Management of Adnexal mass poses a double edged problem. There is a dilemma of performing extensive surgery in the form of staging laparotomy for a benign disease on one hand and the lurking fear of missing the diagnosis of malignancy on the other hand in case the patient is followed on conservative lines. Thus, it seems important to establish risk profiles of all patients with adnexal masses so they can reap the benefit of minimally invasive surgery wherever possible.
This prospective study was conducted to evaluate the benefit of laparoscopic management of adnexal masses thought to be benign based on certain demographic characteristics.
Material and Methods
This prospective study was carried out at a tertiary Hospital where 136 women with adnexal masses were enrolled into the study. The study was approved by the institutional review board.
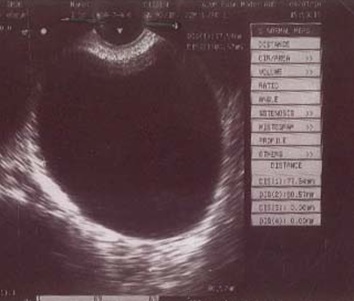
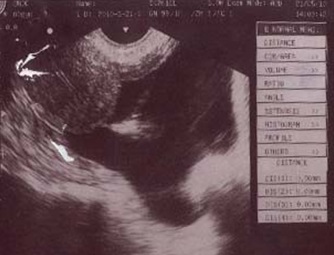
All cases of adnexal masses were enrolled into the study from January 2008 to July 2011, and then subjected to risk evaluation for any underlying malignancy. These women were subjected to thorough history taking including detailed history of pain and the onset or duration of mass. They were then subjected to Transvaginal/ transabdominal Sonography for morphological features [Table/Fig-1] like Tumour size, bilaterality, solid areas, complex echotexture with solid cystic areas or cystic, presence and thickness of septations, presence or absence of ascites [Table/Fig-2]. Tumour marker studies like CA–125, CEA, AFP, beta HCG and LDH were done in patients wherever indicated. The sensitivity and specificity of Serum CA–125 >35U/ml for identifying or ruling out malignancy is 85.5% and 86.4%, respectively, while sensitivity and specificity of cystic morphology on ultrasound for the same is 100% and 46.6%, respectively [1]. Those adnexal masses with high suspicion of malignancy were subjected to additional investigations like colour Doppler ultrasonography, CT scan or MRI.
| Diagnosis | No. of patients |
|---|
| Unilocular clear cyst | 68 |
| Endometrioma | 23 |
| Dermoid cyst | 14 |
| Chronic ectopic | 8 |
| Hydrosalpinx | 5 |
| Encysted fluid collection | 3 |
| Multiloculated cyst | 3 |
| Hemorrhagic cyst | 6 |
| Other pathologies | 6 |
Ultrasound image of a clear cyst
Based on the above criteria the following steps were taken as exclusion criteria for the laparoscopic management in this study:
Complex echotexture with solid cystic areas on transvaginal/ transabdominal ultrasonography.
Raised CA–125 levels in the absence of endometriotic cysts.
Presence of significant ascites.
Resistance Index< 0.4 on Doppler Ultrasonography suggestive of low resistance flow or increased vascularity.
The rest of the adnexal masses were then taken up for laparoscopic management and evaluation [Table/Fig-3].
| Diagnosis | No. of patients |
|---|
| Benign serous cyst | 67 |
| Endometriosis | 23 |
| Hydrosalpinx | 6 |
| Dermoid cyst | 14 |
| Chronic ectopic | 8 |
| Encysted fluid collection | 3 |
| Non–communicating horn of the uterus | 1 |
| sub serous fibroid | 1 |
| Benign mucinous cyst | 4 |
| Haemorrhagic cyst | 5 |
| Paraovarian cyst | 2 |
| Other benign pathologies | 2 |
In young patients with benign pathology cystectomy was performed, while for post–menopausal women oophorectomy or salpingo–oophorectomy was performed. Salpingectomy was performed for hydrosalpinx.
Laparoscopy was performed by using a 10 mm umbilical port through which a 0 degree telescope was inserted and two additional ports of 5mm each were made, one on the left iliac fossa, 1.5 cm medial and anterior to anterior superior iliac spine, the other on the left lumbar region in the plane of umbilicus. A thorough visualization of the entire pelvis and abdomen was done and any fluid if present was aspirated and sent for cytology. A note of the size, shape, location and nature of the adnexal mass, the opposite ovary, their surface, presence of ascites and adhesions were made. The peritoneal surfaces, sub diaphragmatic surface and the entire viscera were inspected in the clockwise direction and biopsy was taken from any suspicious area. Thereafter, bipolar coagulation of the infundibulopelvic ligament was done followed by coagulation of ovarian ligament and fallopian tube to ensure the complete resection of the pedicle.
If cystectomy was planned, capsule was stripped from the ovarian surface using two graspers for traction and counter traction. Bipolar forceps was used to coagulate the bleeding vessels at the base of capsule. After achieving haemostasis edges of the capsule they were left to heal without suturing [Table/Fig-4].
Image of laparoscopic cystectomy

All adnexal masses were placed into endobags and further decompressed if further required in the bag and then removed through one of the ports to avoid intra–peritoneal spillage of the surgical specimen and contamination of the abdominal wall during removal.
For small superficial endometriomas that were difficult to remove surgically, fluid was drained from these endometriomas followed by bipolar fulguration of cyst wall.
Cysts larger than 10cm, were first punctured by the trochar and sleeve of one of the ancillary ports, then keeping the sleeve in situ, the trochar was withdrawn and replaced by suction–aspiration cannula. The entire contents of the cyst were then aspirated carefully without spillage of its contents. After enucleation of the cyst, the cyst was held near this puncture site and brought out through one of the ports, which was enlarged if required to remove the entire cyst carefully avoiding any spillage of its contents.
In selective cases with high suspicion of malignancy per–operatively, specimen was sent for frozen section with the intent of performing a complete staging laparotomy on evidence of malignancy.
At the conclusion of each case haemostasis was assured and the laparoscopic incisions were closed.
The patients were followed up in the post-operative period for any complication. A note of the histopathology report was made and matched with the pre-operative diagnosis. The histopathology slides were reviewed in the Department of Pathology, Base Hospital, Delhi Cantt, India [Table/Fig-5].
| Diagnosis | No. of patients | Benign/Malignant |
|---|
| Serous cystadenoma | 53 | Benign |
| Endometriosis | 23 | Benign |
| Hydrosalpinx | 6 | Benign |
| Mature teratoma | 14 | Benign |
| Chronic ectopic | 8 | Benign |
| Leiomyoma uterus | 1 | Benign |
| Non-communicating horn of uterus | 1 | Benign |
| Encysted fluid collection | 3 | Benign |
| Borderline tumour of low malignant potential | 1 | Borderline malignancy |
| Mucinous cystadenocarcinoma | 1 | Malignant |
| Mucinous cystadenoma | 3 | Benign |
| Haemorrhagic cyst | 5 | Benign |
| Paraovarian cyst | 2 | Benign |
| Other benign pathologies | 15 | Benign |
Results
There were 136 patients in our study, who were treated by laparoscopy for an adnexal or pelvic mass. While most of the women in our study group were in the reproductive age group, there were girls as young as 12 years to women as old as 72 years of age [Table/Fig-6]. Out of the 136 patients, 23 women were post–menopausal. 22 women in our study group had cyst larger than 10cm with the largest cyst 28–30cm in diameter, almost reaching up to the xiphisternum.
| Age in years | Number of patients |
|---|
| <20 | 5 |
| 21-30 | 54 |
| 31-40 | 38 |
| 41-50 | 26 |
| 51-60 | 6 |
| >=61 | 7 |
| Mean age | 35.85 |
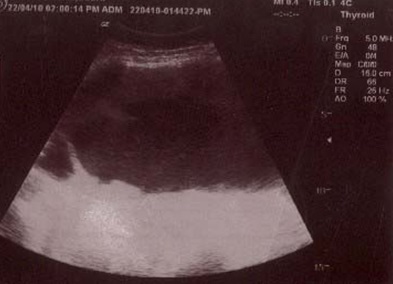
Among all the patients, two were treated laparoscopically. One patient had to be taken up for a staging laparotomy later on, in view of malignancy confirmed on histopathology report. Another patient with chronic pelvic pain and adnexal mass was detected to have encysted fluid collection with extensive intra-peritoneal adhesions [Table/Fig-7].
Ultrasound image of encysted fluid collection
83 patients (61.03%) had undergone laparoscopic cystectomy, while 18(13.24%) patients each had undergone laparoscopic oophorectomy and salpingo-oophorectomy, and 12 patients (8.82 %) underwent laparoscopic salpingectomy. 3 patients underwent laparoscopic adhesiolysis in view of the encysted fluid collection. Adhesiolysis was also performed as an adjunct to several of the above procedures in view of endometriosis or adhesions due to previous surgeries.
A 32–year–old para 3 lady with progressively severe dysmenorrhea who was pre–operatively suspected to have endometriosis was discovered to have a non–communicating horn of uterus on laparoscopy. Laparoscopic resection of non–communicating horn was performed for the patient. The histopathology report confirmed benign pathology in 134 patients (98.53%), while borderline Tumour of low malignant potential was reported in one (0.74 %) and mucinous cystadenocarcinoma in one patient (0.74%) [Table/Fig-5].
The histopathology report of a 14–years–old girl with a clear unilocular cyst size 15 x15cm with no evidence of ascites, revealed a diagnosis of borderline Tumour of Low Malignant Potential (LMP). Since she was at Stage 1a she was on close follow up till date, with no evidence of metastasis or tumour spread post–operatively till date.
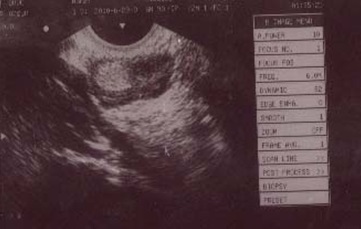
A–52–year old postmenopausal lady with a clear unilocular cyst of size 8 x 9 cm [Table/Fig-8] showed a focus of mucinous cystadenocarcinoma on final histopathology report. She was taken up for a staging laparotomy with total abdominal hysterectomy and bilateral salpingo–oophorectomy on post–operative day 8 and was found to be stage 1a ovarian cancer with no evidence of tumour spread. She was on follow up till date, with no evidence of metastasis.
Ultrasound image of a unilocular clear ovarian cyst which was confirmed as malignancy on histopathology report
Discussion
The aim of this study was to assess the feasability of laparoscopic management of adnexal masses that were predicted to be benign.
The authors have used a combination of clinical impression, ultrasonographic tumour morphology and serum CA–125 value <= 35U/ml to differentiate women at risk of ovarian cancer from those with benign adnexal mass [Table/Fig-9]. Doppler ultrasound, CT scan and MRI have been used selectively only in those cases with high suspicion of malignancy. This combined criteria accurately predicted benign masses in most women (97.79%) except for three. Using a similar criteria, a chinese study [2] has reported a rate of malignancy of 0.77% while Duggal et al., [3] reported no malignancy in the 121 patients evaluated in their study.
Sensitivity and specificity of each variable for identifying or ruling out malignancy [1]
| Sensitivity (%) | Specificity (%) |
|---|
| Serum CA125 >35U/ml | 85.5 | 86.4 |
| Tumour morphology: |
| Cystic | 100 | 46.6 |
| Complex | 91.6 | 56.1 |
Jeong–Won Lee et al., [4] using Sasson’s scoring system for trans-vaginal ultrasound and serum CA–125 levels >= 65U/ml accurately predicted benign adnexal masses in most post–menopausal women (99.5%).
Laparoscopy was successfully completed in 134/136 patients (98.53%) without the need to proceed to laparotomy.
One case was converted to the laparotomy at surgeon’s discretion in view of technical difficulties encountered due to dense adhesions.
Another patient underwent staging laparotomy 8 days after laparoscopic oophorectomy as the cyst was confirmed to be mucinous cystadenocarcinoma on final histopathology report.
In our study, there were two cases of unsuspected malignancy, one was borderline tumour of Low Malignant Potential (LMP), and the other was mucinous cystadenocarcinoma, both were staged on 1a. In both the cases, there was no spillage of contents and no evidence of spread of malignancy.
There was a concern that for stage 1a ovarian cancer, accidental rupture of tumour capsule during laparoscopic surgery may lead to intra–peritoneal dissemination of malignant cells and hence worsen the prognosis.
Studies have shown that intra–operative rupture of capsule upstages the disease from 1a to 1c, and therefore necessitates the use of adjuvant chemotherapy for the patients who may not have required it otherwise. However, this does not affect the prognosis [2,5,6].
On searching the literature it was not mentioned of the possible dissemination of cells in borderline Tumours [7].
Another concern is the spread of malignancy due to delay in the definitive surgery i.e., staging laparotomy in cases where malignancy is revealed by final histopathology report. Literature shows Tumour propagation by performing a biopsy in FIGO stage Ia ovarian cancer patients does not occur if the patient receives adequate radical surgical treatment within one week [8]. However, delays of more than 4 weeks from the time of initial diagnosis to the complete surgical staging for incidentally discovered ovarian cancer does have an adverse impact [9].
Another point of debate is the removal of dermoid cyst [Table/Fig-10] laparoscopically, as there are concerns for post–operative infection and chemical peritonitis in the event of accidental rupture of the capsule.
Ultrasound image of dermoid cyst
In our study, 14 dermoid cysts were successfully removed laparoscopically. We had taken meticulous care to avoid spillage of the contents of the cyst. The intact cyst was placed in the endobag and decompressed inside the bag before removal of its contents. We had 4 cases of intra–peritoneal spillage of contents from the dermoid cyst, they were managed by copiously irrigating with 5 litres of saline. There was no evidence of chemical peritonitis in the post–operative period
It has been shown that in the event of accidental rupture of the capsule, irrigation with copious saline reduces post-operative chemical peritonitis to less than 1% [10,11]. Also, reverse trendelenberg position is important at the end of the procedure to optimize the results of the lavage [7].
Hence, laparoscopy is the method of choice for the removal of benign dermoid cysts as it offers the advantages of reduced pain, shorter hospital stay, better cosmetic outcome and fewer adhesions [7].
In this study there were no trocar injuries and no bowel, vessel or bladder injury during surgery. One patient had post–operative paralytic-ileus, which responded to conservative management. The complication rates observed in this prospective study are comparable to those previously published [Table/Fig-11].
Comparison of complications of different studies
| Study | No. of cases | Laparotomy due to malignancy | Laparotomy due to technical reasons | Trocar site injury | Bowel/bladder injury | Intra–op. complications– others | Post–op. complications |
|---|
| Jeong-Won Lee et al., (2005) | 219 | 1 (0.46%) | 5 (2.28%) | 2 (0.91%) | 0 | 0 | 4 (1.83%)–superficial abdominal hematoma |
| Duggal et al., (2004) | 121 | 0 | 1 (0.83%) | 0 | 0 | 1 (0.83%) | 0 |
| Leng Jui-hua et al., (2006) | 2083 | 16 (0.77%) | 0 | 0 | 0 | 0 | 0 |
| Surender Mohan et al., (2011) | 136 | 1 (0.74%) | 1 (0.74%) | 0 | 0 | 0 | 1 (0.74%)–paralytic ileus |
Conclusion
Hence, in judiciously selected cases and in expert hands benefits of laparoscopic surgery can be offered to patients for management of adnexal masses without compromising on the quality of the treatment.