of Pathology, Chengalpattu Medical College, Chengalpattu, Tamilnadu–603001, India.
3 Professor, Department of Pathology, Chengalpattu Medical College, Chengalpattu, Tamilnadu–603001, India.
4 Associate Professor, Department of Pathology, Chengalpattu Medical College, Chengalpattu, Tamilnadu–603001, India.
5 Professor, Department of Urology, Chengalpattu Medical College, Chengalpattu, Tamilnadu–603001, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ravi S., Professor, Department of Pathology, Chengalpattu Medical College, Chengalpattu, Tamilnadu–603001, India.
Phone: 9842866270,
E-mail: kumudharavips@gmail.com
Primary Renal Lymphoma (PRL) is an unusual and a rare tumour of the kidney. By definition, PRL is a lymphoma without evidence of any systemic involvement. This report describes a case of PRL, which included clinical presentation, imaging findings, histopathology and immunohistochemistry.
Kidney, Lymphoma, Neoplasm
Case Report
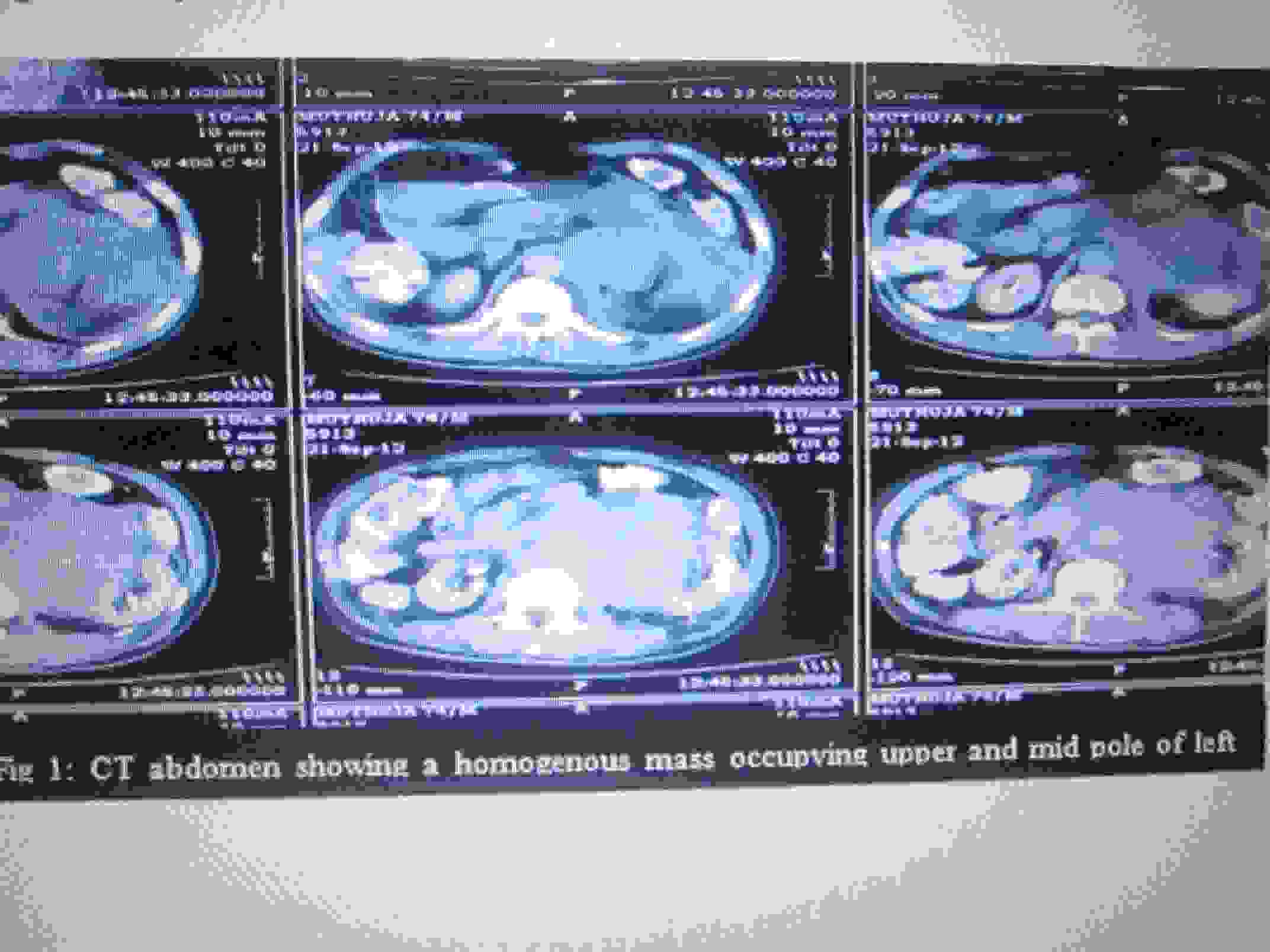
A 74-year-old male came with a complaint of left loin pain which was there since past 2 months. On examination, he was found to have a lumbar mass. An ultrasound of kidneys showed a left upper pole renal mass which measured 8 x 7cm. A plain CT of abdomen revealed a solid, homogenous, mild, enhancing mass which occupied upper and mid pole, which measured 8.5 x 7cm [Table/Fig-1]. Chest X-Ray and CT of chest, along with a complete physical examination, did not reveal any other mass or tumour. Left radical nephrectomy was done. After diagnosing PRL, patient was referred for chemotherapy and he is doing well till date.
CT Abdomen showing a homogenous mass occupying upper and mid pole of left kidney.
Pathology Findings
Left radical nephrectomy specimen measured 12 x 9 x 8cm. E/S–Capsule and perinephric pad of fat could be stripped off in some areas, which revealed an adherent tumour in the upper and mid pole. C/S showed a grey white tumour which occupied upper and middle poles and renal pelvis, [Table/Fig-2] which measured 8 x 7x 4 cm. The tumour was found to infiltrate into the ureter [Table/Fig-3]. The mass was found to involve the parenchyma.
Nephrectomy tumor mass occupying upper, mid pole and renal pelvis
Tumor involving the ureter
The microscopic examination showed that renal parenchyma and adjoining neoplasm were composed of diffuse sheets of a monotonous population of atypical lymphoid cells [Table/Fig-4], sparing the [Table/Fig-5]. Areas of necrosis and haemorrhage were found to be interspersed within the tumour cells. The cells are found to infiltrate the perinephric pad of fat and ureter [Table/Fig-6].
Higher magnification showing monotonous population of atypical lymphoid cells (H & E 40 xs)
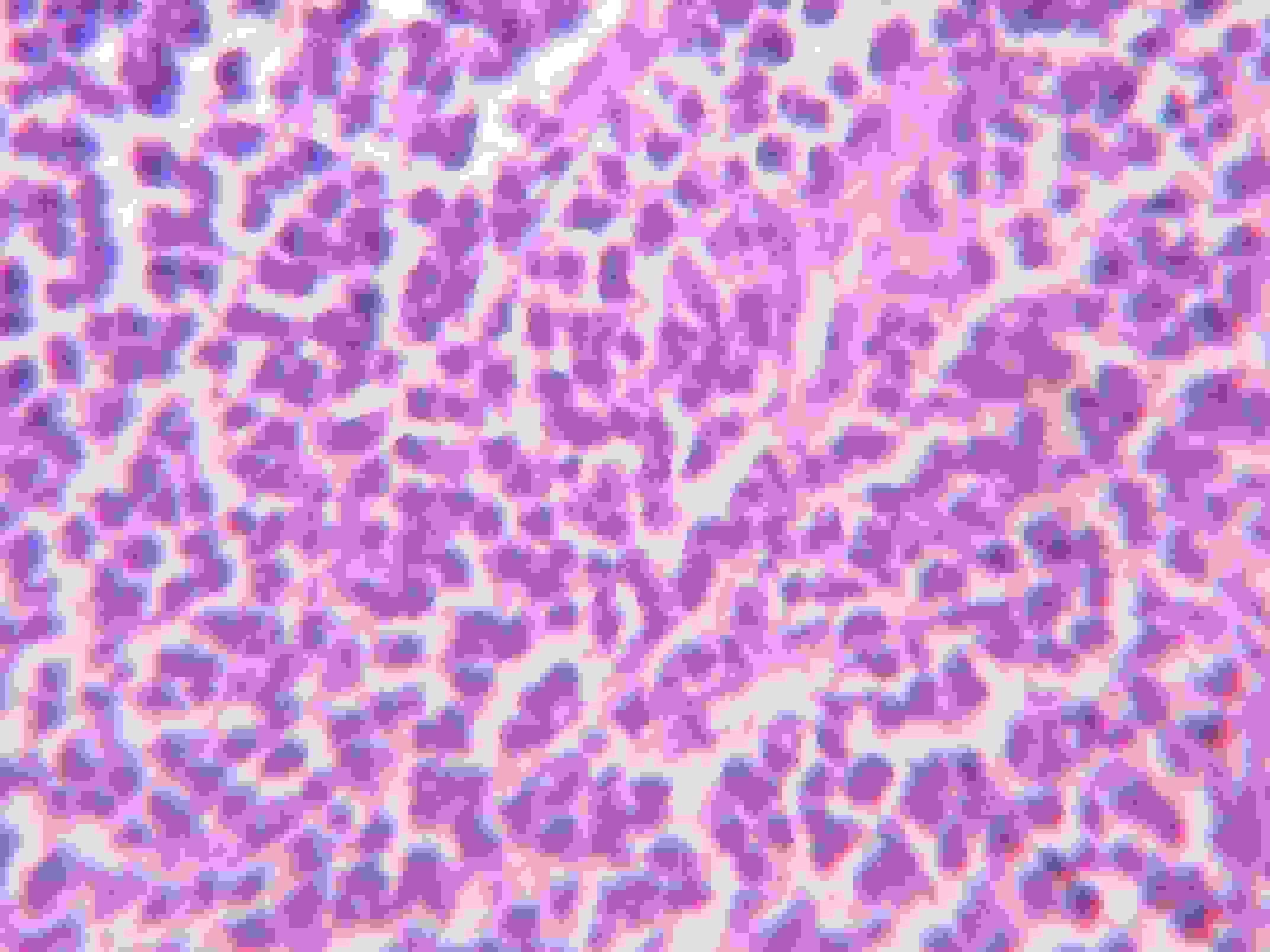
Microscopy showed renal parenchyma and adjoining renal tumor (H & E 10x)

Ureteric involvement by tumor cells (H & E 10 xs)
Based on these findings, a diagnosis of renal lymphoma was made and it proceded for immunohistochemistry. The cells revealed a diffuse positivity for CD45 [Table/Fig-7].
Immunohistochemistry shows cytoplasmic positivity for CD 45
A peripheral smear and a bone marrow examination were done, which revealed a normal picture.
Discussion
A malignant lymphoma rarely presents as a primary, extranodal renal neoplasm [1]. A primary renal lymphoma should be considered in the presence of isolated renal masses, to ensure an early chemotherapy after a histological examination. Common nonmalignant lesions such as simple cysts, angiomyolipoma, abscess, and xanthogranulomatous pyelonephritis, have characteristic radiographic findings and/or clinical history. However, it is important to include renal lymphoma in the differential diagnosis of renal masses, because generally, lumphoma is a systemic disease and treatment is nonsurgical.
Aetiology of PRL is still unknown and many classes of NHL, which include large, small, intermediate and mixed cell types, have been described. Large cell lymphoma is more common than small cell lymphoma and Hodgkin’s lymphoma. Diffuse large B-cell lymphoma (DLBCL) is the most common histology of PRL. Recent research has focused on intravascular large B-cell lymphoma (IVLBCL), which is a rare variant of DLBCL, that is characterised by a malignant lymphoid cell proliferation within the lumina of small blood vessels of several organs (i.e., central nervous system, kidneys, adrenals, skin, liver, or lungs). The presentation of IVLBCL that is limited to the kidney is rare. However, unlike the fatal prognosis of systemic IVLBCL, it was observed that patients who had kidney-limited IVLBCL had a good prognosis when they were treated with CHOP + rituximab protocols. Therefore, some authors recommend differentiating kidney-limited IVLBCL as a distinct, better-prognosis variant of systemic IVLBCL.
A primary renal lymphoma is a disputed condition, because the renal parenchyma does not contain lymphatic tissue. It has been suggested that a primary renal lymphoma may originate in the lymph nodes of the renal sinus or in the lymphatic network of the renal capsule and that it forms cords of cells that penetrate the renal parenchyma [2].
A primary renal lymphoma is USUALLY seen in adults, with an average age of 60 years and a slight male preponderance [3]. It can present in many ways. However, the most common tumours are primary tumours which present as single or multiple nodules, or that involve the kidney, either in a haematogenic dissemination form or through a contiguous retroperineal disease. A PRL is often mistaken for an RCC, and the diagnosis is made after a radical nephrectomy is done.
However, imaging studies may provide evidence for suspected cases of PRL. Ultrasonographic images typically depict an unspecific homogeneous hypoechoic mass. Therefore, a CT scan is preferred for differentiating a PRL from an RCC. A PRL usually appears as a hypervascularised mass with a minimal and a characteristic homogeneous contrast enhancement. Other indirect signs of PRL include the following: enlargement of renal size, direct infiltration of sinus or hilum by a bulky mass, or a diffuse retroperitoneal infiltration. Other less commonly seen patterns include, enlarged non enhancing kidneys, direct invasion of renal sinus and hilum by a bulky retroperitoneal mass or a diffuse perirenal infiltration which encloses the kidney. Most of the patients also have adjacent retroperitoneal adenopathy. A PRL is often mistaken for an RCC, and the diagnosis is made after a radical nephrectomy is done. In contrast, indirect signs that may indicate an RCC which includes the following: the presence of calcifications, venous thrombosis, or an obstructive mass effect over the renal vessels or urinary tract. However, a percutaneous biopsy is always required to confirm the diagnosis. 75% of patients die within 1year of their surgery.
The following diagnostic criteria must be satisfied for a diagnosis of PRL [4]:
Physical examination should exclude any extra renal primary site.
CT of abdomen and thorax must rule out extra renal disease.
A tissue diagnosis is necessary.
A peripheral blood smear must demonstrate a normal pattern.
A bone marrow trephine and an aspirate must show normal patterns [5–7].
[1]. Farrow GM, Harrison EG Jr, DC, Sarcomas and Sarcomatoid mixed malignant tumors of the kidney in adult IICancer 1968 22:551-55. [Google Scholar]
[2]. Torecilla Garcia – Ripoll Jr, Pascual Samaniogo M, Martin Blanco S, Primary renal lymphomaActus Urol.Bsp 2003 Jul – Aug 27(7):555-08. [Google Scholar]
[3]. Gellrich J, Hakenburg OW, Navmann R, Mansock A, Lossitzer Wirth MP, Primary Renal Non-Hodgkin’s lymphoma: A difficult differential diagnosisOccleologrie 2002 25:273-07. [Google Scholar]
[4]. O’Sullivan AW, Lee G, Fitzgerald E, O’Sullivan GC, Bilateral primary renal lymphomaIrish Journal of Medical Science March 2003 172(1):44-45. [Google Scholar]
[5]. Sheth S, Ali S, Fishman E, Imaging of Renal Lymphoma: Patterns of Disease with Pathologic CorrelationRadio Graphics 2006 26:1151-68. [Google Scholar]
[6]. Okuno SH, Hoyer JD, Ristow K, Witzig TE, Primary renal non-Hodgkin’s lymphoma. An unusual extranodal siteCancer 1995 75:2258-61. [Google Scholar]
[7]. Yasunaga Y, Hoshida Y, Hashimoto M, Miki T, Okuyama A, Malignant lymphoma of the kidneyJ Surg Oncol 1997 64:207-11. [Google Scholar]