Infantile or Malignant Osteopetrosis: Case Report of Two Siblings
Tarakeswara Rao P.1, Sunita V.2, Gandhi T.P.3, Sri Harsha4
1 Associate Professor, Department of Paediatrics, Maharajah’s Institute of Medical Sciences, Nellimarla, Andhra Pradesh, India.
2 Assistant Professor, Department of Paediatrics, Maharajah’s Institute of Medical Sciences, Nellimarla, Andhra Pradesh, India.
3 Professor & HOD, Department of Paediatrics, Maharajah’s Institute of Medical Sciences, Nellimarla, Andhra Pradesh, India.
4 Post Graduate Student, Department of Paediatrics, Maharajah’s Institute of Medical Sciences, Nellimarla, Andhra Pradesh, India.
NAME, ADRESS, E-MAIL ID OF THE CORESPONDING AUTHOR: Dr. Tarakeswara Rao P, Department of Paediatrics, MIMS, Nellimarla, Vizianagaram, Andhra Pradesh, India.
Phone: +919441080069,
E-mail: p_tarakeswara@rediffmail.com
Infantile or Malignant osteopetrosis is a rare congenital disorder of bone resorption. It is caused by failure of osteoclasts to reabsorb immature bone. Severe infantile or malignant osteopetrosis present at birth or develops within the first few months of life. We are reporting here a case of two siblings with malignant osteopetrosis. Prominent clinical features included marked pallor, noisy respiration, progressive blindness and developmental delay.
Infantile, Malignant, Osteopetrosis
Introduction
Osteopetrosis or Albers-Schonberg disease is a rare hereditary metabolic bone disorder characterized by generalized skeletal sclerosis caused by a defect in bone resorption and remodeling. Abnormal resorption results in thickening of cortices, increased bony trabeculae and encroachment of marrow spaces leading to paucity of hemopoietic tissue. Autosomal recessive or malignant osteopetrosis present early in infancy and associated with short life span. Two siblings with early hematological and visual impairments are presented here.
Case 1
A 4–years–old girl, born out of consanguineous marriage, brought to Department of Paediatrics with complains of delayed milestones. She had history of repeated chest infections since birth. During these episodes the child had cough, noisy respirations and the chest retractions. She developed head control but never able to sit or stand. She could see and follow objects at 4 month of age. There was history of progressive diminished vision and distention of abdomen since early infancy.
Physical examination revealed large head, pallor, and pigeon chest with noisy respiration. Ocular examination revealed roving eye movements, nystagmus & inability to perceive even to bright light. Abdominal examination revealed hepatosplenomegaly. The child was completely bed ridden with grade IV Protein Energy Malnutrition (PEM). Fundus examination revealed bilateral optic atrophy.
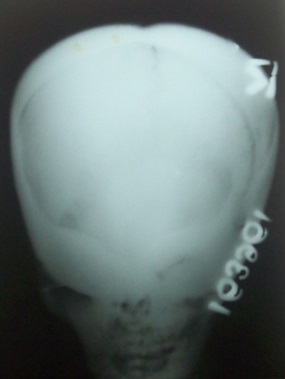
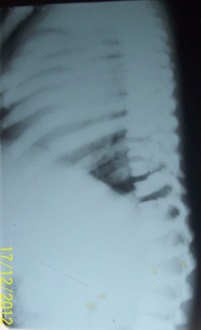
Laboratory investigations showed severe anaemia (Hb 2.5gm/dl), thrombocytopenia with leukocytosis. Peripheral blood smear showed normocytic,normochromic RBCs. Leukocytosis with immature forms (myleocytes, metamyleocytes and bandforms) and normoblasts (3-4/100wbc). Bone marrow aspiration was dry tap. A postero-anterior skull view [Table/Fig-1] showed enlargement of the calvarium with upward slanting of the greater sphenoidal alae and thickened orbital rims, creating the typical “space alien” face. Pneumatization of the maxillary and ethmoidal sinuses was absent. Lateral radiograph of the spine [Table/Fig-2] showed thickened endplates and anterior notching of the vertebral bodies, giving the appearance of “sandwich vertebrae.”
Radiograph of skull showing increased sclerosis, enlargement of calvarium, thickened orbital rims (“space alien” face appearance)
Lateral radiograph spine showing broad club shaped ribs, Thickened endplates and anterior notching of verterbral bodies, decreased marrow spaces in verterbral bodies giving characteristic appearance of “vertebra invertebra”
Diffuse cerebral atrophy, sub–acute sub–dural haematoma along both cerebral convexities, diffuse thickening and sclerosis of skull bones were seen on CT scan.
Case 2
Younger sibling 7–months–old presented to the department of paediatrics with repeated attacks of upper respiratory tract infection and delay in attainment of developmental milestones. There was no head control and social smile was not developed. Child was not following or reaching for objects. Child also failed to respond to sound of rattle or toys.
Examination revealed less weight for age head circumference was 98 percentile for age. Gross pallor and hepatosplenomegaly were present.
Eye examination revealed roving eye movement, dilated, non–reacting pupil. A pale optic disc (Optic atrophy) was seen on direct ophthalmoscopy. Lab investigations revealed low HB (7mg/dl), mild thrombocytopenia with leukocytosis. Peripheral smear showed normocytic,normochromic RBCs, thrombocytopenia and leukoerythroblastic picture. Bone marrow aspirate was dilute and showed only minimal cellularity. A lateral skull radiograph [Table/Fig-3] showed marked sclerosis with thickening of the skull base and calvarium, as in the elder sibling. A lateral radiograph of the spine Showed diffusely increased bone density and reduced marrow spaces in the vertebral bodies, with the characteristic “vertebra-in-vertebra” appearance. A postero-anterior radiograph of lower limbs [Table/Fig-4] showed diffusely increased bone density; subtle radiolucent banding at the distal end of the femur and proximal end of the tibia, indicating marrow activity at the ends and the characteristic “Erlenmeyer flask” appearance. A hand–wrist radiograph Table/Fig-5] showed a “bone-within bone” appearance of the metacarpals.
Radiograph of skull showing increased density of bones at base of skull, thickend calvarium

showing Generalised increased bone density with Erlenmeyer flask appearance

Radiographs of hands showing increased bone density and “bone in bone appearance”

Discussion
Osteopetrosis is very rare in most populations, estimated incidence is less than 1:200,000 birth [1]. It is much more common in consanguineous populations. It is very unusual to find it in two members of the same family. 4 types of osteopetrosis have been described [2]. Severe infantile or autosomal recessive types are present at birth or develop within first months of life. Based on the clinical history and radiographic findings, children were diagnosed having infantile or malignant type of osteopetrosis, with autosomal recessive inheritance.
Nasal obstruction and visual impairments are common initial Presenting symptoms [3]. Visual impairment results from bony encroachment on the optic foramina. Optic atrophy is also present in significant number of cases. In the series reported by phadke et al., optic atrophy was present in 3 out of 6 cases [4]. In the cases reported here both the siblings were totally blind. Nasal obstruction with sterterous breathing as early initial manifestation is seen in both the siblings.
Hematological manifestations associated with osteopetrosis include severe anemia, hepatosplenomegaly (resulting from compensatory extramedullary hemopoiesis). Ensuing hypersplenism leads to thrombocytopenia, leukopenia and haemolytic anemia [5]. Both the cases reported here had hematological Impairement developing within first few months of life. Early visual impairment with hematological disturbance was associated with poor outcome in children with malignant osteopetrosis [6,7]. Cases of malignant osteopetrosis with early visual and hematological impairement rarely survive beyond 1st decade of life [8]. Cases reported here have both early visual disturbance and hematological impairment indicating a poor prognosis.
A characteristic radiological feature seen in both girls was generalized increases in bone density, with a loss of distinction between cortex and medulla, which is typical of osteopetrosis.
Conclusion
Though rare, infantile osteopetrosis should be considered in differential diagnosis in a infant presenting with anemia with hepatosplenomegaly. Early and prompt diagnosis can be made by simple skeletal radiography. Prenatal screening of the subsequent pregnancies may be considered.
[1]. Worth HM, Principles and practice of oral radiologic interpretation ChicagoYear Book of Publishers 1963 [Google Scholar]
[2]. Van Hul W, Vanhoenacker F, Balemans W, Janssens K, De Schepper AM, Molecular and radiological diagnosis of sclerosing bone dysplasiasEur J Radiol 2001 40:198-207. [Google Scholar]
[3]. White SC, Pharoah MJ, Oral radiology: principles and interpretationSystemic diseases manifested in the jaws 2000 4th edSt. LouisMosby [Google Scholar]
[4]. Wilson CJ. Autosomal recessive osteopetrosis. Orphanet Encyclopedia, March 2003. http://www.orpha.net/data/patho/GB/ukmalosteo.pdf [Google Scholar]
[5]. Filho AM, De Castro Domingos A, de Freitas DQ, Whaites EJ, Osteopetrosis – a review and report of two casesOral Dis 2005 11:46-9. [Google Scholar]
[6]. Venkateshwar V, Voidya A, Roy P, Songeeta S, De JK, OsteopetrosisMed J Armed Forces India 2003 59:344-6. [Google Scholar]
[7]. Phadke SR, Gupta A, Pahi J, Pandey A, Gautam P, Malignant recessive osteopetrosisIndian Paediatr 1999 36:69-74. [Google Scholar]
[8]. Shaff MI, Mathis JM, Osteomyelitis of the mandible – an initial feature in late-onset osteopetrosisArch Otolaryngol 1982 :120-1.:108 [Google Scholar]