The amputation of one or more fingers of the hand may result as a consequence of a trauma, disease or a congenital abnormality which causes functional deficiencies and social dysfunction for the patient. The amount of tissue remaining, condition of the bone and the number of fingers involved have to be considered when choosing suitable treatment option [1]. Several microsurgical techniques such as toe-foot-transfer, lengthening procedure and the use of osteo-cutaneous flap may offer opportunities to reconstruct the lost or missing phalanges [2]. The use of bone-anchored implant retained silicone finger prosthesis represents an alternative technique. Bone anchoring method is used since 1994 as described by Branemark [3].
The retention is the key factor for the success of finger prosthesis. The finger prosthesis requires an optimum retention for functions such as grasping, carrying and holding [4]. The friction or adhesive-retained finger prosthesis cannot provide enough retention. So, using implant offers better retention for the finger prosthesis which helps in different functions. The surgery for implant placement has initially been described as a two stage surgery technique and is considered as the standard protocol. Indeed, the first step is the placement of a titanium fixture in the finger bone which remained covered for 2–4 months of healing to permit osseointegration. An abutment is then fitted accordingly in the second stage. The low rate of implant loss or other complications yielded by the two stage surgery technique has led to believe that this technique might be feasible [1–3]. However, no study in the literature has attempted to compare this technique with two stage surgery technique and stated a clear superiority technique in the implant retained finger prosthesis. Therefore, we aim to compare one-stage and two-stage surgery in two cases, and evaluate the safety and possible superiority of the one-stage over the two-stage implant placement technique in the implant retained finger prosthesis.
Methods
Both the cases below were treated in Maxillofacial Prosthetic Clinic, Golden Jubilee Medical center, Mahidol University for the rehabilitation of finger.
Case Report 1
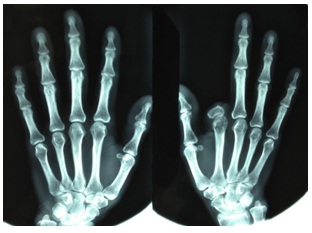
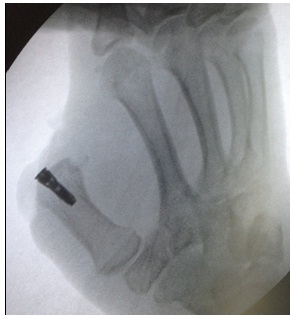
A 45-year-old female whose second (index) finger of right hand was lost as a result of accident [Table/Fig-1]. Physical examination of the hand showed that the patient’s index finger was amputated at the level of proximal phalange but the joint was preserved and functional. The proximal phalange was insufficient for the finger prosthesis using friction or adhesive. She gave no other relevant medical history. Her primary concern was esthetic problem especially at the social gatherings. Radiologic tests were performed in lateral and palmar projections to evaluate the skeleton’s bone thickness and dimensions [Table/Fig-2].
Preoperative picture of the patient with lost index finger

Radiologic examination was performed with palmar projections
The implant retained finger prosthesis was chosen by using one stage surgery technique. Then, Right Branchial nerve was anaesthetized and hemostasis was obtained using the tourniquet at 250 mmHg.
Skin incision was given at the implant site; and the remnant of the proximal phalange was removed. The position and the angulation of the implant were guided by the fluoroscopy radiation. Then implant of 5 mm diameter X 17mm length (Osseo Speed, Astra Tech, Molndal, Sweden) was placed in the bone inside the medullary canal with the insertion torque with 40 Ncm [Table/Fig-3]. Radiograph was taken to verify the position of the implant [Table/Fig-4].
Fixture was placed in the metacarpal

Radiograph was taken to verify the position of the implant

The initial stability was noted 65 Implant Stability Quotient (ISQ) using Resonance Frequency Analysis (RFA). The bone density was observed as Type IV according to Lekholm and Zarb classification [5]. Then, the skin flap was repositioned using Nylon sutures to cover the fixture. Then the skin over the implant site was punched and abutment was placed with 20 Ncm and on 10th day, the suture was removed and no infection was noted [Table/Fig-5].
Healing of soft tissue around abutment at 10 days follow up

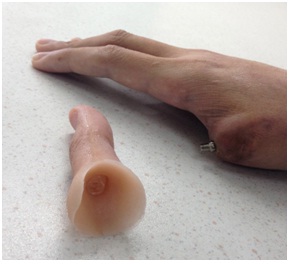
On the following 8th weeks, the implant stability was noted 72 ISQ by RFA. Then, the silicone finger prosthesis was fabricated and attached with the plastic attachment and delivered to the patient [Table/Fig-6–7].
Final silicone finger prosthesis (Dorsal view)

Final silicone finger prosthesis (Ventral view)

At 6th month follow-up, the implant showed an optimal degree of osseous integration of the implant and the absence of infection and other complications [Table/Fig-8].
The implant at 6 month follow up showing no bone loss

Case Report 2
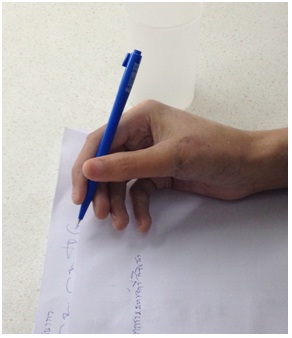
A 25-year-old male patient had an esthetic problem after the amputation of the thumb of right hand as a result of accident [Table/Fig-9]. Consequently, even being right handed, he was educated to the use of the left hand for function. Physical examination of the hand showed that the patient’s thumb was amputated at the Level of metacarpophalangeal joint [Table/Fig-9]. He also gave no other relevant medical history. On radiologic tests in lateral and palmar projections revealed only metacarpal was present [Table/Fig-10]. After consultation, the patient decided to choose implant retained finger prosthesis. In this case, we plan standard modality using two-stage technique. The similar implant of 5 mm diameter X 17 mm length (Osseospeed, Astra Tech, Molndol, Sweden) was placed in the bone inside the medullary canal with similar surgical procedures and radiograph taken [Table/Fig-11, 12]. The implant stability was noted 63 ISQ. After the skin flap closure, the patient was instructed to care the wound every 3 days with pressure dressing. On 10th day, no infection or other complications were noted and the sutures were removed. On the following 8th week, second surgery was done under local anesthesia. Incision was made on the previous incision line. The connective tissues at the osteotomy site were incised and the skin over the implant was punched. The implant stability was noted 71 ISQ. Then, the abutment was placed over the implant on the thumb [Table/Fig-13]. The patient was instructed to continue the wound care. Then, silicone finger was fabricated semi-flexed position by same procedure as in case 1 and delivered [Table/Fig-14]. The patient can write with the prosthesis [Table/Fig-15].
Preoperative picture of the patient with lost right thumb

Radiologic examination showed loss of phalanges of the right thumb

The flap was opened after the incision and the fixture was placed in the metacarpal of the thumb

The radiograph was taken to verify the position of the implant
Skin around the abutment at after the healing

Silicone thumb prosthesis
Silicone thumb prosthesis during writing
At 5th month follow-up, it showed the absence of infection and other complications.
Discussion
Finger reconstruction of proximal phalange and metacarpal requires complex surgical procedures. Digital transposition or toe-foot-transfer may able to achieve the best functional recovery of the missing finger in spite of doubtful cosmetic results; usually of compromised shape and size with unpleasant result [6]. In these two cases, we gave them both options; surgical and prosthetic reconstruction of the finger by explaining its advantages and disadvantages. But both the patients did not choose surgical reconstruction. Once rejected the possibility of surgical reconstructive techniques, we focused toward the least invasive technique which could solve the aesthetic need of the patient: osseointegrated implant is, without any doubt, a valid alternative to reconstruct the missing finger. An implant placed in the intramedullary canal of the residual bone of the amputated digit offers additional advantages, because the technique enables short stumps, where a traditional prosthesis is not successful as in Case 1 [7,8].
The implant retained finger prosthesis allows a partial recovery of the tactile sensation (osseoperception) by transferring stimuli to the bone thorough implant because of the direct pressure of the implant on the bone. Rydevik et al., [9] proposed that this occurs as a result of the transfer of tactile stimuli to inter-osseous nerves via the osseointegrated implant. The patient are able to perform majority of the daily manual activities: writing on paper with pen [Table/Fig-15], typing on the computer, holding or grabbing objects like cups, etc. Sierakowski et al., [10], patients scored highly in the Jebsen Hand Function Test, with results close to the contra-lateral hand. Despite all these advantages and gains, the total experience with osseointegrated prostheses for amputated digits is still very limited. Implant retained finger prosthesis presents minimal risk of infection and implants, complications by optimal hygiene of the wounds.
The major complications are: Lack of osseous integration of the implant which is very rare, detachment of the prosthesis or lack of acceptance by the patient. In our two cases, no major complications were seen on recall visits. The surgical and prosthetic protocol (one-stage and two-stage) for the implant placement in finger are modified from an intra-oral implant protocol [6]. The number of stage in implant placement depends on primary stability of the implant and the status of the surrounding soft tissue.
Regarding one-stage and two stage surgery technique, the latter one has more predictable outcome. The two-stage technique has low risk of infection with better soft tissue management. Moreover, it is more preferable in case of compromised initial implant stability with less than 10 Ncm of insertion torque. However, two-stage surgery demands multiple surgical procedures, hospitalisation and delayed prosthesis delivery. One stage surgery technique needs only one operation with no risk of marginal bone loss. It reduces total cost of surgery and wound care. Importantly, it improves patient’s psychology as prosthesis can be delivered earlier than Two-stage surgery technique. Even though we did one-stage case 1 and two-stage in case 2, there were no complications at follow up visits of 6th month and 5th month respectively. Furthermore, more accurate long term studies reporting on treatment protocols for separate clinical situations are required to allow meaningful comparisons.
So far, the two patients use their prosthesis during his day-to-day work and social activities without any problems and they are happy with the prosthesis.
Conclusion
One stage surgery technique for implant retained finger prosthesis is a reliable, safe and efficient option that allows a good result in a significantly lower operating time and hospital visit as compared to the Two-stage surgery technique. It is achieved in a one day surgery avoiding another hospital visit and anxiety. It could therefore be considered as good option for implant retained finger prosthesis.