Background: Physical inactivity is now a global non-communicable disease. Current recommendations from American College of Sports Medicine, American Heart Association and UK medical officers for physical activity are difficult to implement, due to time constraints and hence, they have less compliance.
Purpose: To compare Sprint Interval Training (SIT) and traditional aerobic exercise (AE) with respect to changes in Vital capacity (VC), Maximum Voluntary Ventilation (MVV) and Physical Fitness Index (PFI) in young sedentary males.
Study Design: This was a randomised, controlled trial.
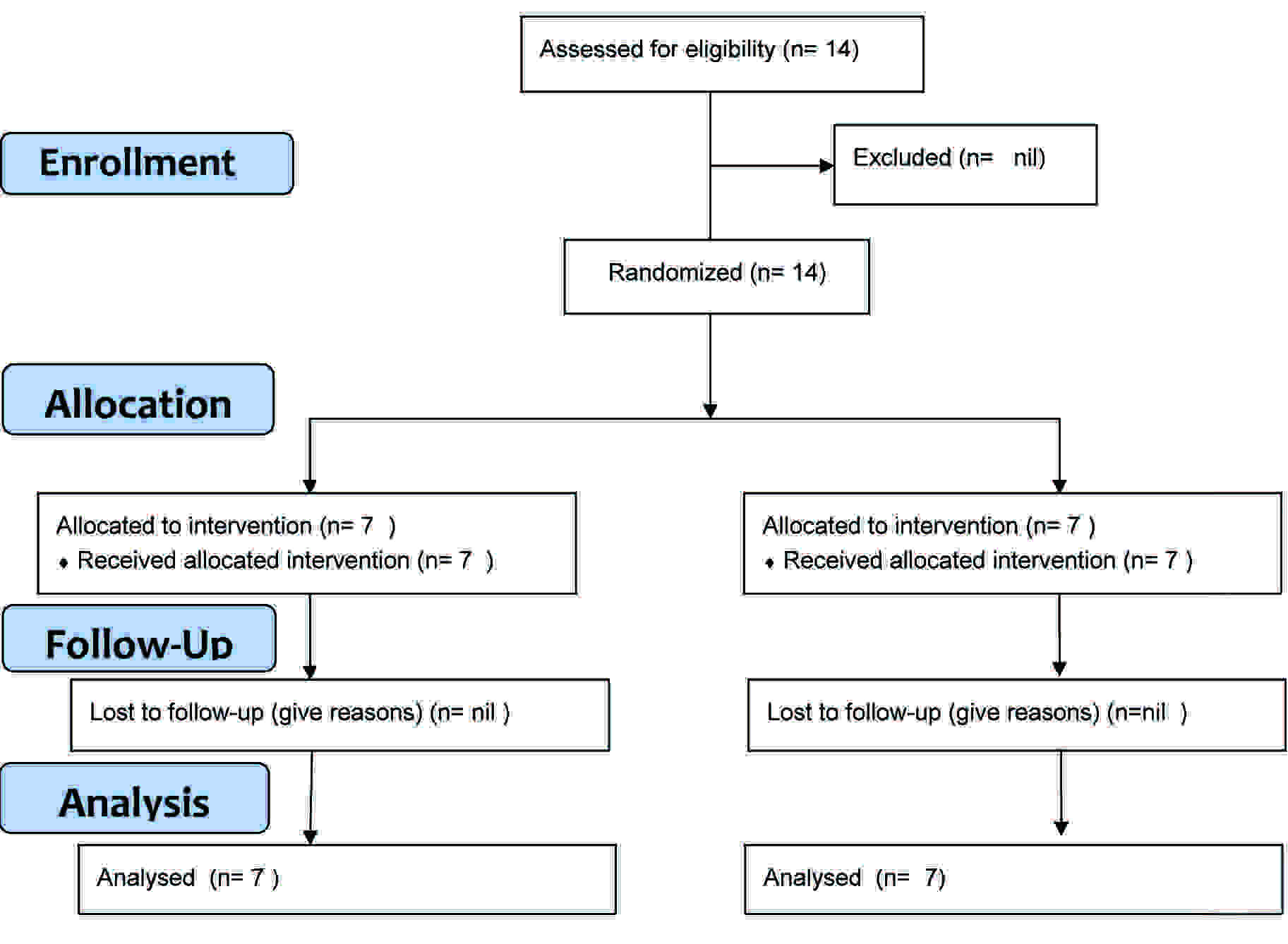
Methods: Fourteen young, sedentary, healthy males who were aged 18-25 years were randomly allocated to SIT group and AE group for 3 weeks. SIT group exercised at high intensity for 10 minutes a day, three days a week. AE group exercised at moderate intensity for 30 minutes a day, five days a week.
Results: Improvement in FVC (litres) in AE group was 0.31 ± 0.11 and that in SIT group was 0.48 ± 0.17. The improvement in MVV (litres) in AE Group was 21.5 ± 11.6 and that in SIT group was 27.77 ± 7.03. Thus, SIT showed a better improvement in primary outcome i.e. FVC and MVV, although difference in improvement was statistically not significant (p= 0.09 and 0.29 respectively). Secondary outcome i.e. PFI improved by 5.57 ± 1.71% in AE group and by 10.28 ± 3.03% in SIT group. The difference in improvement was statistically significant (p= 0.003).
Conclusions: SIT can be suggested as a time efficient option for improving cardiorespiratory fitness and hence, it can be used as a health promotion strategy.
Introduction
Physical inactivity, along with a sedentary lifestyle, is now a global ‘non-communicable’ disease [1–3]. WHO has predicted lifestyle-related chronic diseases – mainly cardiovascular disease, diabetes, cancer and chronic respiratory disease – will account for two thirds of all the deaths globally in next 25 years [4].
Economic losses as per WHO estimate between 2005 and 2015 will increase to around US$558 billion in China, $237 billion in India, $303 billion in Russia and $33 billion in the U.K [5].
Physical activity has numerous positive effects on health and regular moderate intensity exercise is known to reduce morbidity and mortality which results from chronic diseases like diabetes, cardiovascular and respiratory disorders [6–9].
Current recommendations of American College of Sports Medicine, American Heart Association and UK medical officers are 30 minutes of moderate-intensity, daily physical activity, five days a week [10–11].
However, for exercise guidelines to yield a positive economic benefit for society and health benefits for the individual, not only should the regime reliably modify key disease risk factors, it must also be plausible to implement.
In recent times, due to factors like lack of time, high penetration of television and internet and long travelling hours for job and other reasons, people find it difficult to incorporate exercise regimes which require several hours per week. Also, such regimens require a higher degree of motivation for compliance.
Sprint interval training (SIT) is an exercise strategy that is intended to improve performance and health with short training sessions. Sprint interval training protocol consists of repeated intervals of short durations at maximal or near maximal intensity, which are interspersed with recovery periods of rest or low intensity exercise. Sprint interval training has been shown to improve aerobic as well as anaerobic fitness in untrained individuals, leading to improved cardiorespiratory health [12, 13].
A recent systematic review which was made by Kent [14] has stressed the need to compare the interventions in practical scenario and it has also suggested that future research be undertaken with proper randomization and on a sample from general population unlike earlier studies which had selected samples of convenience.
The present study was undertaken to compare the traditional aerobic exercise versus sprint interval training with respect to pulmonary function tests and physical fitness index in young, sedentary males.
Methods
Trial Design and Randomisation
The present study had an Interventional parallel assignment Randomized Controlled Trial design. Allocation in 1:1 ratio to the groups and the baseline and post intervention tests were done by the trained staff that were not aware of study hypothesis. Statisticians were blinded regarding the study protocol.
Study was conducted at Government Medical College, Aurangabad, Maharastra, India, during Dec 2011 to Jan 2012.
The Institutional Ethics Committee of Government Medical College, Aurangabad, approved the study protocol.
The trial was registered with the WHO, with UTN as U1111-1126-7019 and Clinical Trial Registry of India as CTRI/2011/12/002312.
Sample size: Six per group as per Janet D Elashoff (2007) nQuery Advisor Version 7.0. Statistical Solutions, Cork, Ireland, with a single tailed hypothesis, α at 0.05 and 80% power of the study. This was calculated to estimate an effect size of 2 for the primary outcome measure.
Seven subjects per group were enrolled to allow for loss to follow up[Table/Fig-1].
Participants
Inclusion criteria
Young, sedentary, healthy males who gave their consents for the study.
Age group of 18 to 25 years.
Asymptomatic males with normal baseline ECGs.
Exclusion criteria
Those who did not give their consents for the study.
Smokers.
Any history of cardiac, respiratory, hepatic renal or any major disease.
Sportspersons or those who undertook doing athletic activities.
Fourteen subjects were recruited by advertisement from general population in the Aurangabad district Maharashtra, India. Recruitment was done during December 2011. All subjects provided written informed consents at the start of the trial.
Their baseline assessment for age, weight and height was done as per standard protocol and then random allocation was done by a computerised method to either of the groups, to undergo interventions for a period of 3 weeks. Prior to interventions, detailed histories were taken and physical examinations were done, to rule out any contraindication for high intensity exercise.
Intervention
Group I: AE: Subjects ran at low intensity ie. like jogging for 30 minutes a day for 5 days a week.
Group II: SIT: A 60 seconds intense running exercise, followed by 90 seconds of rest, which was repeated for 4 cycles, thrice per week i.e. every Monday, Wednesday and Friday.
Both groups were initially familiarised to the training protocol. The supervision of the intervention was done by trained medical staff that were not aware of the study hypothesis.
Subjects were asked to continue with their routine lifestyles and diet throughout the duration of the study.
Hypothesis: Sprint interval training is better than traditional aerobic exercise with respect to improvement in Forced Vital Capacity (FVC) and Maximum Voluntary Ventilation (MVV) after 3 weeks [Table/Fig-2].
| Parameter | AE | SIT |
|---|
| Age (years) | 22.28 ± 1.7 | 22 ± 1.63 |
| Weight (kg) | 62.1 ± 3.2 | 63.28 ± 2.92 |
| Height (cm) | 174.14 ± 2.6 | 173.85 ± 3.76 |
| BMI (kg/m2) | 20.5 ± 1.53 | 20.95 ± 0.98 |
Outcomes
Following parameters were measured as primary outcome by using Medgraphics U.S.A Body Plethysmograph, Elite Dx Model No-830001-005:
Forced Vital Capacity (FVC)
Maximum Voluntary Ventilation (MVV).
Three readings were recorded and best efforts which were made were included in the observations. All the readings were taken as per guidelines and during morning time, to maintain uniformity [Table/Fig-3].
Primary Outcome Measures CI: 95% Confidence Interval
| Parameter | AE | p value | SIT | p value |
|---|
| Before | After | Before | After |
|---|
| FVC | 3.37±0.26 | 3.68±0.26 | 0.001 | 3.36±0.33 | 3.83±0.34 | 0.001 |
| MVV | 151.16 ± 17.75 | 172.66 ± 15.48 | 0.006 | 140.66 ± 15.97 | 168.33 ±14.26 | 0.0002 |
| Change in FVC | 0.31±0.11 (CI: 0.2 to 0.41) | 0.48±0.17 (CI: 0.32 to 0.64) | 0.09 |
| Change in MVV | 21.5±11.6 (CI: 10.8 to 32.2) | 27.77±7.03 (CI: 21.3 to 34.3) | 0.29 |
Recordings were done one day prior to beginning of intervention and two days after the completion of three weeks of intervention.
Physical Fitness Index (PFI) done by Queens College Step Test [15] was measured as a secondary outcome at the beginning of study and after 3 weeks of intervention [Table/Fig-4].
Secondary Outcome Measures
| Parameter | Aerobic Exercise | p value | Sprint Interval Training | p value |
|---|
| Before | After | Before | After |
|---|
| Physical Fitness Index | 67.85±3.02 | 73.42±3.04 | 0.0001 | 67±4 | 77.28 ± 2.56 | 0.0001 |
| Change in Physical Fitness Index | 5.57 ± 1.71 | 10.28 ± 3.03 | 0.003 |
PFI = 130.907 – 1.503 × Queens College Test Heart rate.
Recordings were done one day prior to beginning of intervention and two days after the completion of three weeks of intervention.
All subjects completed the protocol. No one was lost to follow up.
Statistical Analysis
The continuous data was expressed as Mean ± Standard deviation.
Paired t–test was used to compare Forced Vital Capacity, Maximum Voluntary Ventilation and Physical Fitness Index before and after intervention in both groups. Independent t–test was used to compare changes in Forced Vital Capacity, Maximum Voluntary Ventilation and Physical Fitness Index after aerobic exercise and Sprint interval training. The calculations were done by using Microsoft Excel, 2007 version.
Results and Discussion
Sprint Interval training group showed better improvement in Forced Vital Capacity and Maximum Voluntary Ventilation, although difference in improvement was statistically not significant, but considering that time requirement was 30 minutes as compared to 150 minutes in a week for traditional aerobic exercise, it seemed to be a smarter option. Also, there was better improvement in Physical Fitness Index after Sprint Interval Training as compared to traditional aerobic exercise, the difference in improvement was statistically significant.
In accordance with our study, recently, the data from study of Dunham C, Harms CA [16] suggested that both whole-body exercise training and High Intensity Training were effective in increasing inspiratory muscle strength, with High Intensity Training offering a time-efficient alternative to Endurance Training in improving aerobic capacity and performance.
Hutchinson predicted that premature morbidity and mortality could be identified by a ‘reduced vital capacity’, a term which he coined, because he recognized that spirometric abnormalities accurately predicted about the capacity for living [17].
The results of the Prospective study with a 29 –year follow up i.e. Buffalo Health Study cohort [18], suggested that pulmonary function was a long-term predictor for overall survival rates in both genders and that it could be used as a tool for general health assessment.
Lee HM et al., [19] concluded that evaluation of lung function may be useful for improving risk stratification in persons with an intermediate CHD risk, where it added to prediction of mortality over global risk assessment.
Study of Burney and Hooper stressed that survival in asymptomatic adults without chronic respiratory diseases or persistent respiratory symptoms was associated with Forced Vital Capacity and not with airway obstruction, as was measured by the FEV1/FVC ratio [20].
Duck Chal et al., studied that maintainence or improvement of fitness was associated with a lower risk of all-cause and Cardiovascular Disease mortality in men. Preventing age-associated fitness loss was important for longevity, regardless of Body Mass Index change [21].
A recent study which was done by Abdullah Gari [22] showed that high intensity training was better than moderate intensity exercise for glycaemic control.
Thus, as was found in the present study, Sprint Interval Training can improve lung functions and Physical Fitness Index. Both these outcomes had been earlier proven to be beneficial in maintenance of health and that they were also related to longevity. In other studies, this particular training protocol was also found to improve lipid profile, glycaemic index and other risk factors for chronic diseases.
Limitation of this study was small sample size and also, further research with interventions in practical scenario in diverse populations, will be needed, to prove beyond doubt, the effectiveness of Sprint Interval Training and to incorporate it in recommendations for health promotion.
To conclude, Sprint Interval Training can be seen as a promising health promotion strategy to counteract the recent global sufferings which are caused by non communicable diseases.
[1]. World Health Organization. Preventing Chronic Diseases: A Vital Investment – WHO Global Report. 2005. http://www.who.int/chp/chronic_disease_report/contents/en/index.html (accessed 17 June 2011) [Google Scholar]
[2]. Dans A, Ng N, Varghese C, The rise of chronic non-communicable diseases in southeast Asia: time for actionLancet 2011 377:680-09. [Google Scholar]
[3]. United Nations. The Millenium Development Goals Report 2009. 2009. http://www.un.org/millenniumgoals/pdf/MDG_Report_2009_ENG.pdf (accessed 17 June 2011) [Google Scholar]
[4]. Mathers CD, Loncar D, Projections of global mortality and burden of disease from 2002 to 2030PLoS Med 2006 3:e442 [Google Scholar]
[5]. World Health Organization. The Global Burden of Disease: 2004 Update. 2008. http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004 update_full.pdf (accessed 17 June 2011) [Google Scholar]
[6]. Helmrich SP, Ragland DR, Leung RW, Physical activity and reduced occurrence of non-insulin-dependent diabetes mellitusN Engl J Med 1991 325:147-52. [Google Scholar]
[7]. Hooi JD, Kester AD, Stoffers HE, Incidence of and risk factors for asymptomatic peripheral arterial occlusive disease: a longitudinal studyAm J Epidemiol 2001 153:666-72. [Google Scholar]
[8]. Morris JN, Clayton DG, Everitt MG, Exercise in leisure time: coronary attack and death ratesBr Heart J 1990 63:325-34. [Google Scholar]
[9]. Rasmussen F, Lambrechtsen J, Siersted HC, Low physical fitness in childhood is associated with the development of asthma in young adulthood: the Odense schoolchild studyEur Respir J 2000 16:866-70. [Google Scholar]
[10]. Chief medical officers of England, Scotland, Wales and Northern Island. Start active, stay active: a report on physical activity from the four home countries’ chief medical officers. Department of Health, 2011 [Google Scholar]
[11]. ACSM, AHA support federal physical activity guidelines. http://www.acsm.org/about-acsm/media-room/acsm-in-the-news/2011/08/01/acsm-aha-support-federal-physical-activity-guidelines (accessed 17 Jan 2012) [Google Scholar]
[12]. Gibala MJ, McGee SL, Metabolic adaptations to short-term high-intensity interval training: a little pain for a lot of gain?Exerc Sport Sci Rev 2008 Apr 36(2):58-63. [Google Scholar]
[13]. Edge J, Bishop D, Goodman C, Dawson B, Effects of high- and moderate-intensity training on metabolism and repeated sprintsMed Sci Sports Exerc 2005 Nov 37(11):1975-82. [Google Scholar]
[14]. Kent W, The Effects of Sprint Interval Training on Aerobic Fitness: A Systematic ReviewWebmed Central Sports Medicine 2012 3(5):WMC003284 [Google Scholar]
[15]. Bandyopadhyay Amit, Queens College Step Test – an Alternative of Harvard Step Test in Young Indian MenInternational Journal of Applied Sports Sciences 2007 19(2):1-6. [Google Scholar]
[16]. Dunham C, Harms CA, Effects of high-intensity interval training on pulmonary functionEur J Appl Physiol 2012 Aug 112(8):3061-8.Epub 2011 Dec 23 [Google Scholar]
[17]. Hutchinson John, On the capacity of the lungs, and on the respiratory functions, with a view of establishing a precise and easy method of detecting disease by the spirometerMed Chir Trans 1846 29:137-252. [Google Scholar]
[18]. Schünemann HJ, Dorn J, Grant BJ, Winkelstein W Jr, Trevisan M, Pulmonary function is a long-term predictor of mortality in the general population: 29-year follow-up of the Buffalo Health StudyChest 2000 Sep 118(3):656-64. [Google Scholar]
[19]. Lee HM, Le H, Lee BT, Lopez VA, Wong ND, Forced vital capacity paired with Framingham Risk Score for prediction of all-cause mortalityEur Respir J 2010 Nov 36(5):1002-6.Epub 2010 Jun 18 [Google Scholar]
[20]. Burney PG, Hooper R, Forced vital capacity, airway obstruction and survival in a general population sample from the USAThorax 2011 66:49-54.doi:10.1136/thx.2010.147041 [Google Scholar]
[21]. Duck-Chul L, Long-Term Effects of Changes in Cardiorespiratory Fitness and Body Mass Index on All-Cause and Cardiovascular Disease Mortality in MenCirculation 2011 124:2483-90.doi: 10.1161/CIRCULATIONAHA. 111.038422 [Google Scholar]
[22]. Gari Mamdooh Abdullah, Moderate versus high intensity aerobic exercise training on glycemic control and anti-inflammatory effects on non insulin dependent diabetic patientsWorld Applied Sciences Journal 2010 8(6):667-71. [Google Scholar]