Verruciform Xanthoma (VX) is a relatively rare benign mucocutaneous lesion of unknown aetiology. VX occurs predominantly in oral cavity which also occasionally affects skin and genital mucosa. It was first reported in the oral cavity in 1971. This rare harmless lesion usually presents as sessile or pedunculated, appear as a papule or single plaque showing verrucous or papillomatous mucosal growth with variable color from reddish pink to gray. In majority of oral cases, it affects gingiva and alveolar mucosa that may be mistaken for benign, premalignant and malignant conditions. VX is diagnosed with certainly only on histopathologic examination. Histologically VX is characterized by the presence of parakeratinized epithelium showing papillary or verrucous growth with thin rete ridges and connective tissue papillae extending up to the surface. The papillae characteristically consist of foam cells also called xanthoma cells. Here we describe a case report of verruciform xanthoma occurring on the buccal mucosa in a 42–years old male patient along with its clinical, pathogenesis, histological features and treatment modalities discussed.
Verruciform xanthoma, Oral cavity, Pathogenesis, Xanthoma cells
Case Report
A 42–years old male patient reported with a chief complaint of growth in the left buccal mucosa since 8 months. Medical, surgical, dental, family and personal histories were not noteworthy except the patient has the habit of smoking 8 to 10 beedies per day from the past 20 years. Intra–oral examination revealed a solitary pedunculated cauliflower like growth seen on the left buccal mucosa opposite to 36 and 37, measuring about 2 x 2 cm in size, soft to firm in consistency, non tender and not fixed to the underlying mucosa [Table/Fig-1]. Based on the habit, site and solitary growth, clinically diagnosis of verrucous carcinoma was made. An excisional biopsy was performed under local anesthesia and was sent for histopathological examination.
A solitary cauliflower like growth seen on the left buccal mucosa

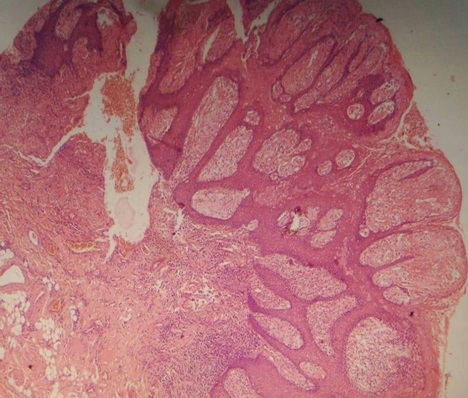
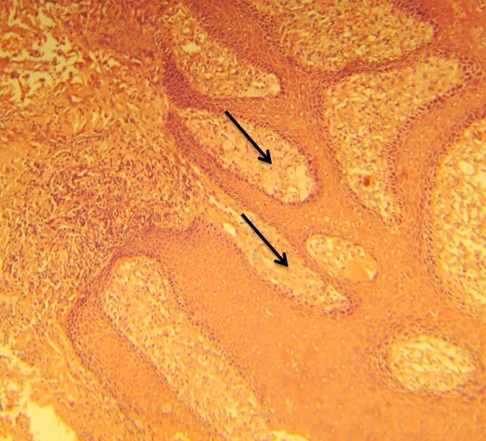
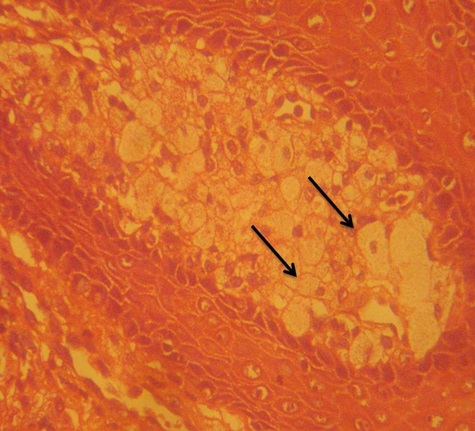
On histopathological examination, haematoxylin and eosin stained sections showed papillary projections lined by stratified epithelium along with underlying connective tissue stroma in scanner (4X) view [Table/Fig-2]. Under low power magnification (10X) the epithelium was parakeratinized stratified squamous type. Between the strands of epithelium, the connective tissue papillae extends up to the surface with a thin layer of epithelium present over it. In these extensions the connective tissue appeared to be replaced by large cells [Table/Fig-3]. Under high power magnification (40X) these large swollen cells showed clear to eosinophilic granular cytoplasm with eccentrically placed nuclei [Table/Fig-4]. The large swollen cells that filled the connective tissue papillae between the epithelial rete ridges are called foam cells or xanthoma cells. The underlying connective tissue stroma was showing mild to moderate chronic inflammatory cell infiltrate chiefly composed of lymphocytes. Based on these histopathological features, a diagnosis of verruciform xanthoma was made. On follow up, neither malignant transformation nor recurrence of the lesion has been reported after excision.
Photomicrograph showing papillary projections lined by stratified epithelium along with underlying connective tissue stroma. (H & E, 4x)
Photograph showing papillary projections lined with thin epithelium and core of connective tissue extending into the epithelium. (H&E,10x)
Photomicrograph showing large swollen cells that filled the connective tissue papillae between the epithelial rete ridges. The cells show clear to eosinophilic granular cytoplasm with eccentrically placed nuclei and are called foam cells or xanthoma cells. (H & E, 40x)
Discussion
Verruciform Xanthoma (VX) is an uncommon clinicopathologic entity that predominantly affects the oral cavity and sometimes skin and genital mucosa [1]. It was first described by Shafer in 1971 where he described 15 cases of this condition in the oral cavity and coined the term ‘verruciform xanthoma’ [2]. Most frequently encountered sites in the oral cavity is masticatory mucosa with gingival margin followed by hard palate, tongue, buccal mucosa, floor of the mouth, alveolar mucosa, soft palate and junction between hard and soft palate [3]. VX also occurs in non–oral sites and the first report of involvement of an extra–oral site was described by Santa Cruz in 1979 where he reported two cases of VX in the vulva [4]. Since then, several reports of VX in non–oral sites especially on anogenital skin have been appeared in the literature [5].
VXs are usually asymptomatic, solitary though multi–focal lesions have reported. They are slow growing lesions, evolves to sizes varying from 0.2 to 2 cm. VX though has a slight male preponderance with a reported male: female ratio of 1.1:1; below the age of 50 years male to female ration is 1.6:1 and this ratio is reversed in favor of females which is about 0.8:1 respectively after the age of 50 years. Majority of cases have been reported in Caucasians [3,6,7]. In most of the cases VX tends to occur as an isolated lesion but in many cases the lesion developed in association with the other diseases like oral pemphigus vulgaris, carcinoma in situ, lichen sclerosus, solar keratoses, discoid lupus erythematosus, lichen planus and congenital hemidysplasia with ichthyosiform erythroderma and limb defects (CHILD syndrome) [8]. Similar findings are seen in the present case where VX is occurring in a male patient of age 42 years on the left buccal mucosa measuring about 2 x 2 cm in size, asymptomatic, not fixed to the underlying mucosa and is not associated with any other lesion.
Clinically VX appear as a papule or single plaque showing verrucous or papillomatous mucosal growth with variable color ranging from reddish pink to gray that may be mistaken for a viral wart, benign, premalignant and malignant conditions. Differential diagnosis includes squamous papilloma, verruca vulgaris, verrucous carcinoma and squamous cell carcinoma. Clinically, majority of the squamous papillomas are found to be round in shape, whitish, flaccid in consistency and pedunculated [9]. The lesions of verruca vulgaris are circumscribed, firm, elevated papule with papillomatous hyperkeratotic surface [10]. Verrucous carcinoma lesions are almost always large, exophytic, soft, fungating, slow growing neoplasms with a pebbly mamillated surface [11]. Whereas squamous cell carcinoma presents as an ulcer with fissuring or raised exophytic margins. It may also present as a lump, as a red lesion (erythroplakia), as a white or mixed white and red lesion, as a non-healing extraction socket or as a cervical lymph node enlargement, characterized by hardness or fixation [12]. Diagnosis is made on the basis of histological appearance of the lesions showing hyperplastic parakeratinized squamous epithelium showing papillary or verrucous growth with elongated thin rete ridges of relatively uniform depth [13].
Now parast et al., demonstrated three architectural appearances of VX when viewed under light microscope:
1. A warty or verrucous appearance,
2. A papillary or cauliflower architecture and
3. A slightly raised or flat lesion [14].
Histologically VX is characterized by the presence of parakeratinized epithelium showing papillary or verrucous growth with thin rete ridges and connective tissue papillae extending up to the surface. The papillae characteristically consists of foam cells also called xanthoma cells (xanthos = yellow). These cells are not seen beneath the level of the adjacent rete ridges and may completely fill the papilla. They contain lipid as well as periodic acid Schiff (PAS) positive, diastase-resistant granules. In the lamina propria, chronic inflammatory infiltration may also be observed. [2] Similar histopathological features are seen in the present case where sections show papillary projections lined by parakeratinized stratified squamous epithelium along with underlying connective tissue stroma. Between the strands of epithelium, the connective tissue papillae extended up to the surface with a thin layer of epithelium present over it. In these extensions the connective tissue appeared to be replaced by foam cells or xanthoma cells. Excision is usually the treatment of choice and VX usually doesn’t recur. [2] In the present case too there is no recurrence of the lesion reported after excision.
Given the occurrence of VX in masticatory mucosa, mainly in the gingiva, the possibility of trauma or inflammatory reasons can be considered as main etiological factor. Zagarelli et al., suggested the concept that local trauma and inflammation lead to epithelial entrapment and the cause of accumulation of lipid containing macrophages is epithelial degeneration. The products of epithelial breakdown elicit an inflammatory response which is manifested by a predominant neutrophilic infiltrate in the epithelium and a subsequent release of lipid material through the epithelium that finally is scavenged by the macrophages. [15] This theory was supported by several authors and suggested a local irritant as the initiator of this process. Ide et al., suggested few possible oral agents as etiological factors such as wet micro–environment, periodontal pathogens, mechanical stimuli, tobacco, alcohol, drugs, sensitizing or allergic substances of food stuffs and dental materials [16].
Mostafa et al., suggested that epithelial hyperplasia with elongation of the epithelial rete ridges is illusory and is not a proliferation of epithelial cells with downward growth of the rete ridges but rather results from the upward pushing effect of the accumulated macrophages towards the epithelium. This reflects the thinning of the epithelium overlying the macrophages in the connective tissue papillae [17]. Nowparast et al., suggested that the verrucous and papillary architecture may be secondary to the presence of foam cells which affect the nutrition and metabolism of the epithelial cells leading to a hyperkeratotic change [14].
Viral infection could be associated to VX since extra–oral lesions usually occur in the genitalia. Despite the lack of intraepithelial inclusions or pronounced vacuolation, Santa Cruz and Martin also suggested that a viral cause was possible. However Hu et al., did not detect human papilloma virus in their cases by in-situ-hybridization. [18] Many histochemical, immunohistochemical and ultrastructural studies have been done so far but even today the pathogenesis of VX is obscure and needs to be clarified.
No conclusive evidence of the malignant transformation of preexisting VX exists in the literature. Murat-Susic et al., presented a case of VX associated with epidermolysis bullosa and highlighted that the concomitant presence of VX in patients with epidermolysis bullosa could pose an increased risk of SCC occurrence[19].
Conclusion
In conclusion, Verruciform Xanthoma (VX) is a localized lesion whose correct diagnosis requires surgical excision and careful histological examination. Although VX has an asymptomatic clinical course, histopathologically it still poses a challenge to the understanding of its pathogensis. A need to investigate associations with other epithelium lesions especially, those related to greater carcinogenesis risk is also required.
[1]. Damm DD, Fantasia JE, Rough white patch of gingiva. Verruciform XanthomaGen Dent 2002 50:378-80. [Google Scholar]
[2]. Shafer WG, Verruciform xanthomaOral Surg Oral Med Oral Pathol 1971 31:784-49. [Google Scholar]
[3]. Philipsen HP, Reichart PA, Takata T, Ogawa I, Verruciform xanthoma-biologcal profile of 282 oral lesions based on a literature survey with nine new cases from JapanOral Oncol 2003 39:325-36. [Google Scholar]
[4]. Santa Cruz DJ, Martin SA, Verruciform xantohoma of the vulva: Report of two casesAm J Clin Pathol 1979 71:224-8. [Google Scholar]
[5]. Joshi Rajiv, Ovhal Ajay, Verruciform xanthoma: Report of five casesIndian J Dermatology 2012 57(6):479-82. [Google Scholar]
[6]. Polonowita AD, Firth NA, Richa AM, Verruciform xanthoma and concomitant lichen planus of the oral mucosa. A report of three casesInt J Oral Maxillofac Surg 1999 28:62-6. [Google Scholar]
[7]. Iamaroon A, Vickers RA, Characterization of verruciform xanthoma by in situ hybridization and immunohistochemistryJ Oral Oathol Med 1996 25:395-400. [Google Scholar]
[8]. Kunal S, Alka DK, Seema H, Verruciform xanthoma: Report of two cases and review on pathogenesisJOMFP 2008 12:41-4. [Google Scholar]
[9]. Thalassa EC, Sandra AM, Flaviana DV, Ana TMM, Nadia LL, Oral squamous papilloma: clinical, histologic and immunohistochemical analysesJournal of Oral Science 2009 51(3):367-72. [Google Scholar]
[10]. Vela DD, Sharma Rajeev, Durgesh NB, Extensive mucocutaneous verruca vulgaris in a non–immunocompromised patientInt J Clinic Paediatric Dent 2011 4(1):65-68. [Google Scholar]
[11]. Rohan RW, Verrucous carcinoma of the oral cavity: A clinical and pathological study of 101 casesOral Oncology 2009 45:47-51. [Google Scholar]
[12]. Markopoulos Anastasios K, Current Aspects on Oral Squamous Cell CarcinomaThe Open Dentistry Journal 2012 6:126-30. [Google Scholar]
[13]. Hatakeyama Marcia, Alonso Juliana MSL, Marinaldo Guilhermino, Brandao Adriana A. H., Cavalcante Ana Sueli R, Verruciform xanthoma located in anterior gingivalJ Clin Exp Dent 2010 2(2):82-4. [Google Scholar]
[14]. Nowparast B, Howell FV, Rick GM, Verruciform xanthoma: A clinicopathologic review and report of fifty four casesOral Surg Oral Med Oral Pathol 1980 51:619-25. [Google Scholar]
[15]. Zegarelli DJ, Zegarelli-Schmidt EC, Zegarelli EV, Verruciform xanthoma: Further light and electron microscopic studies, with the addition of a third caseOral Surg Oral Med Oral Pathol 1975 40:246-56. [Google Scholar]
[16]. Ide F, Obara K, Yamada H, Mishima K, Saito I, Kusama K, Cellular basis of verruciform xanthoma: immunohistochemical and ultrastructural characterizationOral Dis 2008 14:150-7. [Google Scholar]
[17]. Mostafa KA, Takata T, Ogawa I, Ijuhin N, Nikai H, Verruciform xanthoma of the oral mucosa: A clinicopathological study with immunohistochemical findings relating to pathogenesisVirchows Arch A 1993 423:243-8. [Google Scholar]
[18]. Hu JA, Li Y, Li S, Verruciform xanthoma of the oral cavity: clinicopathological study relating to pathogenesis. Report of three casesAPMIS 2005 113:629-34. [Google Scholar]
[19]. Murat-Susic S, Pastar Z, Dobric I, Camino Varela A, Hutinec Z, Verruciform xanthoma in recessive dystrophic epidermolysis bullosa Hallopeau-SiemensInt J Dermatol 2007 46:955-9. [Google Scholar]