Background: Taurodontism is a clinical entity with a morpho–anatomical change in the shape of the tooth, which was thought to be absent in modern man. Taurodontism is mostly observed as an isolated trait or a component of a syndrome. Various techniques have been devised to diagnose taurodontism.
Aim: The aim of this study was to analyze whether a biometric analysis was useful in diagnosing taurodontism, in radiographs which appeared to be normal on cursory observations.
Setting and Design: This study was carried out in our institution by using radiographs which were taken for routine procedures.
Material and Methods: In this retrospective study, panoramic radiographs were obtained from dental records of children who were aged between 9–14 years, who did not have any abnormality on cursory observations. Biometric analyses were carried out on permanent mandibular first molar(s) by using a novel biometric method. The values were tabulated and analysed.
Statistics: Fischer exact probability test, Chi square test and Chi-square test with Yates correction were used for statistical analysis of the data.
Results: Cursory observation did not yield us any case of taurodontism. In contrast, the biometric analysis yielded us a statistically significant number of cases of taurodontism. However, there was no statistically significant difference in the number of cases with taurodontism, which was obtained between the genders and the age group which was considered.
Conclusion: Thus, taurodontism was diagnosed on a biometric analysis, which was otherwise missed on a cursory observation. It is therefore necessary from the clinical point of view, to diagnose even the mildest form of taurodontism by using metric analysis rather than just relying on a visual radiographic assessment, as its occurrence has many clinical implications and a diagnostic importance.
Introduction
Taurodontism is an enlargement of the body and pulp chamber of multirooted teeth, with apical displacement of the pulpal floor and bifurcation of the roots [1]. This term was first coined by Keith in 1913, to describe molars of Neanderthal human fossils, which showed a tendency of the body of the tooth enlarging at the expense of its roots [2–5]. Taurodontism was considered to be typical of Neanderthal man. This anomaly was thought to be absent in modern man. However, an increasing number of reports do suggest that taurodontism is present in the present day man also. The incidence of Taurodontism has been reported to be lower than 1% in modern man and to be 3% in primitives, Eskimos and American Indians [5].
Taurodontism has gained much importance among dental clinicians and anthropologists, who use this trait to determine the evolution of man [2]. Taurodontism can be observed as an isolated trait or a component of a syndrome, which includes Trichodentoosseous syndrome, Klinefelter’s syndrome, Ectodermal dysplasia and Otodental dysplasia. Taurodontism can occur in both the deciduous and permanent dentitions, though it is more common in the permanent dentition [4,6,7]. Hammer proposed that Taurodontism results from failure of the epithelial diaphragm to invaginate at the proper horizontal level. There is no odontoblastic deficiency during dentinogenesis of the roots. However, other possible causes of Taurodontism, which have been proposed by Margion are: a specialized or a retrograde characteristic, a primitive pattern, a Mendelian recessive trait and an atavistic feature [5,6]. Various techniques have been employed by various authors to diagnose taurodontism objectively. Keen, Blumberg, Shiffman and Channel have devised objective methods by using radiographs for diagnosing taurodontism. At present, a visual radiographic assessment is the most followed method of diagnosing taurodontism. By using this method, severe forms of taurodontism can be easily recognized without much difficulty. However, the mildest form of taurodontism goes unnoticed. To overcome this difficulty, we used the biometric analysis to diagnose taurodontism. By using this method, we tried to test the hypothesis that the teeth which apparently appeared normal could actually be having taurodontism in its mildest form, which was not possible to diagnose by using a visual radiographic assessment. The importance of these analyses lies in the fact that taurodontism can be missed on a cursory observation of radiographs, which is a subjective method of analyzing it and is most often used in diagnosing this trait. The diagnosis of taurodontism is not only useful from the clinical point of view, but also in the identification of various pathological states of associated medical conditions or syndromes.
Material and Methods
Panoramic radiographs were retrieved from the past dental records of our institution. The radiographs were chosen in such a way that only those radiographs which did not show any evidence of taurodontism of the permanent first mandibular molar on visual examinations were taken up for the study. We used the biometric method which was propsed by Kim Seow and Lai to measure taurodontism by using panoramic radiographs. A total of 43 cases constituted our study group, of which 31 were females and 12 were males. These were aged between 9-14 years . Only those radiographs were taken, where there was a radiographic evidence of root completion of the permanent mandibular right or left first molar or both, without any evidence of taurodontism on a cursory observation. Permanent mandibular first molars with carious involvements or those with restorations and with orthodontic appliances were excluded from the study. Radiographs of subjects with abnormal oral habits or parafunctional habits, syndromes or developmental anomalies of the tooth which was concerned, were also excluded from this study. Faulty radiographs which obscured or altered the morphology of the teeth were not included in this study.
Radiographic Assessment of Taurodontism
We used the biometric method which was devised by Kim Seow and Lai to measure taurodontism in panoramic radiographs [2]. This method was chosen over other methods, as this method uses standard landmarks on the tooth, that are constant and are not affected by environmental and age related factors. Furthermore, this method is simple, easily reproducible, and less time consuming. The radiographs were first placed on an X–ray viewer. The outline of either the right or left permanent mandibular first molar or both were traced on a tracing paper by using a 0.5 mm lead pencil. The crown – body (CB) to root ratio were determined in each of these cases. Crown- body (CB) length was determined by drawing an occlusal line through the deepest pit, which was parallel to another line which joined the cusp tips. The crown (C) length was measured in a longitudinal axis, from the deepest pit to the cementoenamel junction. The body (B) length was measured from the cementoenamel junction to the bifurcation in a longitudinal axis. These values were added in each of the cases to obtain a crown – body (CB) length. Similarly, the root (R) was measured along the same axis, from the furcation to the apex of the root [Table/Fig-1]. These measurements were made by two independent observers and their values were tabulated. To reduce the inter–observer bias, an average value of the two was deduced.
Traced radiograph (by using lead pencil)
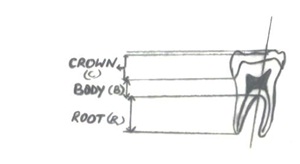
Teeth with a CB: R ratio of <1.10 were considered as normal (Cynodont), those with ratios of between 1.10-1.29 were designated as hypotaurodontic; those with ratios of between 1.30–2.00 were designated as mesotaurodontic and those with values which were > 2.0 were designated as hypertaurodontic.
Statistical Analysis
Fisher exact probability test, Chi–square test and Chi–square test with Yates correction were used for statistical analysis of the data.
Results
Cursory observations of the radiographs by either of the observers did not yield any case of taurodontism. The actual measurement yielded us 8 (18.6%) cases of taurodontism. A Fisher exact probability test which was applied to compare these two proportions yielded a probability of 0.005. (Fisher exact probability, p < 0.005) The difference was statistically significant [Table/Fig-2]. Of the eight, 4 cases exhibited taurodontism of the permanent mandibular left first molar, 6 cases exhibited taurodontism of the permanent mandibular right first molar and 2 cases exhibited taurodontism bilaterally.
On analysing between the genders, the 12 male subjects were found to yield four cases of taurodontism and 31 female subjects yielded 4 cases of taurodontism [Table/Fig-3]. These proportions were tabulated and the Chi square test was applied. The differences between the genders were not statistically significant (Chi-square value of 1.23; p value of 0.26).
Prevalence of taurodontism by the method of analysis
| Method of Observation | Taurodontism Positive | Taurodontism Negative | Total |
|---|
| Cursory observation | 0 (100%) | 43 (100%) | 43 (100%) |
| Biometric analysis | 8 (18.60%) | 35 (81.39%) | 43 (100%) |
* p value < 0.005
A comparative analysis was done for cases whose ages were less than or equal to 12 years and more than 12 years. Apparently, the cases of taurodontism were higher among those who were aged equal or less than 12 years (25%) as compared to those who were aged more than 12 years (6.66%). However the difference was not significant, as the Chi–square test with a Yates correction was only 1.13, with a p value of 0.29 [Table/Fig-4].
The prevalence of taurodontism in both the genders using the biometric analysis
| Gender | Presence of taurodontism | Absence of taurodontism | Total |
|---|
| Males | 4 (33.3%) | 8 (66.6%) | 12 (100%) |
| Females | 4 (12.9%) | 27 (87.09%) | 31 (100%) |
| Total | 8 (18.6%) | 35 (81.39%) | 43 (100%) |
* p value = 0.26
Prevalence of taurodontism in the two age groups using the biometric analysis
| Age | Taurodontism Positive | Taurodontism Negative | Total |
|---|
| Equal or less than 12 years | 7 (25%) | 21 (75%) | 28 (65.11%) |
| More than 12 years | 1(6.66%) | 14 (93.33%) | 15 (34.88%) |
| Total | 8 (18.60%) | 35 (81.39%) | 43 (100%) |
* p value = 0.29
Discussion
Molars in modern humans, for the most part, have long crowns and roots but short bodies. These teeth are called cynodonts. However, there exists an anomaly in which the furcation is displaced apically, this results in elongation of the body and pulp chamber and in shortening of the roots. This condition is called taurodontism. The term Taurodontic (bull tooth) was coined from the latin term, ‘tauros’, which means ‘bull’ and the Greek term, ‘odus’, which means ‘tooth’ [6,8]. This anomaly was first reported in the remnants of prehistoric hominids by de Terra in 1903, by Gorjanovic- Krambeger and Aldoff in 1907 and in 1909, Pickerell noted this anomaly in modern man [3]. A trait which was considered to be typical of Neanderthal man, has now been found even in modern man and it is also associated with several developmental anomalies and syndromes [5]. Identification of this condition can only be made by doing a radiographic examination, as the external morphology of the teeth is within normal configuration. Even on a radiographic examination, the diagnosis of taurodontism is subjective [7].
As observation of radiographs is a subjective analysis, it is an unreliable indicator which can diagnose taurodontism. This subjective analysis which is most often used in clinical practice to diagnose taurodontism, is the one which was given by Shaw in 1928 as hypotaurodontism, mesotaurodontism, hypertaurodontism and it is based on the apical displacement of the pulp chamber floor [2].
In this study, we used the method which was devised by Kim Seow and Lai to assess taurodontism in apparently normal panoramic radiographs [2]. Mandibular molar was chosen for the following reasons: the permanent mandibular first molar is the most stable tooth of the series; hence, any change in the morphology may indicate a true change. Secondly, the entire outline of this tooth is evident clearly on the panoramic radiographs, in contrast to the maxillary molars, where the root apices are usually obscured by the zygomatic bone. Hence, the lengths of the roots can be easily determined. Keen, in his technique, used metric attributes to diagnose taurodontism; however, they were affected by environmental changes and by aging [8]. Our study group was between 9-14 years of age, where there is a radiological evidence of root completion and the process of tooth wear is minimal. Thus, environmental and ageing factors were taken into consideration for our analysis. Similarly, Blumberg, in 1971, improvised Keens’ technique by using measurements which were not influenced by caries, age or sex, but subjective criteria were still considered for the analysis. To overcome this subjective analysis of assessing taurodontism, Shiffman and Channel established an objective method, but this technique, like Keens technique, was affected by environmental and aging factors [8]. In addition to the environmental and age related factors that hampered the assessment of taurodontism, our study also took into consideration other factors that hampered the assessment, and they were excluded.
On visual examination of the panoramic radiographs, neither of the two observers found any evidence of taurodontism in the permanent mandibular first molar. A metric analysis was then carried out on the traced radiographs. The radiographs which were used in this study were orthopantograms (OPGs) which were procured from the past dental records. It is known that a periapical radiograph, on using the parallel cone technique, exhibits minimal distortion. However, a comparative analysis in terms of accuracy of a periapical radiograph above that of an (OPG), did not yield a statistically significant difference between the two techniques, thus validating our use of OPGs for analysis [2]. The value of crown, body and root ratio was deduced and a mean of the values of the two observers was taken, to keep the bias to the minimal. On analyzing the data, 18.6% of these were found to exhibit evidences of taurodontism. The type of taurodontism which was observed in all these cases was hypotaurodontism or the mildest form of taurodontism. Of these cases, only two cases exhibited hypotaurodontism bilaterally. We then extended our study to a comparative analysis in terms of age, sex and sides of the mandibular arch. We observed that hypotaurodontism was seen in both the sexes in the two age groups which were considered [Table/Fig-1 and 2].
Finally, taurodontism, although it is rare, has many clinical implications. Endodontic treatments in taurodontic teeth have been described as complex and difficult. The floor of the pulp chamber is more apically positioned, thus making localisation and instrumentation of the root canal orifices more difficult. When the roots are bifurcated or trifurcated, a pronounced curve is usually present in each of the roots. Gauging the apical curves is essential in such cases. Extractions may be more difficult, as the furcation is located more apically and as the root apices may be shorter and thinner. When as orthodontic treatment is being planned, it must be noted that the anchorage values of taurodontic teeth may be reduced in view of their reduced root surface area. The reduced root support of taurodontic molar teeth may mean that the use of a head gear is contraindicated [4]. In fixed prosthesis therapy, a taurodontic molar may not be considered an an adequate abutment tooth, since its smaller surface area may be less resistant to the lateral displacing forces as compared to that of a cynodont [9]. From a periodontal standpoint, taurodontism may be particularly useful. The chances of a furcation involvement are considerably less in a taurodont tooth than in a normal tooth, as a significant periodontal destruction is essential before a furcation involvement occurs in the former [10]. However, in case of a furcation involvement, the prognoses of such teeth become questionable as compared to those of normal teeth. In a similar condition such as teeth with taurodonts lose more periodontal support than a normal tooth with a furcation involvement [11]. Furthermore, taurodontism should be differentiated from other conditions which exhibit similar features. These include the shell teeth of dentinogenesis imperfecta, which have large pulp chambers which result from the relative absence of dentin. These teeth exhibit a normal furcation but smaller roots. The teeth in regional odontodysplasia, ‘ghost teeth’ characteristically have very thin enamel and dentin and a large pulp chamber. The dental hard tissue exhibits quantitative and structural deficiencies and the teeth usually fail to erupt. In hypophosphatasia, the teeth are hypocalcified and they harbour large pulp chambers. The teeth are lost because of cemental agenesis. Dentin dysplasia type 2 exhibits large flame shaped pulp chambers, especially in premolars. The pulp horns rather than pulp chambers are elongated in hypophosphataemia. Pseudohypoparathyroidism exhibits teeth with enlarged root canals, with lack of an apical closure [9].
Conclusion
Our study was statistically significant in diagnosing taurodontism, in terms of metric analyses on radiographs. A trait which was missed in some of the radiographs on clinical examination, was diagnosed with our study. It is therefore, necessary from a clinical point of view, to diagnose even the mildest form of taurodontism by using metric analysis rather than just relying on a visual radiographic assessment, as its occurrence is a complicating factor for an endodontic treatment and a risk factor for orthodontic therapy. Moreover, it may also be beneficial in the possible identification of other associated medical conditions.
* p value < 0.005
* p value = 0.26
* p value = 0.29
[1]. Seow KM, Taurodontism of the mandibular first permanent molar distinguishes between the trichodentoosseous syndrome and amelogenesisimperfectaClin Genet 1993 43:240-46. [Google Scholar]
[2]. Seow KM, Association of taurodontism with hypodontia: a controlled studyPaediatr dent 1989 3:214-19. [Google Scholar]
[3]. Sathyanarayanan R, Carounanidy U, Taurodontism- review and an endodontic case reportEndodontology13:8-10. [Google Scholar]
[4]. Gill DS, Figueiredo JAP, Tredwin CJ, Naini BF, Taurodontism –a reviewDent Update 2001 36:235-43.(2009) [Google Scholar]
[5]. Bhat SS, Sargod S, Mohammed SV, Taurodontism in deciduous molars- a case reportJ Indian SocPrev Dent 2004 22:193-95. [Google Scholar]
[6]. Bharti R, Chandra A, Tikku AP, Wadhwani KK, Taurodontism an endodontic challenge: a case reportJ Oral Science 2009 51:471-74. [Google Scholar]
[7]. Durr DP, Campos AC, Ayers CS, Clinical significance of taurodontismJADA 1980 100:378-81. [Google Scholar]
[8]. Jafarzadeh H, Azarpazhooh A, Mayhall JT, Taurodontism: a review of the condition and endodontic treatment challengesInt Endod J 2008 41:375-88. [Google Scholar]
[9]. Saini T, Wilson CA, Taurodont molars: review of literature and radiographic featuresThe Saudi Dental Journal 1990 2:68-70. [Google Scholar]
[10]. Manjunatha BS, Suresh KK, Taurodontism–a review on its etiology, prevalence and clinical considerationJ Clin and Exp Dent 2010 2:187-90. [Google Scholar]
[11]. Sanjay K, Shantipriya R, Prasad MGS, Soumya K, Nirjhar B, Sanjivini S, Taurodontism of multiple teeth associated with generalized aggressive periodontitis: a case reportInt J Dent Case Reports 2012 2:11-15. [Google Scholar]