Digital radiography has come of age since mid-1980s, when the first digital X-ray sensors for dentistry were introduced by Francis Mouyen [1]. In recent years, digital imaging has generally superseded its conventional analogue, imaging in radiology, which has led to a profound change in the interpretation of radiological images. The reason for this paradigm shift from analog/film-based to digital/filmless imaging is multitudinous. Its main advantages over conventional film radiographs are speed, real time imaging and communication, convenience, lack of darkroom procedures and chemicals, availability of image improvement tools and dose reduction [2–6].
There are two ways of obtaining a digital image–direct and indirect. Direct digital imaging indicates that the original image is captured in a digital format. In indirect digital imaging, the image is captured in an analog format and it is then converted into a digital format, by using a scanner or a camera [1,3,7].
A digital camera has become an increasingly popular tool for digitizing conventional radiographs, by using the same image sensor technology as that of a direct digital radiograph – the charge-coupled device, to acquire the image. It promotes an instant image integration into dental practice software, further image enhancement and immediate data transmission, and it also aids in patient instruction and acceptance of the treatment [8].
With these advantages in mind, this study was aimed at subjectively analyzing and investigating the image clarity and the diagnostic quality of Indirectly Digitized Periapical Images (DIs) and Processed Digitized Periapical Images (PDIs) in comparison with those of Conventional Intraoral Periapical Radiographs (CRs).
Material and Methods
Forty two intraoral periapical radiographs of routine outpatients who visited the Department of Oral Diagnosis and Radiology were exposed. Only those teeth which clinically substantiated the diagnosis of a pulpal involvement with a subsequent periapical pathosis, were selected for the study. An informed consent from each patient and permission from the institutional ethical review board were obtained. A calibrated dental X-ray unit (Evolution X-300, Toshiba Co, Italy) at 70 kVp and 8 mA, along with an E speed film (Kodak Eastman Co., Rochester, NY) were used for all exposures. These were processed using automatic processor. These Conventional Radiographs (CRs) served as the control group and they were labeled as Group 1.
A Canon Power Shot SD500 7.1 megapixel digital camera (Canon, USA) which was in the macro-lens mode was used to capture the images, with a recording image dimension of 2592 × 1944. The distance between the lens of the camera and the radiograph was fixed at 10 cm, by using a tripod. An identical illumination was used throughout, with the radiographs being placed at the same location on the masked light box. These images were transferred directly to a Dell Insipiron 1525 computer laptop with a 15.4′ inch LCD monitor, which was enabled with a screen resolution of 1280 × 800. These unaltered images constituted Group 2 Digitized Images (DIs).
The images were converted into grayscale mode, their brightness and contrast being manipulated in Adobe Photoshop (Ver 7.0, Adobe Systems Incorporated, USA), to form the Group 3, Processed Digitized periapical Images (PDI).
All the images were saved as JPEG maximum quality images and they were viewed at the ratio of 1:2, under the same viewing conditions. However, investigators were provided the option of zooming in on the image whenever it was required.
Two experienced oral radiologists discretely viewed and interpreted CRs and compared them with DI and PDI counterparts, with CRs serving as the control. Visibility and clarity of five parameters – Lamina Dura (LD), Periodontal Ligament Space (PDL), Boundaries of the Periapical Lesion (BA) (if any) and its Internal Architecture (IA) and Periapical Structures (PAS) on the CRs, DIs and PDIs were assessed. A three point grading system was used to grade the DI and PDI images where, 0 was deterioration of image, 1 was no change in image and 2 – was enhanced image, as compared to the CRs. The scores obtained from the individual parameters were summated to obtain an overall score for the image. Paired
t-test and Kappa analysis were used for the statistical analysis (Med Calc Ver 12.0.3.0).
Results
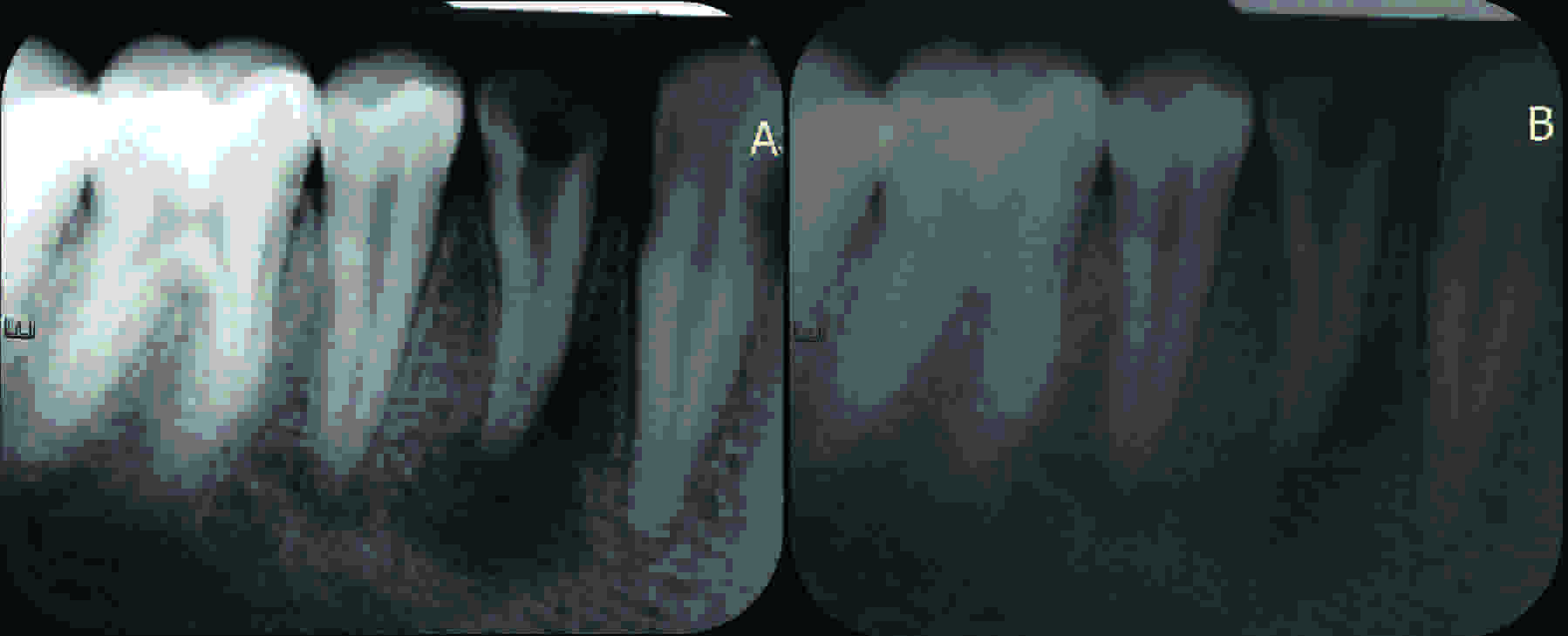
The study involved analyzing radiographs and digitized and processed digitized images for obtaining a perceived clarity of the apical third of root and the periapical structures. On comparison, the PDIs group showed an overall enhancement in image clarity, which not only assisted in a better interpretation of the structures which were studied but also facilitated a better diagnostic assessment [Table/Fig-1]. In contrast, DIs group showed deterioration in the image quality. Paired t test was performed to compare the overall scores of group 1 with those of group 2 and 3 and the results were statistically significant (p < 0.05) [Table/Fig-2]. The overall interobserver variability was rated as good, with kappa values of 0.76 and 0.84 respectively for Groups 1 and 2 [Table/Fig-3].
Comparison of (A) PDI image with (B) DI image
| Investigator 1 | Investigator 2 |
|---|
| Grp 1vs Grp 2 | Grp1 vs Grp3 | Grp 1vs Grp 2 | Grp1 vs Grp3 |
|---|
| Standard deviation | 1.5325 | 2.1647 | 1.6793 | 2.3871 |
| Two-tailed probability | < 0.0001 | 0.0328 | < 0.0001 | 0.0184 |
Interpretation-scores of both the investigators for each parameter, as compared to conventional radiographs, with Kappa analysis
| Investigator | Image quality score | DI | PDI |
|---|
| LD | PDL | BL | IA | PAS | LD | PDL | BL | IA | PAS |
|---|
| One | 1 | 19 | 14 | 9 | 7 | 13 | 21 | 22 | 10 | 10 | 21 |
| 2 | 0 | 0 | 0 | 0 | 0 | 16 | 13 | 8 | 12 | 14 |
| 0 | 23 | 28 | 18 | 19 | 29 | 5 | 7 | 9 | 4 | 7 |
| Two | 1 | 14 | 13 | 10 | 6 | 16 | 23 | 20 | 11 | 11 | 23 |
| 2 | 0 | 0 | 0 | 0 | 0 | 16 | 16 | 9 | 11 | 13 |
| 0 | 28 | 29 | 17 | 20 | 26 | 3 | 6 | 7 | 4 | 6 |
| Kappa | .753 | .647 | .757 | .898 | .738 | .749 | .867 | .868 | .978 | .727 |
Discussion
Digitization, while maintaining the original radiographic information, merely performs conversion of an analog image into a form that can be read and analyzed by the computer. A digital image comprises of pixels (picture elements), with its spatial resolution (size of the pixel) and contrast resolution (number of grey levels) determining the resolution of the digital image. Image processing is indicative of any procedure that works towards improving, restoring and analyzing, or any approach which alters the digital image. Image enhancement implies that the adjusted image is an improved version of the original one [9]. Digitization equips the clinician with an opportunity for image processing with the use of a wide array of tools like image enhancement, density and contrast alteration, gray scale inversion, magnification, pseudocolour, and pseudo 3-D [10,11]. The aim behind image processing is to generate images that enhance the visual perception and make pertinent information more evident. The image characteristics which are usually altered are contrast and density. Contrast can be changed by maneouvering the gradient of the gray levels in the image, whilst density can be changed by adding or deducting the same value to each pixel [10,11]. The same image, therefore may be used for various diagnostic tasks by adjusting the image characteristics; eg: for detection of marginal bone loss, use of a light radiograph is preferred, while for caries detection, an increased contrast image is needed [12]. This procedure thus serves multiple purposes and it also reduces patient radiation exposure and operator labour. However, an image which has a pixel saturation i.e too dark or noise or inadequate subject contrast cannot be salvaged [10,11]. The resolution of the modern digitized images is comparable or it may be even be better than that of film. However, it should be borne in mind that, though an enhancement may make images aesthetically acceptable, it may also cause loss of clinical information and jeopardize the diagnosis [7].
In the present study, investigators appreciated the enhanced appearance of the processed digital images as compared to the other modalities which were studied. This betterment could be attributed to contrast and brightness adjustments which were performed, which aided the investigators in a finer subjective assessment of the structures which were evaluated. Our results are in accordance with those of Prapayasatok and co-investigators who evaluated the diagnostic accuracy of proximal caries detection on digitized film images which were captured by a digital Sony Cyber-shot, DSC-S75 camera at different resolution settings of 640 × 480, 1280 × 960 and 1600 × 1200. The observers were not permitted to use any tools to enhance the images. The study concluded that for proximal caries detection, at the camera resolution of 1280 × 960, the diagnostic accuracy of digital images were comparable with that of conventional films [13].
In contradiction, study of Goga and co-workers which aimed at comparing digital images of conventional radiographs with those of the original radiographs for a perceived clarity of endodontic files, periapical lesions and carious lesions, concluded that use of superior-grade digital cameras or scanners did not produce images of investigative quality and clarity and that diagnostic quality of the conventional radiographs was better than that which digital images produced [8]. Akin to our study, Prapayasatok and co-investigators also disagreed with the results of Goga and opined that their results could have been influenced by the choice of viewing monitors and the way the images were displayed [13].
Studies which were broadly based on identical concepts as ours have shown varied results. A research which compared seven digital cameras for digitizing radiographs, surmised that low-priced digital cameras may not provide diagnostic quality images [14]. Yet another study which evaluated the accuracy of approximal caries diagnosis from digitized radiographs and digitally modified radiographic images, in comparison to conventional radiography, concluded that the hyperbolic logarithmic modification can be an alternative to conventional radiography in incipient approximal caries diagnosis and restorative decision making [15]. A study which compared conventional intra-oral radiographs and scanner digitized equivalents for image density, contrast, and resolution, noted that resolution of both conventional and digitized radiographs was alike [4].
Contradictory views have been expressed on the subject of digitization, with some studies endorsing the effectiveness of digital imaging methods and others preferring direct viewing of the analog radiographs [16–21].
Various studies have supported utilization of digital tools for image enhancement and they have suggested that image treatment options should be presented to the dentists [22–24]. This view was attested by the authors of the present study also. A research paper which examined the achievable resolution after scanner digitization of intra-oral films, determined that film resolution was utilized best through digitization. It also stated that high contrast use of technical aids such as masking, light boxes and magnifiers, the observer’s eyesight and clinical experience are of further importance in analyzing a radiograph [25].
Conditions like room luminance, image compression, monitor luminance and display monitor technologies have also been investigated to ascertain their influence on the interpretation of radiographs and digital images. Some investigators opine that the diagnostic quality would be lower if it was viewed under normal dental surgery lighting and that background lighting hampers grey- scale perception on computer displays, while others advocate that dental practitioners need not alter their usual dental operatory settings [26–28].
Monitor luminance is a critical component in maximizing contrast resolution and the perceived gray scale. It has been opined that both objective and subjective measures of a radiologist’s performance can be improved with optimized levels of monitor brightness [29]. An investigation which compared film, desktop monitor and laptop displays of indirectly digitized film images, concluded that diagnostic accuracy for proximal surface caries detection was similar for all the modalities which were assessed [30]. The interpretations of laser-digitized hand radiographs versus original radiographs in patients with rheumatoid arthritis, reported that the high resolution monitors provided highly reproducible results which were comparable to those which were obtained from the original radiographs [31].
Despite the reported variations in the resolution of digitized images, there seems to be a general consensus that digitizing conventional radiographs provide an opportunity to utilize the image processing tools which may improve the subjective image quality [4].
Conclusion
Although innumerable studies have been conducted, which have analyzed the image characteristics of direct digital and scanner acquired digitized images, those which involved digital cameras are far and few. The attractive qualities of a digital camera, its universal acceptance, ease of use, real time imaging, affordability and its application in telemedicine and radiology, may be some of the reasons for employing digital cameras for digitization.
This investigation revealed that unprocessed digital images were of a poor diagnostic quality. Processing the digitized images resulted in an enhanced image clarity and an improved diagnostic quality. Nevertheless, the authors opine that more research is required, with an increased sample size, to validate and firmly establish the diagnostic competence of indirectly acquired and processed digitized intraoral radiographic images.