Maxillofacial injuries are common and they occur in a variety of situations. All patients who undergo maxillofacial or head trauma, are presumed to sustain cervical spine injuries. Identification of cervical spine injuries is essential in management of trauma, because a missed injury can result in a catastrophic spinal cord injury. Advanced Trauma Life Support (ATLS) guidelines have suggested that routine use of cervical spine radiographs may not be required in an asymptomatic patient. We are presenting here a case with a cervical spine injury with no clinical deficits, found incidentally on panoramic radiographs which were advised for evaluation of the mandibular fracture. We suggest that importance has to be given to examination of the cervical spine on the panoramic radiographs as well.
Cervical spine fracture, Mandibular fracture, Treatment planning
Case Report
A 30-years old female reported to the hospital with the complaints of pain in the lower front teeth and difficulty in opening the mouth following a road traffic accident.
Patient was well oriented and she had no relevant medical history. On general physical examination, other concomitant injuries were ruled out clinically. Patient had a swelling and a 2cm linear lacerated wound over chin. An intra-oral examination revealed a sub-lingual haematoma and a disturbance in an occlusion which was provisionally diagnosed as a compound fracture of left parasymphysis of the mandible.
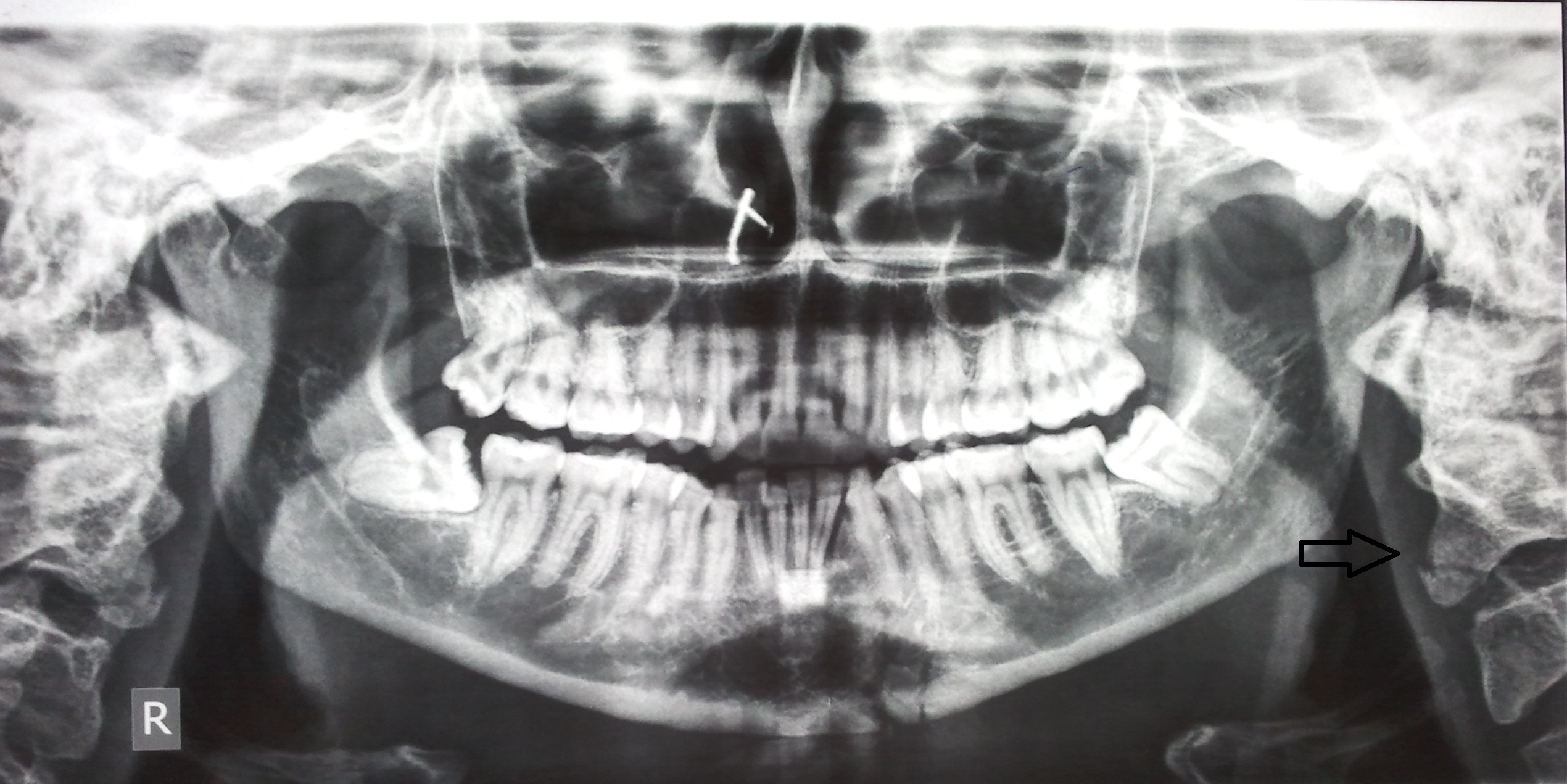
A panoramic radiograph was advised and the diagnosis was confirmed. Incidentally, we also noted a chip fracture (tear drop) in anteroinferior fragment of the C2 vertebra [Table/Fig-1]. C spine radiographs with lateral and AP views were taken [Table/Fig-2] and patient was referred for an orthopaedic opinion.
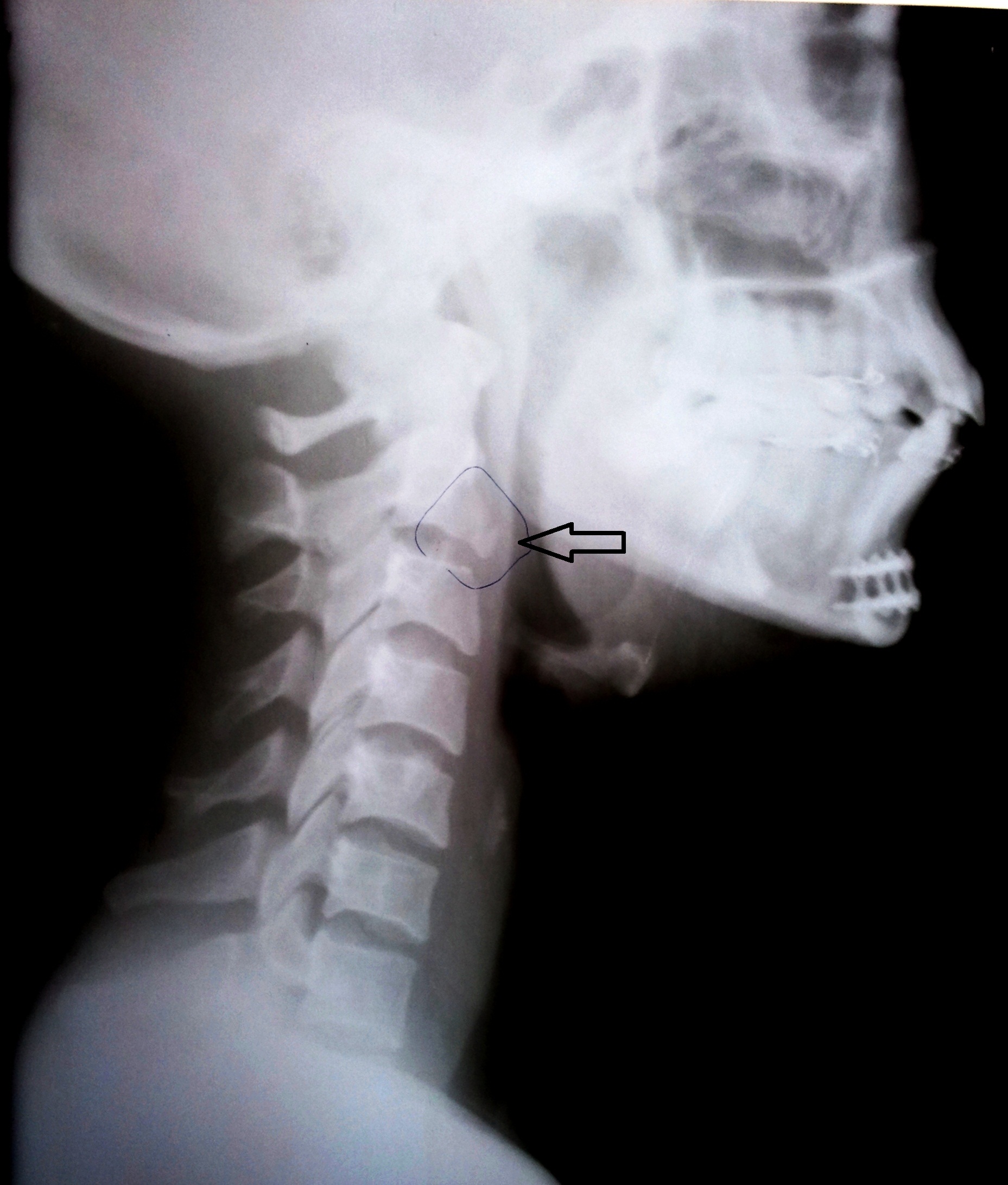
The observations which they made were chip fractures of anteroinferior fragment of the C2 vertebra, an anterior longitudinal ligament line, a posterior longitudinal ligament line, normal posterior elements and a posterior spinous process with no divergence or convergence, which confirmed that there was no instability or absence of neurological deficits. A minimal neck extension during intubation and a Philadelphia cervical hard collar were advised post operatively for 3 weeks. Patient underwent an open reduction and an internal fixation through the existing wound under GA successfully . The patient had an uneventful recovery.
Discussion
In maxillofacial trauma cases, the occurrence of associated injuries has been well documented .The incidence of cervical spine injuries in the presence of facial fractures accounts for up to 1.3-4% of the reported cases [1]. Concurrent mandibular and cervical spine fractures are reported to be 2.6% [2]. Cervical spine fractures can clinically present from mild soft tissue swellings with a normal neurologic picture, to obvious signs of muscle spasms and frank neurologic deficits [3].
Concomitant injuries are common in patients with facial trauma and they involve the head and the neighbouring neck region [4].The association between facial and cervical spine injuries has been frequently reported [5].
Because of the differences in the mechanisms of injury for both regions, most often, a high velocity trauma to the head or face is suspected for a combined occurrence. Therefore, the cervical spine has to absorb the appearing energy in relation to the trunk [6].
It is important to note that facial bone fractures present with swelling and haematoma, whereas spinal trauma does not always present with obvious symptoms. Cervical spine trauma can be missed, especially when pain from other parts of the body dominates [7].
ATLS guidelines have suggested that routine use of cervical spine radiographs may not be required in awake and alert trauma patients without neck pain [8].
In our case, on clinical examination, the patient was found to have no history of pain in the neck or clinically evident neurologic deficits. Hence, no cervical spine radiographs were advised.
C2 spine fracture was an incidental finding on panoramic radiographs which were advised for treatment planning for mandibular fractures.
Despite the support of ATLS guidelines, many trauma surgeons believe that cervical spine radiographs are necessary because of the legal, ethical, and financial implications of missed cervical spine injuries [8].
Conclusion
This case shows that cervical spine fractures can be missed in awake and alert blunt trauma patients with concomitant facial injuries (mandibular fractures), and since panoramic radiographs are frequently advised for evaluation of mandibular fractures, importance has to be given to the examination of the cervical spine on the panoramic radiographs as well. The mere absence of a neurologic deficit or pain does not rule out an injury to the cervical spine and it should be assumed in any patients with facial injuries until it is ruled out on an adequate roentogenic examination. Adequate methods of intraoperative stabilization of cervical spine injuries allow an appropriate and a timely management of facial fractures.
[1]. Beirne JC, Butler PE, Brady FA, Cervical spine injuries in patients with facial fractures: a 1-year prospective studyInt J Oral Maxillofac Surg 1995 Feb 24(11):26-29. [Google Scholar]
[2]. Ardekian L, Gaspar R, Peled M, Manor R, Laufer D, Incidence and type of cervical spine injuries associated with mandibular fracturesJ Craniomaxillofac Trauma 1997 Fall 3(2):18-21. [Google Scholar]
[3]. Brynin R, Yomtob C, Missed cervical spine fracture: chiropractic implicationsJ Manipulative Physiol Ther 1999 Nov-Dec 22(9):610-14. [Google Scholar]
[4]. McCabe JB, Angelos MG, Injury to the head and face in patients with cervical spine injuryAm J Emerg Med 1984 Jul 2(4):333-5. [Google Scholar]
[5]. Lewis VL Jr, Manson PN, Morgan RF, Cerullo LJ, Meyer PR Jr, Facial injuries associated with cervical fractures: recognition, patterns, and managementJ Trauma 1985 Jan 25(1):90-93. [Google Scholar]
[6]. Davidson JS, Birdsell DC, Cervical spine injury in patients with facial skeletal traumaJ Trauma 1989 Sep 29(9):1276-78. [Google Scholar]
[7]. Hackl W, Hausberger K, Sailer R, Ulmer H, Gassner R, Prevalence of cervical spine injuries in patients with facial traumaOral Surg Oral Med Oral Pathol Oral Radiol Endod 2001 Oct 92(4):370-76. [Google Scholar]
[8]. Gonzalez RP, Fried PO, Bukhalo M, Holevar MR, Falimirski ME, Role of clinical examination in screening for blunt cervical spine injuryJ Am Coll Surg 1999 Aug 189(2):152-57. [Google Scholar]