In our country diabetes poses burden to healthcare and financial system. The International Diabetes Federation (IDF) estimates the total number of people in India suffering from diabetes to be around 50.8 million in 2010, rising to 87.0 million by 2030. According to WHO, India will be a worldwide diabetic capital in 2025 [1].
This debilitating disease causes various microvascular complications such as retinopathy, nephropathy and neuropathy. The complications of diabetes are attributed to the biochemical and structural changes in basement membrane proteins in different organ systems. Chronic hyperglycaemia leads to non-enzymatic glycosylation of proteins such as collagen, elastin etc leading to thickening of basement membrane and micro–angiopathy. Micro–angiopathy in alveoli may restrict lung volumes and capacities [2].
Thus it can be hypothesised that alterations in pulmonary function, especially diminished alveolar gas exchange can occur in patients with diabetes mellitus. There were limited literature and evidence available regarding the role of type 2 diabetes over the structural changes and micro–angiopathy. So by this study we aimed to assess the alveolar gas exchange and pulmonary function in patients with type II diabetes mellitus and the effect of hyperglycaemia and duration of diabetes by comparing with non-diabetic controls.
Material and Methods
This cross sectional study included 30 patients with Type 2 diabetes of age 30-60 years, attending the Diabetic out patient department, SRM Medical college Hospital and Research Centre. Thirty age and sex matched normoglycemic individuals were included as the comparison group. Institutional Ethical committee approval was obtained and written consent was taken from the study subjects.The diagnosis of diabetes was determined according to WHO criteria as follows, fasting blood sugar ≥126 mg/dl and 2 hour post load glucose test ≥200 mg/dl [5]. Blood glucose levels were estimated by Glucose Oxidase-Peroxidase GOD/POD method and the glycated haemoglobin (HbA1C) was determined by Immuno-inhibition method, both using Beckman Coulter auto-analyzer. Subjects with any cardiac or respiratory diseases, anaemia, connective tissue diseases, musculoskeletal disorders, and patients under medications that affect pulmonary function and those with significant occupational history that affects the lung and smokers were excluded from the study.
The pulmonary function test was performed according to American Thoracic Society (ATS) criteria [6] in all the participants using Easyone Pro computerised spirometer at the Research laboratory in the Department of Physiology, SRM Medical College Hospital & Research Centre. All the tests were conducted in sitting posture and all the subjects performed spirometry three times at an interval of 15 minutes and the best of the three was taken into the account. The parameters measured were Forced Vital Capacity (FVC), Forced Expiratory Volume in 1 second (FEV1), Forced Expiratory Volume Percentage (FEV1 /FVC), Peak Expiratory Flow Rate (PEFR), Forced Expiratory Flow (25 – 75%), Peak Inspiratory Flow (PIF) and Forced Inspiratory Vital Capacity ( FIVC) with calculation of their percentage predictive values. FEV1 is the volume of air exhaled in the first second during FVC manoeuvre. FEV1/FVC% is the volume of air expired in the first second, expressed as percentage of FVC.
The diffusing capacity of lung for carbon monoxide (DLCO), Alveolar Ventilation (VA) and DLCO/VA ratio and Total Lung Capacity (TLC) were determined by single breath Carbon Monoxide (CO) diffusion test. The test was performed using a gas mixture of 10% helium, 0.3% CO, 21% oxygen and the rest was nitrogen. Diffusion capacity is defined as the volume of gas (1ml) diffused through the alveolar-capillary membrane under a certain pressure gradient (1mmHg) in a certain period of time (10 seconds). Carbon monoxide has a high affinity for haemoglobin. The integrity of alveolar-capillary membrane is the main factor affecting the diffusion of Carbon monoxide. The ratio of DLCO to alveolar ventilation (DLCO/VA) was used to assess the alveolar membrane permeability [4].
To assess the association of diabetes control as measured with HBA1c levels we categorized HBA1c values into equal or less than 7% and greater than 7%, and tested for significance with the t-test. We selected this cut off point as a priori because it is usually selected in clinical practice to discriminate between appropriate and inappropriate control [7].
The spirometric volumes were expressed as litres and DLCO values were expressed as ml/mmHg/min. All the data were entered in MS excel spread sheet and the statistical analysis was done using SPSS version 17.0. The data were expressed as mean ± standard deviation. Descriptive tables were generated and student t test was used to demonstrate the findings. p value of less than 0.5 was considered to be statistically significant.
Results
To study the role of diabetes over the pulmonary function, a comparison group of non-diabetic individuals after confirming their glycaemic status were used who had normal pulmonary functions. Hence care has been taken to avoid variations in basic characteristics between the diabetics and the comparison group which influence the pulmonary function, such as age, height, weight and as well as BMI [Table/Fig -1].
Comparison of anthropometric data between patients with type II diabetes mellitus and non-diabetic individuals
| Parameters | Group I Diabetic patients (n= 30) (Mean ± SD) | Group II Controls (n=30) (Mean ± SD) | p value |
|---|
| Age in years | 44.8 ± 8.9 | 39.4 ± 11.7 | 0.09 |
| Height in cms | 158 ±11 | 161 ±8.8 | 0.226 |
| Weight in kg | 65 ±10.9 | 64.7 ± 11.6 | 0.926 |
| BMI$ [Weight in Kg/ (Height in meters)2] | 26.06 ± 4.03 | 24.81 ± 4.24 | 0.244 |
$ BMI – Body Mass Index
On comparing the diabetics and non-diabetic individuals,Forced Vital Capacity (FVC), Forced Expiratory Volume in first second (FEV1), Peak expiratory flow rate ( PEFR), FIVC, PIF and Total lung capacity ( TLC) were significantly lower (p < 0.05) in Type 2 diabetes patients compared to non diabetic subjects [Table/Fig -2].
Comparison of pulmonary function test parameters between patients with type II diabetes mellitus and non-diabetic individuals
| Pulmonary function parameters (Unit) | Group I Diabetic patients (n= 30) (Mean ± SD) | Group II Controls (n=30) (Mean ± SD) | P value |
|---|
| FVC (L) | 2.37 ± 0.7 | 2.9 ± 0.5 | 0.001* |
| FEV1 (L) | 1.9 ±0.6 | 2.4 ± 0.5 | 0.001* |
| FEVI/FVC | 96.1 ±10.1 | 97.5 ± 9.3 | 0.532 |
| FEF25-75% (L/s) | 2.2 ±1.0 | 2.6 ± 1.0 | 0.101 |
| PEFR (L/s) | 5.2 ±2.0 | 6.2 ± 1.7 | 0.040 * |
| FIVC (L) | 2.1 ±0.7 | 2.7 ±0.6 | 0.002* |
| PIF [L/s] | 2.8 ±1.2 | 3.5 ± 1.5 | 0.029 * |
| TLC (L) | 3.6 ±0.7 | 4.1 ± 0.6 | 0.001* |
| DLCO (ml/min/mmHg) | 15.07 ±3.7 | 19.1 ± 3.7 | 0.0001* |
| DLCO/VA [ml/min/mmHg/L] | 3.7 ± 1.4 | 5.07 ± 0.9 | 0.002* |
*Statistically significant
The measures of the integrity of alveolar-capillary membrane such as DLCO and DLCO/VA were significantly lower in patients with type II diabetes than the comparison group [Table/Fig-2]. The effect of glycemic status of the diabetics on DLCO and DLCO/VA were shown in the [Table/Fig – 3 and 4] respectively.
Comparison of pulmonary function test parameters between type II diabetic patients with HbA1c < 7 or > 7
| Pulmonary function parameters (Unit) | Diabetic patients with HbA1c < 7 (n= 18) (Mean ± SD) | Diabetic patients with HbA1c > 7 (n=12) (Mean ± SD) | P value |
|---|
| FVC (L) | 2.51 ± 0.71 | 2.17 ± 0.72 | 0.2 |
| FEV1 (L) | 2.04 ±0.63 | 1.76 ± 0.58 | 0.23 |
| FEVI/FVC | 93.89 ±10.7 | 99.58 ± 8.5 | 0.13 |
| FEF25-75% (L/s) | 2.37 ± 0.95 | 2.03 ± 1.15 | 0.38 |
| PEFR (L/s) | 5.57 ±2.17 | 4.1 ± 1.71 | 0.26 |
| FIVC (L) | 2.35 ±0.79 | 1.91 ±0.67 | 0.13 |
| PIF [L/s] | 2.81 ±1.4 | 2.81 ± 0.88 | 1.00 |
| DLCO [ml/min/mmHg] | 16.68 ± 1.63 | 12.64 ± 1.06 | 0.001* |
| DLCO/VA [ml/min/mmHg/L] | 4.42 ± 2.46 | 3.2 ± 1.5 | 0.03* |
| TLC (L) | 3.33 ±0.5 | 3.31 ±0.95 | 0.95 |
*Statistically significant
Effect of glycemic status (HbA1c) on DLCO among diabetics
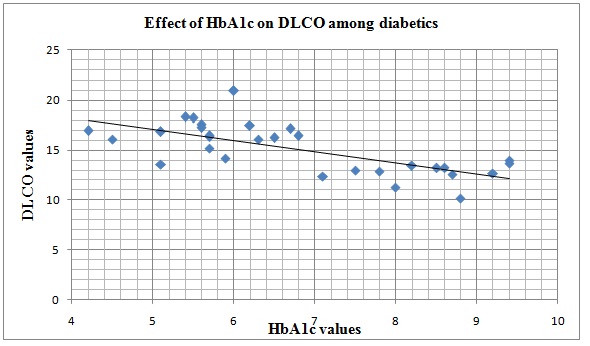
The best parameter to evaluate the metabolic control level of diabetes is HbA1c level. To evaluate the effect of the metabolic control of DM on lung functions, patients were divided into two sub groups based on their HbA1c levels: well controlled [n= 18; HbA1c < 7%] with mean HbA1c 5.69 ± 0.69 and poorly controlled[n=12; HbA1c > 7%] with mean HbA1c 8.43 ± 0.73. The DLCO ( p value = 0.001) and ratio of DLCO / VA ( p value = 0.03) were significantly reduced among the diabetics with poor glycemic control (HbA1c > 7). There was no significant difference in the other pulmonary function parameters between the diabetics and non-diabetic individuals. [Table/Fig -5].
Effect of glycemic status (HbA1c) on DLCO/VA among diabetics
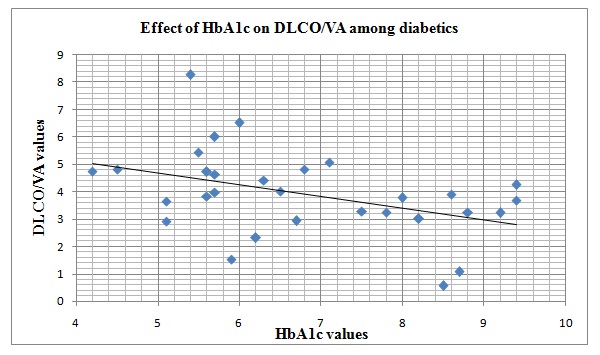
To determine the effect of duration of diabetes on pulmonary functions, the diabetic patients were divided into two subgroups: one with diabetes duration < 10 years(n=19) with mean duration of 3.10 ± 1.76 years and the other group with diabetes duration >10 years (n=11) with mean 13.81 ± 1.72 [Table/ Fig -6]. On statistical analysis, duration of diabetes was not influencing the pulmonary function of these diabetic individuals.
Comparison of pulmonary function test parameters between type II diabetic patients with duration of diabetes < and > 10 years
| Pulmonary function parameters (Unit) | Diabetic duration < 10 years (n= 19) (Mean ± SD) | Diabetic duration > 10 years (n= 11) (Mean ± SD) | p value |
|---|
| FVC (L) | 2.46 ± 0.75 | 2.22 ± 0.68 | 0.31 |
| FEV1 (L) | 1.97 ± 0.66 | 1.84 ± 0.55 | 0.60 |
| FEVI/FVC | 95.35 ± 9.29 | 97.55 ± 11.78 | 0.58 |
| FEF25-75% (L/s) | 2.08 ± 1.14 | 2.5 ± 0.78 | 0.28 |
| PEFR (L/s) | 5.55 ±2.06 | 4.65 ± 1.88 | 0.24 |
| FIVC (L) | 2.35 ±0.84 | 1.87 ±0.54 | 0.10 |
| PIF [L/s] | 3.06 ±1.37 | 2.38 ± 0.71 | 0.14 |
| DLCO [ml/min/mmHg] | 15.29 ± 2.74 | 14.67 ± 1.93 | 0.51 |
| DLCO/VA [ml/min/mmHg/L] | 4.12 ± 2.54 | 3.77 ± 1.7 | 0.53 |
| TLC [L] | 3.4 ± 0.79 | 3.19 ± 0.53 | 0.77 |
Discussion
Based on this study, it was evident that the pulmonary functions were decreased in diabetic individuals in comparison with age and sex matched non-diabetic subjects. Specifically, diabetics had a significant reduction in FVC, FEV1, PEFR, FIVC, PIF and TLC relative to their matched normoglycemic comparision group . These results were similar to the observations made in other studies which documented decreased pulmonary function in diabetics [8–11].
In this study there was significant reduction in mean FVC and the mean FEV1 values in all diabetic patients. These findings were consistent with findings of Davis et al., Irfan M et al., and Shravya Keerthi et al., [11–13]. The decrease in FVC, FEV1 and normal value of (FEV1/FVC) shows restrictive pattern of lung disease in the diabetics. Similar findings were observed by Swati H shaw et al., Irfan M et al., and Kanyakumari DH et al., [8,12,14]. There was increased cross-linkage formation between polypeptides of collagen in pulmonary connective tissue, which decreases FVC and hence was responsible for restrictive respiratory defects.
In our study there was a significant decrease in PEFR in diabetic subjects which is similar to other studies [13, 15, 16]. This may be related with the poor mechanical properties of the lung, like lung compliance and elastic recoil of lungs. The alteration in collagen and elastin ratio is the main pathological factor in the diabetic patients [17]. In addition, myopathic or neuropathic changes and alterations in the bronchial reactivity affects the respiratory muscles further which impairs the endurance and efficiency of ventilatory pump [18, 19].
The findings of our study were in agreement with the of the study of Davis et al., [11] who conducted a large community-based study in Western Australia in Type 2 diabetic patients and demonstrated that VC, FVC, FEV1, and PEF were decreased. We also found that the TLC was significantly low in diabetic than the comparison group which was in concordance with the other study findings [17, 20]. Impairment in lung function of patients with diabetes were believed to be the consequence of biochemical alterations in the connective tissue constituents of the lung and micro–angiopathy due to the non–enzymatic glycosylation of proteins induced by chronic hyperglycaemia. DLCO and the ratio of DLCO/ VA which determines the alveolar permeability were significantly reduced which revealed decline in pulmonary gas exchange in the diabetic group. This was consistent with the findings of other studies [3, 4, 21–22] which may be due to thickening of alveolar and small vessel walls.
DLCO and ratio of DLCO / VA were significantly reduced among the diabetics with poor glycaemic control (HbA1c > 7) and there was no significant difference in other pulmonary functions. It was also reasonable to expect that a decrease in DLCO may occur with the increasing hyperglycaemia in diabetes when the prevalence of micro–angiopathic complications also increases which was observed and stated by Sanjeev sinha et al., [23–25].
In diabetes, pathophysiological mechanisms that have played the role in micro–angiopathy cause damages in alveolar basement membrane due to the presence of abundant connective tissue and extensive microvascular circulation.
Some authors postulated that the thickened alveolar interstitium may be a reflection of the increase in lysyl oxidase activity, an enzyme that plays a major role in connective tissue formation and whose activity has been shown to have increased in rats with experimentally induced diabetes [26].
Studies conducted by Davis et al., [11] and Mckeevear et al., [27] identified pulmonary functions like FVC, FEV1 were significantly reduced in diabetics with poor glycemic control. Davis et al., identified that strong predictor of reduced lung function was the level of glycemic control and an increase of 1% in mean HbA1c was associated with a decrease of 4% in predicted forced vital capacity (FVC) and reduced lung function was an independent predictor of all-cause mortality with a 10% reduction in FEV1 associated with a 12% increase in all-cause mortality.
To find the effect of duration of diabetes over the lung functions of diabetics, we compared the lung functions of diabetics with duration < 10 years and > 10 years. None of the pulmonary functions are significantly different between the two groups in this study which was similar to the studies conducted by Swati H shaw et al.,[6] and Pinnar Cellik et al., [28]. However, Barret-Connor et al., [29] found that FEV1 and FVC were low in diabetic cases, who had diabetes for more than 10 years and in hyperglycaemics., which became more apparent with the increase in duration of diabetes. Our study shows that the duration of diabetes had not influenced the lung functions. This may be due to the fact that, our study was being descriptive in nature. If it might be a follow-up study, this result may differ.
Conclusion
Thus this study infers that diabetes has a significant effect over the pulmonary function. Though this study couldn’t identify the effect of duration of diabetes over the lung function, this study concludes that hyperglycaemia has a detrimental effect over the alveolar diffusion capacity which is the vital function of the lung. As a conclusion, microangiopathy, which occurs during the course of diabetes, causes damages not only the kidneys, eyes, and nervous system but also the alveolar basement membrane. Indeed, it’s time to add the spirometer which is a non-invasive and a cost effective tool for monitoring diabetes and its important sequelae.
$ BMI – Body Mass Index
*Statistically significant
*Statistically significant