We are reporting a rare case of a schwannoma which originated from the cervical portion of the spinal accessory nerve, which was located in the left posterior triangle of the neck and did not have any neurological deficit, which was diagnosed by the Magnetic Resonance Imaging (MRI) scan and confirmed histopathologically after surgery.
Schwannoma, Accessory nerve, Tumour, Nerve sheath
Introduction
The schwannomas have been referred to as neurilemmomas, neuromas, or neurinomas with an unknown originating cause [1,2]. Schwannomas are uncommon benign nerve sheath tumours that originate from any cranial, peripheral or autonomic nerve of the body, with the exception of the olfactory and the optic nerves [1–3]. Some 25-50% cases of the reported schannomas have a predilection for the head and neck [1,2,4], which pose a diagnostic and a management challenge [2]. The schwannomas which occur in the head and neck region mostly originate from the vagus nerve or from the sympathetic nervous system [4]. They are usually solitary asymptomatic nodule masses which are slow growing in the soft tissue and are painless unless they cause pressure on the adjacent nerves [1], Various preoperative image studies have been used to distinguish their locations and origins [4]. The accepted treatment of Schwannomas is surgical excision and surgical modalities, which preserve the neurological function [1,4].
A total of 28 cases of spinal accessory nerve schwannomas have been reported, among which four were reported in the craniocervical region, which extended from C1 or C2 to the vermis, with only two being located in the cervical region [5,6]. We are reporting here, a rare case of an accessory nerve schwannoma in the cervical region.
Case Report
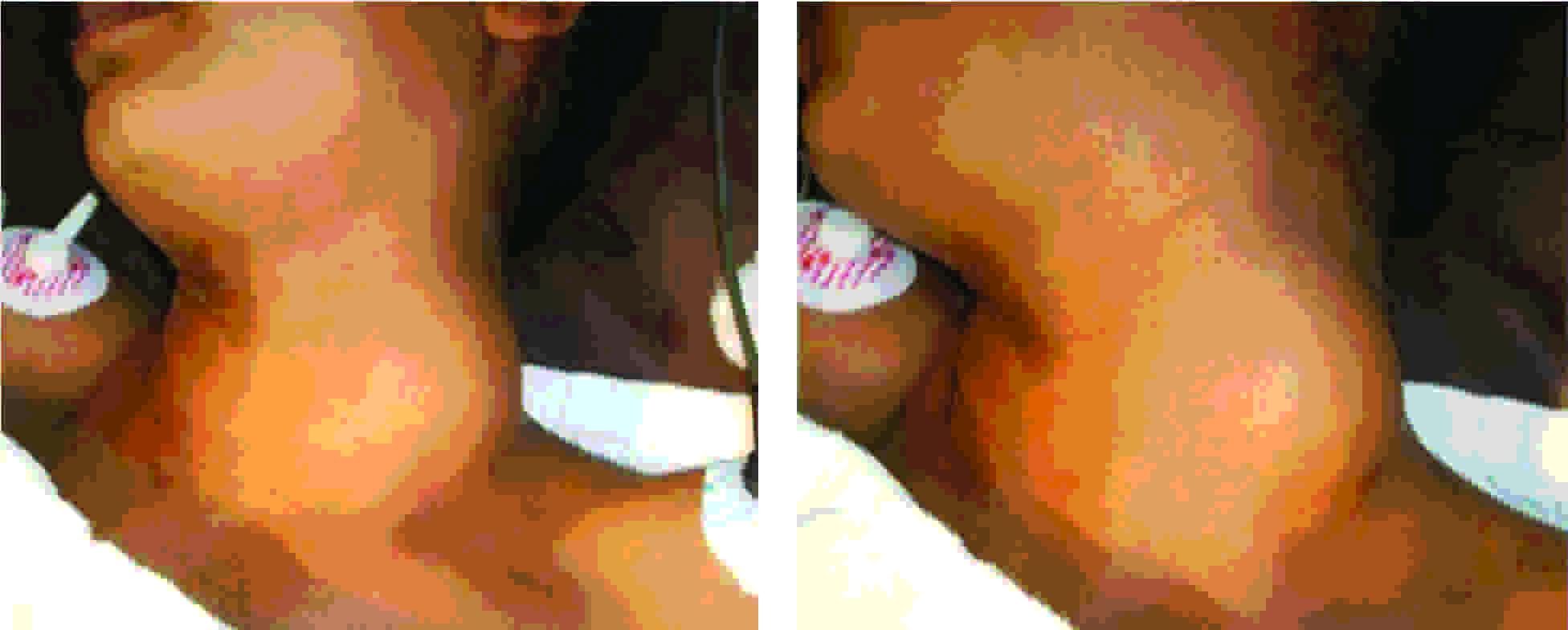
A 17 year old girl presented to the Department of Surgery with the complaint of a painless, slow growing lump on the left side of neck, over a period of 1 year. There was no remarkable personal or family history. The swelling was an oval mass of size, 6 cm by 5 cm, which was located in the posterior triangle of the neck. The swelling was soft, cystic and mobile, with well defined margins and no pressure symptoms. There was no tenderness [Table/Fig-1]. The neurological examinations showed that the neck muscles on both the sides were symmetric. The trapezius and the sternocleido mastoid were similar in power, tone and trophism on both the sides.
Clinical Presentation of patient with Schwannoma
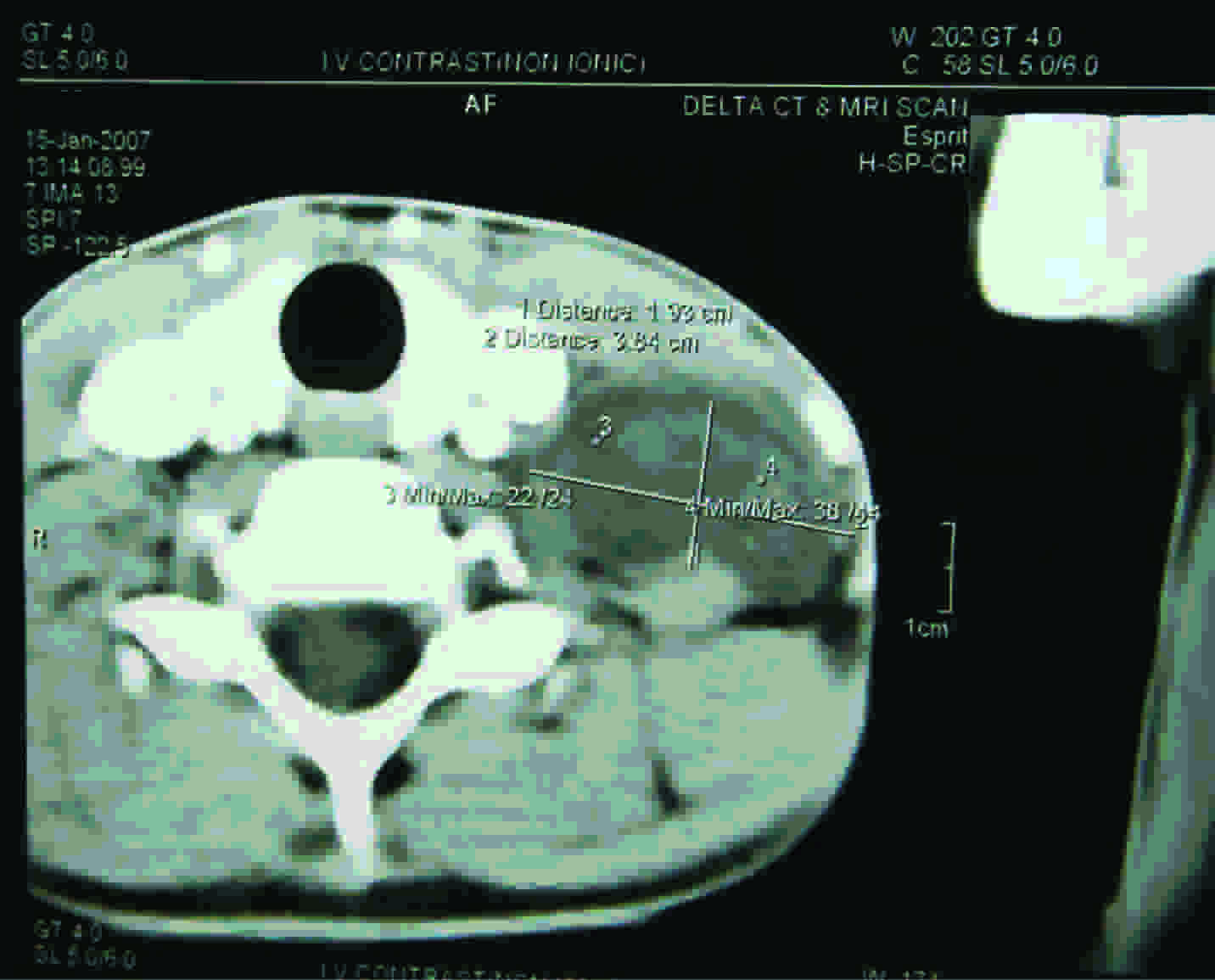
The patient underwent complete blood count and urine culture examinations, which were found to be within normal limits. Ultrasonography was advised to know whether the tumour was located between the jugular vein and the carotid artery. Magnetic Resonance Imaging (MRI) was done with the use of Gadolium based contrast media, for determining the exact nerve of origin [Table/Fig-2].
MRI scan showing the location and dimension of Schwannoma
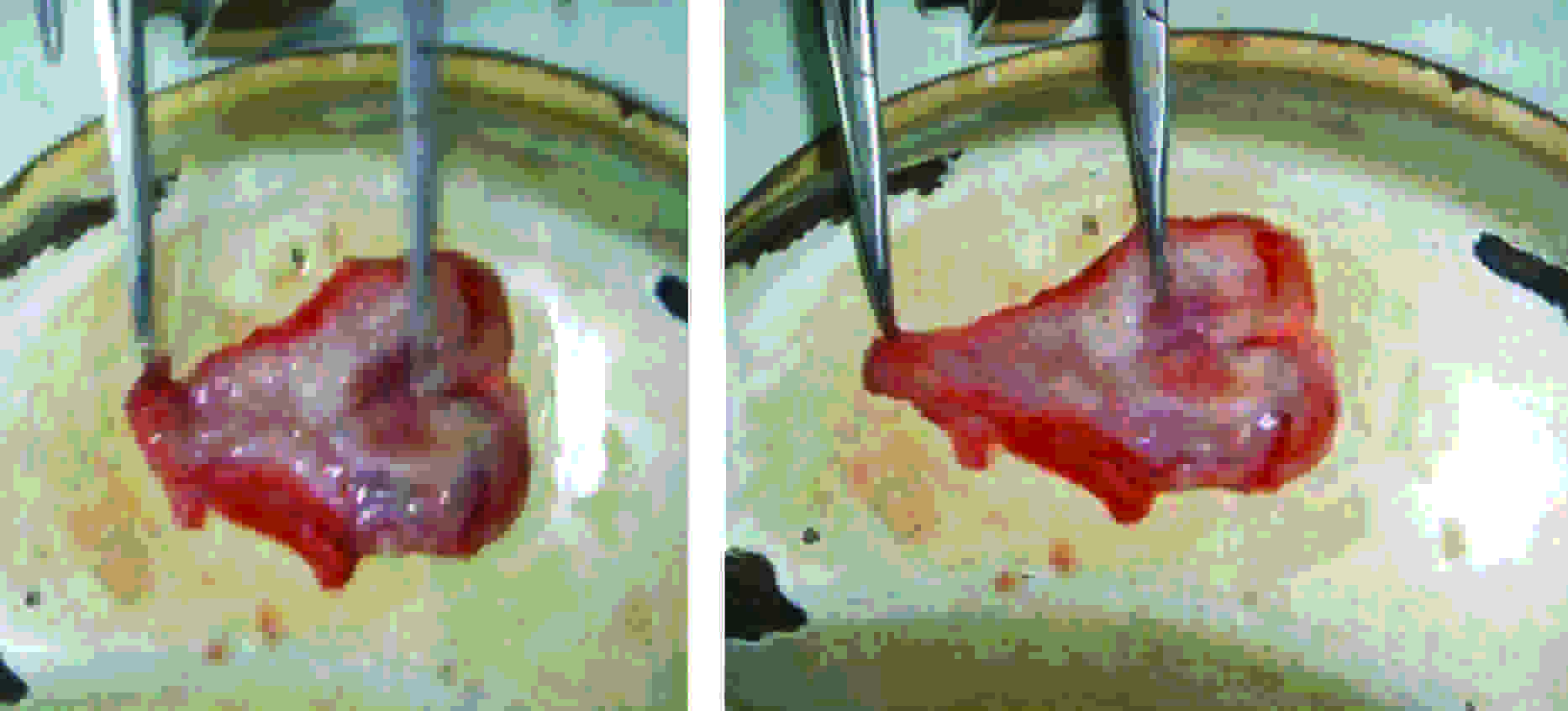
A surgical resection of the tumour was planned under general anaesthesia. The tumour was resected by doing a lateral cervical approach incision. A well circumscribed, encapsulated, yellowish white, shiny mass was found to grow within the substance of the spinal accessory nerve.
The tumour was resected by displacing the uninvolved fascicles which were running between the leaves of the capsule, and not entering the tumour itself. The tumour was extending into the neural canal but it was easily separated by doing a blunt dissection and by applying a mild traction to the tumour. Total excision of the tumour and the entire capsule was done [Table/Fig-3].
Surgical approach to the patient with Schwannoma (Arrow)

The cut section of the tumour demonstrated that it was well encapsulated and gray white on the cut section [Table/Fig-4]. The specimen was sent for a histopathological examination.
Cut section of Schwannoma
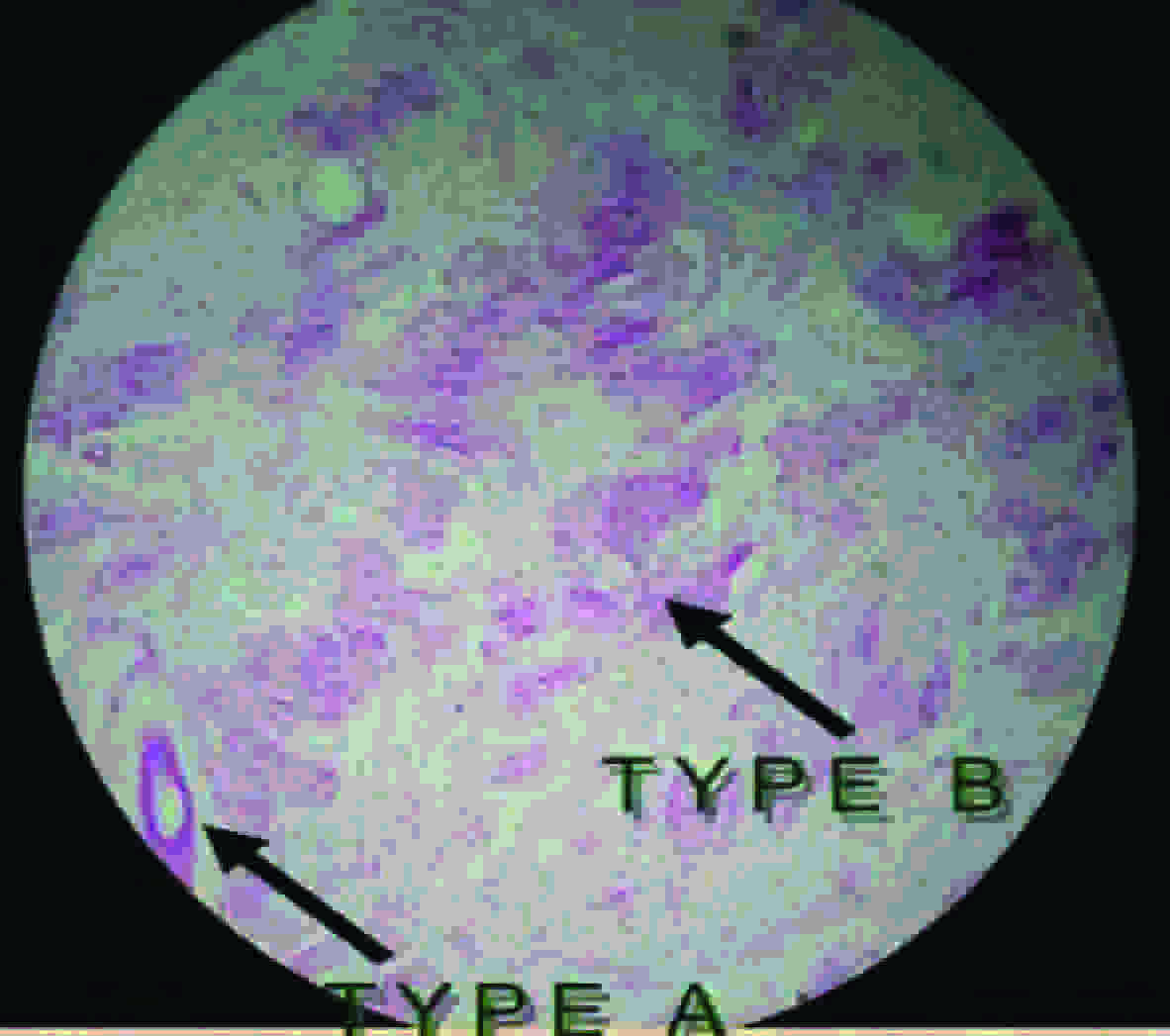
The histopathology demonstrated schwann cells in a collagenous matrix. The Antoni Type A tissue had elongated spindle cells which were arranged in irregular streams and was compact in nature, whereas, the Antoni type B tissue had a looser organization, often with cystic spaces being intermixed within the tissue [Table/Fig-5].
Histopathological section of Schwannoma demonstrating Antoni Type A tissue with elongated spindle cells arranged in irregular streams and compact in nature; and Antoni type B tissue with looser organization, often with a cystic spaces intermixed within tissue
During the postoperative period, the patient developed weakness of the trapezius muscle and was unable to abduct the left arm. The patient was advised physiotherapy and after one month of discharge, the patient was able to abduct her left arm and there was no other neurological deficit .
Discussion
A schwannoma is a relatively slow growing tumour of the nerve sheath, which is composed of the schwann cells, which normally produce the insulating myelin sheath which covers the peripheral nerves. They are homogenous tumours and they always stay on the outside of the nerve and may push the nerve aside or against the bony structure [7].
The schwannomas which occur in the head and neck region mostly originate from the vagus nerve or from the sympathetic nervous system [4]. Most of the cases present with an asymptomatic stable neck mass that causes little concern, other than the possibility of a malignancy and cosmesis [2]. The intracranial accessory nerve schwannomas could be either of the jugular foramen type, the intracisternal type, or of the cervical type. The lower cranial nerves which include the glossopharyngeal nerve, the vagus and the accessory nerve, form a complex at the jugular foramen, which is defined as a jugular foramen schwannoma without the identification of the individual cranial nerve [8].
Imaging studies help in the accurate diagnosis of schwannomas, with a reasonably good accuracy. The modalities like MRI scans are very helpful in identifying the tumours and their correlations with the surrounding vascular structures, muscles, and nerves [4]. In addition, preoperative imaging provides information on the tumour size, location, extent and the surrounding anatomy, and it enables the surgical planning [2].
A gross total resection remains the treatment of choice for these tumours, because they are radio resistant. This tumour is confirmed on the histopathological section, which shows the presence of the Antoni type A and type B cells. The tumour s which originate in the Schwann cells can be detected during immune-histochemical examinations, by virtue of their positive results for the S-100 antigen test [1,5].
The other treatment option is sterotactic radiosurgery (SRS). SRS is gaining popularity, but it depends on many factors, which include the size and the location of the Schwanoma and the age of the patient. Whenever it is possible, SRS should be avoided in young patients [9].
Conclusion
The initial evaluation of the patients with suspected cervical nerve tumours should include the history, clinical assessment, focusing on the stigmata on a family history of neurocutaneous disease and a complete examination of the head and neck, to rule out other neck masses. The primary treatment of the Schwannomas which originate from the cervical portion of the spinal accessory nerve is resection of the total tumour, with sacrifice of the involved nerve. Usually, no postoperative dysfunction of the nerve occurs.
[1]. Chen TW, Chen CJ, Leung KW, Recurrent schwannoma of upper neck: A case reportTaiwan J Oral Maxillofac Surg 2009 20:60-7. [Google Scholar]
[2]. Kang GCW, Soo KC, Lim DTH, Extracranial non-vestibular head and neck schwannoma: A ten year experienceAnn Acad Med Singapore 2007 36:233-40. [Google Scholar]
[3]. Tay HL, Swanston AR, Lumley JSP, Glossopharyngeal schwannoma presenting as gagging dysphagiaPostgrad Med J. 1994 70:207-9. [Google Scholar]
[4]. Kim SH, Kim NH, Kim KR, Lee JH, Choi HS, Schwannoma in head and neck: Preoperative imaging study and intracapsular enucleation for functional nerve preservationYonsei Med J 2010 51:938-42. [Google Scholar]
[5]. Tatebayashi K, Tanaka Y, Numata H, Kawakami S, Kamitani H, Watanbe T, Schwannoma of the spinal accessory nerve in the cistern magnaSurgical Neurology 2003 59:217-22. [Google Scholar]
[6]. Kaynar MY, Hanci M, Sarioglu AC, Intraspinal schwannoma of the accessory nerveBritish Journal of Neurosurgery 1999 13:429-31. [Google Scholar]
[7]. Schwannoma. From Wikipedia, the free encyclopedia. Avaialble at url. http://en.wikipedia.org/wiki/Schwannoma (Accessed on 21st August, 2012) [Google Scholar]
[8]. Julow J, Neurinoma of spinal accessory nerve: Report of two casesActa Neurochir (Wein) 1983 69:219-24. [Google Scholar]
[9]. Jayaraman M, Smirniotopoulos JG, Davis LM, Patel MR, Krasny RM, Imaging in cranial nerve schwannoma. Available at url. http://emedicine.medscape.com/article/336141-overview (Accessed on 21st August, 2012) [Google Scholar]