Laser Gingival Retraction: A Quantitative Assessment
Vamsi Krishna Ch1, Nidhi Gupta2, K. Mahendranadh Reddy3, N. Chandra Sekhar4, Venkata Aditya5, G.V.K. Mohan Reddy6
1 Senior Lecturer, Department of Dental, Sri Sai College of Vikarabad- 501101, India.
2 Professor, Department of Dental, Sri Sai College of Vikarabad- 501101, India.
3 Professor, Department of Dental, Sri Sai College of Vikarabad- 501101, India.
4 Professor, Department of Dental, Sri Sai College of Vikarabad- 501101, India.
5 Reader, Department of Dental, Sri Sai College of Vikarabad- 501101, India.
6 Senior Lecturer, Department of Dental, Sri Sai College of Vikarabad- 501101, India.
NAME, ADDRESS, E-MAIL ID OF THE CORESPONDING AUTHOR: Dr. Vamsi Krishna C.H., Senior Lecturer, Department of Dental, Sri Sai College of Vikarabad - 501101, India.
Phone: 919885767632,
E-mail: chvk_guntur@yahoo.co.in
Background: Proper gingival retraction improves the prognosis of crowns and bridges with sub gingival finishlines.Use of lasers assists the operator to achieve proper retraction with good clinical results.
Aims: The present study was intended to assess the amount of lateral gingival retraction achieved quantitatively by using diode lasers.
Settings and Design: Study was carried on 20 patients attended to a dental institution that underwent root canal treatment and indicated for fabrication of crowns.
Material and Methods: Gingival retraction was carried out on 20 teeth and elastomeric impressions were obtained. Models retrieved from the impressions were sectioned and the lateral distance between finish line and the marginal gingival was measured using tool makers microscope. Retraction was measured in mid buccal, mesio buccal and disto buccal regions.
Statistical Analysis: The values obtained were used to calculate the mean lateral retraction in microns.
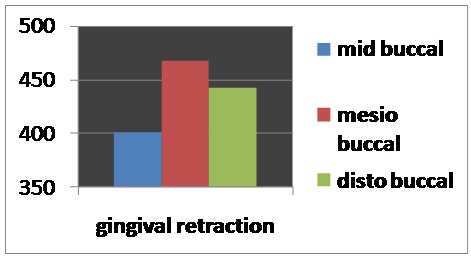
Results: Mean retraction values of 399.5 μm, 445.5 μm and 422.5μm were obtained in mid buccal, mesio buccal and disto buccal regions respectively.
Conclusions: Gingival Retraction achieved was closer to the thickness of sulcular epithelium and greater than the minimum required retraction of 200um.
Lasers, Gingival Retraction, Finish Line
Introduction
Accurate recording of finish line is a very important parameter for fabrication and successful prognosis of indirectly fabricated restorations. Exposure of sub-gingival finish line, with adequate moisture control to capture the finish line details in impression, is the main goal of gingival retraction procedure. Techniques such as mechanical, chemical, chemico mechanical and surgical methods have been followed conventionally for gingival retraction. Soft tissue lasers can be used as a substitute to conventional retraction techniques, because they provide adequate retraction along with hemostasis, with less working time and good patient comfort [1, 2]. The present study was done to test the effectiveness of diode lasers in gingival retraction procedures.
Material and Methods
Sample Selection
A total of 20 abutment teeth which were indicated for porcelain fused to metal crowns with labial sub-gingival shoulder and lingual supragingival chamfer finish line, were selected for the study. All the abutments were root canal treated, as they did not require local anaesthetic infiltration for tooth preparation. Out of 20 selected abutments, 10 abutments were anteriors and the remaining 10 were posterior teeth. All selected abutments had healthy gingiva, without a periodontal pathology.
Methodology
A diode laser with a fibre optic tip was used for the study (PICASSO diode laser, DENSPLY). After tooth preparation, retraction procedure was carried out by passing laser optic fibre in contact mode along the gingival sulcus, to remove sulcular epithelium. Laser energy was delivered which had a wavelength of 980nm and power of 0.8W [3], in continuous mode [4]. Continuous mode was used, as the laser energy was delivered in single stroke by passing the laser tip along the gingival sulcus [Table/Fig-1,2]. Laser tip was inserted 1mm into the gingival sulcus, to facilitate an accurate recording of finishline.Topical anaesthetic gel was applied onto the gingival sulcus region before retraction procedure. Local anaesthetic infiltration was not used for any of the abutments. After completing retraction, impressions were made by using addition silicon impression material and models were obtained from type IV stone (Kalrock, Kalabhai Karson Pvt. Ltd., India).
Gingival retraction using laser and post operative view

Lateral retraction measured using tool makers microscope from finish line to marginal gingiva

On stone models, mesio-buccal, mid-buccal and disto-buccal regions were selected for measurement of retraction. Two points were marked, one on finish line and the other one on crest of marginal gingiva, in three regions, for each abutment. Gingival retraction was assessed by measuring the distance between two points by using a toolmakers microscope.
Results
Measurements were carried out in three regions for each abutment and the results were subjected to a statistical analysis. Sample sizes of 20 abutment teeth were used. Retraction values which were obtained from mesio buccal, midbuccal and disto buccal regions were tabulated separately [Table/Fig-3]. Mean value was calculated from the data [Table/Fig-4].
Table showing the amount of retraction attained in mid buccal, mesio-buccal and disto- buccal regions(μm)
| Sample | Mid buccal (μm) | Mesio buccal (μm) | Disto buccal (μm) |
|---|
| 1 | 330 | 450 | 480 |
| 2 | 270 | 640 | 340 |
| 3 | 450 | 570 | 440 |
| 4 | 470 | 330 | 290 |
| 5 | 540 | 440 | 670 |
| 6 | 350 | 410 | 450 |
| 7 | 230 | 410 | 510 |
| 8 | 430 | 370 | 390 |
| 9 | 540 | 590 | 410 |
| 10 | 440 | 520 | 440 |
| 11 | 350 | 310 | 550 |
| 12 | 450 | 400 | 330 |
| 13 | 620 | 450 | 370 |
| 14 | 250 | 380 | 290 |
| 15 | 390 | 440 | 330 |
| 16 | 250 | 320 | 320 |
| 17 | 340 | 440 | 450 |
| 18 | 510 | 420 | 380 |
| 19 | 400 | 540 | 450 |
| 20 | 380 | 480 | 560 |
| MEAN | 399.5 | 445.5 | 422.5 |
Bar diagram showing the retraction attained in mid buccal, mesio-buccal and disto- buccal regions
Discussion
Marginal fit of indirect restorations depends on a proper gingival retraction and an accurate recording of the finishline.To capture the details of finishline accurately, retraction has to be done apically as well as laterally. A minimum lateral displacement of 0.2mm is required, for the impression material to flow into gingival sulcus with a dimensional accuracy [5].
Gingival sulcus is lined by sulcular epithelium with two basal layers of cells, from which remaining cell layers proliferate. If retraction procedure is carried out by removing superficial layers of epithelium, without damaging basal cell layer and connective tissue cells, the tissue changes and shrinkage of gingiva can be avoided. A minimum retraction of 0.2mm can be obtained by removing 200 um thickness of epithelium from the sulcus by using laser.
Diode lasers can be used for many soft tissue dental procedures, which include soft tissue surgeries [6–8] and periodontal [9,10] and peri-implant surgeries [11]. The study was carried out by using a diode laser for gingival retraction. As compared to conventional techniques, laser offers certain advantages such as lesser operating times and lesser collateral heat generation, with good hemostasis and patient comfort. But it does not offer much of tactile feedback to the operator during the procedure. Use of diode lasers for retraction purposes has shown less recession around natural teeth as compared to retraction cord (2.2 percent versus 10.0 percent) with laser. Retraction studies have shown bacterial reduction at treatment site and improvement in gingival marginal health after 1 week [12]. Thus, the use of diode lasers facilitates soft tissue management during impression making and serves as a valuable tool for the prosthodontist during the fabrication of accurate fixed prostheses.
Conclusion
The present study was carried out on 20 abutment teeth at three specified sites. Within the limitations of the study, the following conclusions were drawn,
A gingival retraction which ranged from 230 μm - 670 μm, closer to the thickness of sulcular epithelium and which was greater than the limit of minimum retraction of 200um.
Procedure can be carried out within less time.
A considerable improvement in patient comfort has been reported.
Further studies have to be carried out, to assess the amount of tissue which is removed, tissue changes, shrinkage and healing after using laser for retraction.
[1]. Lasers in clinical dentistryDent Clin North Am 2004 48(4):751-1145. [Google Scholar]
[2]. Donovan TE, Chee WW, Current concepts in gingival displacementDent Clin North Am 2004 48(2):433-44. [Google Scholar]
[3]. Samo Pirnat, Versatility of an 810nm diode laser in dentistry: an overviewJ of Oral Health and Laser Acad 2007 4:1-9. [Google Scholar]
[4]. Gherlone EF, Maiorana C, Grassi RF, Ciancaglini R, Cattoni F, The use of 980-nm diode and 1064-nm Nd: YAG laser for gingival retraction in fixed prosthesesJ Oral Laser Applications 2004 4(3):183-90. [Google Scholar]
[5]. Laufer BZ, Baharav H, Cardash HS, The linear accuracy of impressions and stone dies as affected by the thickness of the impression marginInt J Prosthodont 1994 7(3):247-52. [Google Scholar]
[6]. Goharkhay K, Moritz A, Wilder-Smith P, Schoop U, Kluger W, Effects on oral soft tissue produced by a diode laser in vitroLasers Surg Med 1999 25(5):401-06. [Google Scholar]
[7]. Crippa R, Calcagnile F, The Use of Laser Technology for Sub-mandibular Calculosis: A Case ReportJ Oral Laser Applications 2003 3:173-76. [Google Scholar]
[8]. Stubinger S, Saldamli B, Jurgens P, Ghazal G, Zeilhofer HF, Soft tissue surgery with the diode laser-theoretical and clinical aspectsSchweiz Monatsschr Zahnmed 2006 116(8):812-20. [Google Scholar]
[9]. Moritz A, Schoop U, Goharkhay K, Schauer P, Doertbudak O, Treatment of periodontal pockets with a diode laserLasers Surg Med 1998 22(5):302-11. [Google Scholar]
[10]. Kreisler M, Al Haj H, d’Hoedt B, Clinical efficacy of semiconductor laser application as an adjunct to conventional scaling and root planingLasers Surg Med 2005 Dec 37(5):350-55. [Google Scholar]
[11]. Maiorana C, Salina S, Santoro F, Treatment of Peri implantitis with Diode Laser: A Clinical ReportJ Oral Laser Applications 2002 2:121-27. [Google Scholar]
[12]. Lin PP, Horton JJ, Subgingival application of pulsed Nd: YAG laser reduces/inhibits bacteriaDent Res 1992 71:299 [Google Scholar]