Malrotation is a well described intestinal anatomical variant. The overall incidence is estimated to be occurring in 1 in 2500 to 3000 individuals. Failure to recognize the nature and characteristic features of these misplacements may lead to grave errors in procedure, or to injurious prolongation of the operation. The treatment goals are to prevent intestinal catastrophe.
Material and Methods
During routine dissection of cadavers for 1st MBBS students in the last 5 years at Sri Siddhartha Medical College, a rare case of sub hepatic caecum was observed in a male cadaver. A detailed dissection was done in the region to observe the position of appendix and their vascular supply. The specimen was photographed.
Observations and Results
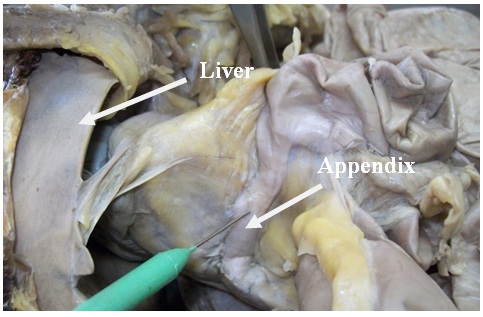
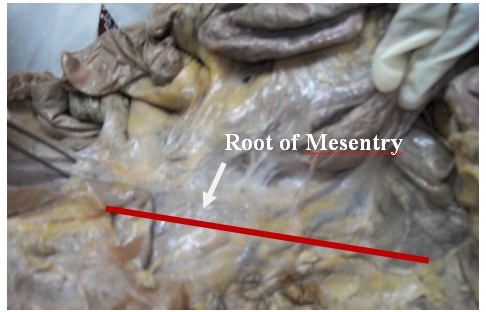
During routine dissection we found a rare developmental anomaly of positioning of caecum in sub–hepatic region with retrocecal appendix in a male cadaver. The ascending colon was absent; the ileum with its mesentry was extending till sub–hepatic region. The appendix measured about 9.5 cm [Table/Fig-1, 2]. The attachment of root of mesentry was normal in position extending from L2 to the right sacroiliac joint [Table/Fig-3]. The terminal part of ileum was extending from right iliac fossa to the sub hepatic region to reach caecum and was enclosed by the mesentry. The other structures were normal in position.
Shows the Position of Caecum

Showing the inferior Margin of Liver and Retrocaecal appendix
Showing the attachment of root of Mesentr
The superior mesenteric artery was normal in its origin and course but variation was observed in its branching pattern. On the left side the jejunal and ileal branches were normal, but on the right side, the ileocolic branch was absent. The caecum and appendix were supplied by the right branch of middle colic artery. The tip of the appendix was also supplied by an additional branch from right colic artery. The continuation of superior mesenteric artery joined the descending branch of right colic artery and supplied the mobile part of ileum on right side.
Discussion
Malrotation is a consequence of altered embryonic development of the midgut. The true incidence of intestinal rotational disorders is as high as 1% of the total population [1] and roughly 50-70% of cases occur during the first four weeks of life [2].
Midgut is the portion of intestinal tract which develops from the roof of yolk sac between the anterior and posterior intestinal portals. The development of midgut undergoes rotation and fixation of parts to assume adult position. The changes occur near the caecal region as well, which results in the so called decent of caecum or caudal migration of caecum with the relative diminution of size of right lobe of liver so that ascending colon hepatic flexure are defined, then the caecum reaches the right iliac fossa.
Derangements may occur at any stage, either rotation or fixation. The sub hepatic caecum occurs in 6% of population [3]. The common varieties are sub hepatic caecum as in this case, lumbar caecum, pelvic caecum, mobile ascending or descending colon [3]. Complete nondescent of the caecum and appendix is significant as the source of appendicitis which occasionally occurs in the upper right abdomen.
Sub–hepatic appendicitis was first described in 1955 by King, but has rarely been reported since, and includes a case of delayed diagnosis leading to perforation [4]. Strangely, literature dealing with sub–hepatic caecum, with or without appendicitis, is comparatively scarce. Lockwood, in 1892, reported one case studied at autopsy. Treves in 1885, listed two cases studied at autopsy, and later Robinson reported 2 cases in the study of 130 necropsies. Smith in 1911, reported in autopsy studies on infants, most of them were under 3 months of age, stated that nondescent of the caecum occurred in 6% of 1050 cases. Surgeons have described occasional cases discovered at operation. Jonas, reported 11 cases in which he was able to demonstrate arrest in development of the intestinal tract, described three in which the appendix was found in the gall-bladder region [5]. In cases of appendix situated at a higher position, the symptoms and signs of acute appendicitis may mimic acute cholecystitis [6] [Table/Fig-4].
Shows the No of Cases Reported by Different Authors
| Sl No | Author | No of Cases Reported |
|---|
| 1 | Lockwood | 1 |
| 2 | Treves | 2 |
| 3 | Robinson | 2 |
| 4 | Jonas | 3 |
| 5 | Present Study | 1 |
Sub–hepatic anatomical location of the appendix makes it more difficult to diagnose acute appendicitis at any age, including in older adults. Usually the patients presents with acute abdominal pain. Abdominal CT is frequently required for diagnosis. Sub– hepatic appendicitis is a rarely reported variant of a common surgical emergency that leads to delayed diagnosis and incurs higher complication rates, including suppuration and perforation [4]. Recurrent abdominal pain in otherwise healthy adults may be caused by developmental anomalies of gut. These anomalies should be kept in mind before any psychiatric cause [7]. An understanding of vascular variants is critical to perform surgeries in mal rotated patients. In this case the cecum and appendix were supplied by the right branch of middle colic artery. The tip of the appendix was also supplied by a branch from right colic artery. Failure to recognize these vascular anomalies may lead to serious complications. Other developmental anomalies of the gastrointestinal system may complicate the picture [5,6].
Sir Arthur Keith mentions that the secondary adhesions of the mesenteries of abdominal viscera are regarded as adaptations to the upright posture. An iliac position of caecum is a feature which occurs only in the animals adopted to the upright posture. In this case the attachment of root of mesentry was normal in position extending from L2 to the right sacroiliac joint. The peritoneal adhesions which are formed in the 4th and 5th months of foetal life especially the caecum assumes its position in the iliac fossa, are subject to great range of variations. The object of all these adhesions is to give a fixation of the viscera to the abdominal wall. The extensive attachment of mesentry is also a secondary adhesion affected due to upright posture [8].
Conclusion
To conclude, minor degrees of developmental misplacements of portions of the midgut are extremely common. The incidence of essential errors of disposition is confined almost entirely to midgut. The reason for this greater frequency of error in the midgut is to be found in the more complicated evolution of its natural disposition in the abdomen.
The relatively high incidence of appendicitis in the general population and its high occurrence in older adults increases the burden of appendicitis in the elderly. Rarely reported primary sub hepatic and other unusually located appendicitis may lead to diagnostic delays at any age, especially in the elderly. Hence surgeons should be aware of these types of variations to avoid unusual complications.