Cysticercosis is a common problem world wide. However, disseminated cysticercosis is rare. Still rarer is asymptomatic disseminated cysticercosis. We are reporting here a rare case of asymptomatic disseminated cysticercosis which involved brain, face, orbit, lungs, heart, pancreas and spleen in a young Nigerian male, who sought medical attention for dysphagia which was diagnosed as achalasia cardia. Despite widespread dissemination of cysticercosis which involves multiple organs, the individual was asymptomatic for the same. Pancreatic and splenic involvement in disseminated cysticercosis has extremely rarely been reported in literature.
Introduction
Cysticercosis refers to a parasitic infestation which is caused by encysted larval stage of the pork tape worm, Taenia solium. In the life cycle of Taenia solium, humans act as definitive hosts and they harbour the adult forms of the tape worm in their small intestines [1]. Although tape worm infestation is a major and a global public health problem, disseminated cysticercosis is a rare clinical entity with around 50 cases being reported so far [2]. Various authors have reported disseminated cysticercosis which involved central nervous system, striated muscles, sub-cutaneous tissues, orbits, lungs and heart [2–8]. We are reporting here a very rare case of disseminated cysticercosis which involved brain, lungs, heart, orbit, face, pancreas, kidney and spleen in a young male who sought medical attention for progressive dysphagia, which was later diagnosed as achalasia cardia.
Case Report
A 27-years old Nigerian male presented with the chief complaint of dysphagia which had two year’s duration. The dysphagia was initially to solids, which further progressed to liquids as well. An upper GI endoscopy which was done in Nigeria revealed a distal oesophageal stricture, with no evidence of a growth. The patient subsequently came to India for further treatment.
On general clinical examination, he was found to be a well nourished individual. His vital parameters were all within normal limits. Multiple subcutaneous nodules (10-15mm) were detected all over his body. On examination of his respiratory system, bilateral basal crepitations were heard. Rest of the clinical examination was within normal limits. Routine haematological and biochemical parameters were within normal limits. His HIV ELISA test was negative.
He underwent a plain CT scan, followed by a contrast enhanced CT scan of the chest in a 64 slice multi-detector row CT scanner (GE Healthcare, Milwaukee, WI, USA). The CT scan study revealed a moderately dilated oesophagus with an air fluid level within it. The distal oesophagus showed smooth luminal narrowing, with a thin stream of orally administered contrast, which was noted to pass into the stomach [Table/Fig-1], which was consistent with a diagnosis of achalasia cardia. The same was also confirmed on a conventional barium swallow study. Besides, there were multiple, discrete parenchymal nodules (maximum size: 10mm) which were distributed randomly in both lung fields [Table/Fig-2]. On soft tissue window setting, most of these nodules showed presence of central fluid attenuation (HU=6 to 10) with an eccentric hyperdense (HU=45 to 55) focus which was consistent with a diagnosis of cysticercosis [Table/Fig-3]. Similar fluid attenuating nodular lesions were noted in the visualized thoracic and abdominal walls. On a closer look, at least one such lesion was also noted in the musculature of the interventricular septum [Table/Fig-4]. The visualized upper abdomen revealed presence of similar lesions within the pancreas, spleen and possibly, in upper pole of right kidney [Table/Fig-5 and 6]. In view of these findings, NCCT, followed CECT of the head were carried out, although he did not give any past history of seizures. Findings of CT scan of head were consistent with a diagnosis of neurocysticercosis which was in vesicular stage [Table/Fig-7]. In addition, similar lesions were noted in and around the orbit as well as in facial muscles [Table/Fig-8]. Based on the CT scan findings, a diagnosis of achalasia cardia with an incidentally detected (asymptomatic) Disseminated Cysticercosis (DCC) was made. Later, he was found to be positive for anticysticercal antibodies by ELISA .
CT scan of thorax and upper abdomen (thick coronal reconstruction) demonstrates dilated contrast filled distal esophagus with smooth tapering at the gastroesophageal junction consistent with a diagnosis of achalasia cardia

Axial (a) and coronal (b) sections of the thorax (Lung window) demonstrate multiple, discrete parenchymal nodules (maximum size: 10mm) distributed randomly in both lung fields
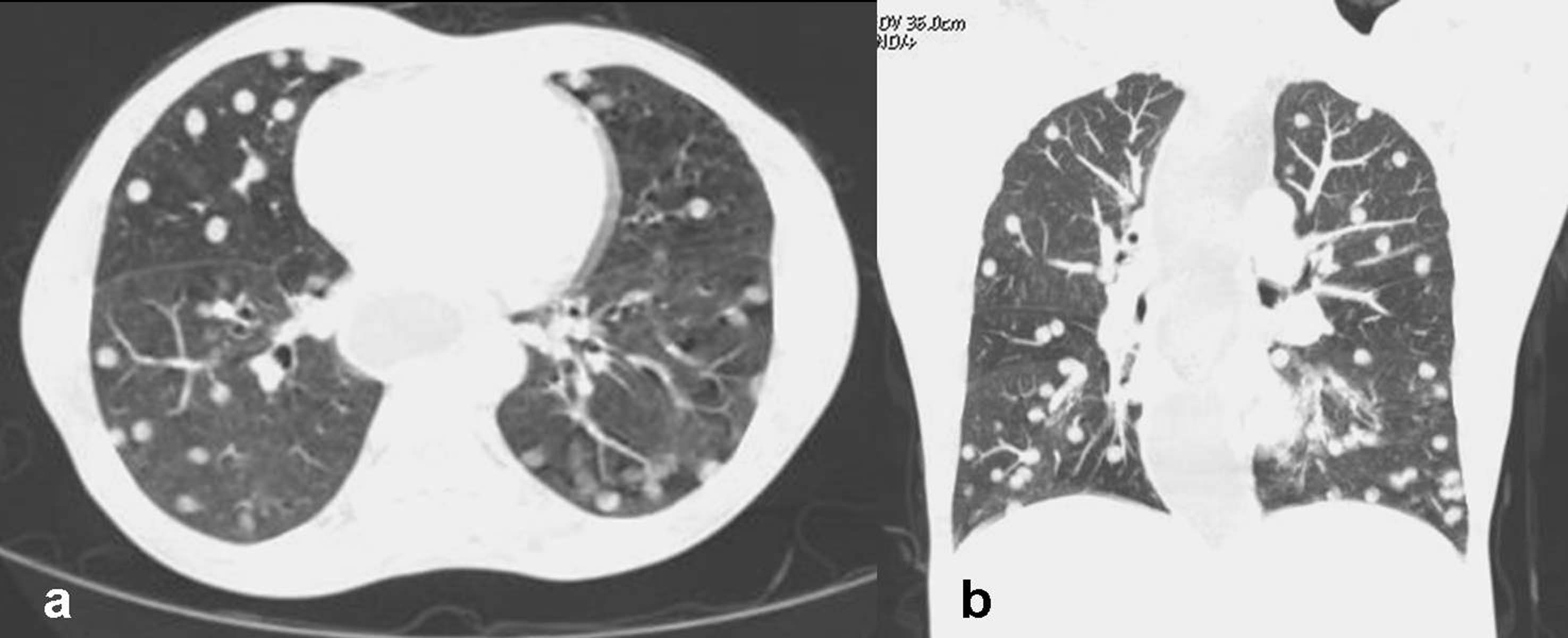
Axial section (Soft tissue window) demonstrates multiple small lung nodules with most of them having central fluid attenuation and peripheral eccentric hyperdense focus (single white arrow). Also note similar lesions in the chest wall (black arrow)

Axial section (magnified) demonstrates cysticercus lesion in the interventricular septum (single white arrow). Also note dilated distal esophagus with air fluid level (double white arrow)

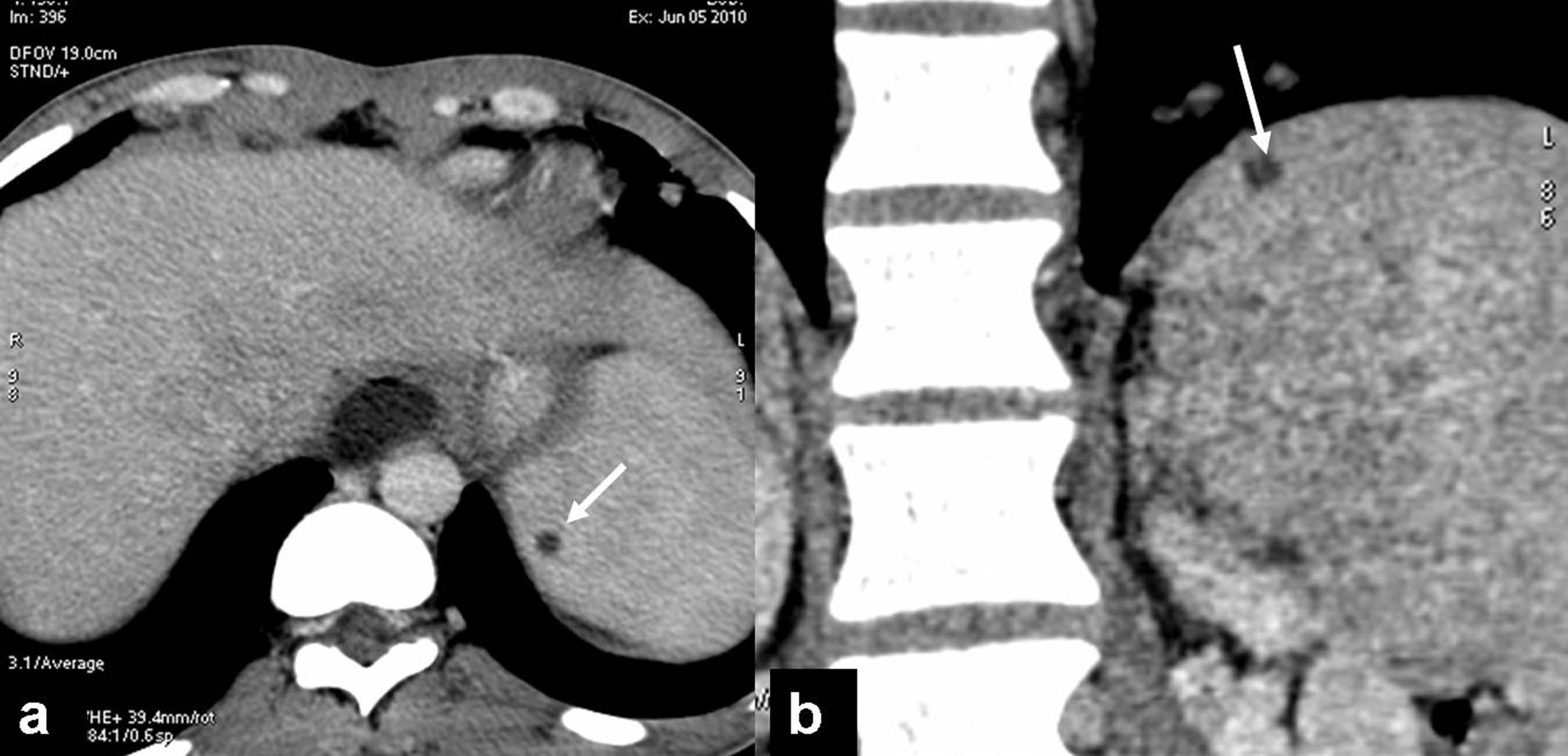
Axial section through upper abdomen demonstrates cysticercus lesion in the mid body of pancreas (single white arrow) and also possibly in the anterior aspect of the right kidney (double white arrow).

Axial section (a) and coronal reconstruction (b) demonstrating cysticercus lesion within splenic parenchyma
Contrast enhanced CT scan brain: demonstrates multiple cysts with most of them having eccentric mural hyperdense focus suggestive of neurocysticercosis (vesicular stage). Note absence of perilesional edema or contrast enhancement

Axial (a) section through the orbit demonstrates presence of cysticerci in the muscles of face (white arrow) and neck (black arrow). Sagittal section through orbit (b) shows presence of cysticercus lesion in the upper eye lid and in the inferior aspect of orbit (white arrow)

He underwent cardiomyotomy for achalasia cardia through the abdominal route. During the immediate post-operative period, he was on prophylactic antibiotics, analgesics and proton pump inhibitors (pantoprazole). He had an uneventful post-operative recovery. Although he was asymptomatic for DCC, he was treated with oral albendazole under supervision. A neurological consultation was sought and he was put on antiepileptic medication. A post- operative follow up CT oesophago-gastrography revealed good contrast opacification of the oesophagus, GE junction and stomach, with no evidence of any extra-luminal tracking or pooling of contrast. The patient was briefed about the status of DCC and he was subsequently discharged from the hospital with an advice of periodic follow ups.
Discussion
Cysticercosis has been known since ancient times. This disease was noted in human beings as early as 1550 [9]. Even today, cysticercosis is a common public health problem worldwide, especially in developing countries, which include India. The disease which was once thought to be confined to the developing countries, is increasingly being recognized in the industrialized countries as well, because of immigration across the globe. The prevalence of the taeniasis varies from place to place, depending on certain factors like geography, ethnicity, religious rituals, income, food habits, personal hygiene, level of education and overall standards of living. There are great variations in the reported incidence and prevalence of taeniasis in the Indian subcontinent [9].
Although cysticercosis is quite common, DCC with multiple organ involvement is rather rare. So far, around fifty cases have been documented in the English literature. Clinical features of DCC depends on the localization of the cysts, parasite burden and host parasite interaction. The central nervous system is most commonly involved in DCC, followed by striated muscles, sub-cutaneous tissues and orbits and accordingly, the most common presenting feature is recurrent episodes of seizure in a case of Neuro Cysticercosis (NCC). Other features of NCC include headache, chronic meningitis, focal neurological deficits, psychological disturbances, dementia, etc [9]. Orbital cysticercosis may present as proptosis, diplopia and even loss of vision. Cardiac and pulmonary involvements are frequently asymptomatic [8] and they may be detected as an incidental finding during imaging workups. Involvement of sub-cutaneous tissues often manifests as palpable subcutaneous nodules. Diffuse muscular involvement can manifest as myalgia, weakness or pseudohypertrophy [6,9].
With the advent of imaging modalities like high resolution ultrasonography, CT scan and MRI, there has been a substantial increase in the detection rate of cysticercosis [10]. Neurocysticercosis (NCC) is now considered as the single most common cause for seizure in the developing countries [11]. Bhalla et al., [2] described a case of DCC which involved brain, sub-cutaneous tissues, skeletal muscles, right orbit and thyroid gland in a patient who presented with generalized tonic clonic seizure. Recently, Atin Kumar et al., [3] reported a paediatric symptomatic case of extensively disseminated cysticercosis which involved virtually entire striated muscular system, sub-cutaneous tissues, paraspinous region, lungs, tongue and parotid glands, which was diagnosed on the basis of whole body MRI with parallel imaging. Pulmonary and cardiac cysticercosis is extremely rare, with only few cases having been reported in the English literature. Bastos et al., [5] described a case of DCC with pulmonary and cardiac involvement, which was demonstrated in a helical CT scan. With increasing use of high resolution ultrasonography, CT scan and whole body MRI, more and more cases of DCC are expected to be encountered in day to day clinical practice. As was illustrated by Atin et al., [3] whole body MRI can help in arriving at a confident diagnosis of DCC, in evaluating the organs which are affected, in estimating the para-site burden and even in demonstrating the various evolutionary stages of the cysticerci. In general, MRI is known for its excellent soft tissue resolution. Moreover, unlike CT scan, MRI does not have any ionizing radiation hazards, thus making it as the most suitable and stand alone imaging modality for the comprehensive diagnosis of DCC.
Our case was unique in several aspects. Firstly, despite involvement of multiple organ systems which included the central nervous system, our patient was asymptomatic, as far as DCC was concerned. Diagnosis of DCC was made while the patient was being investigated for dysphagia, which later on, was found to be caused by achalasia cardia. Secondly, pancreatic, renal and splenic involvements in DCC, as were observed in our case, have only been described extremely rarely in the literature [12].
[1]. Baily GG, Cysticercosis. In: Cook GC, Zumla A, editorsManson’s Tropical Disease 2003 21st edLondonWB Saunders:1584-95. [Google Scholar]
[2]. Bhalla A, Sood A, Sachdev A, Varma V, Disseminated cysticercosis: a case report and review of the literatureJ Med Case Reports 2008 2:137 [Google Scholar]
[3]. Kumar A, Goenka AH, Choudhary A, Sahu JK, Gulati S, Disseminated cysticercosis in a child: whole-body MR diagnosis with the use of parallel imagingPediatr Radiol 2010 40:223-27. [Google Scholar]
[4]. Kadhiravan T, Soneja M, Hari S, Sharma SK, Images in clinical tropical medicine: disseminated cysticercosisAm J Trop Med Hyg 200 80:699 [Google Scholar]
[5]. Bastos AL, Marchiori E, Gasparetto EL, Andrade BH, Junior GC, Pulmonary and cardiac cysticercosis: helical CT findingsBr J Radiol 2007 80(951):e58-60. [Google Scholar]
[6]. Bandyopadhyay D, Sen S, Disseminated cysticercosis with huge muscle hypertrophyIndian J Dermatol 2009 54(1):49-51. [Google Scholar]
[7]. Chadha V, Pandey PK, Chauhan D, Das S, Simultaneous intra-ocular and bilateral extra-ocular muscle involvement in a case of disseminated cysticercosisInt Ophthalmol 2005 26:35-37. [Google Scholar]
[8]. Sousa Ade Q, Solon FR, Da Costa Filho JE, Lima FH, Disseminated cysticercosis with asymptomatic involvement of the heartBraz J Infect Dis 2006 10:65 [Google Scholar]
[9]. Prasad KN, Prasad A, Verma A, Singh AK, Human cysticercosis and Indian scenario: a reviewJ. Biosci 2008 33:571-82. [Google Scholar]
[10]. Rajshekhar V, Raghava MV, Prabhakaran V, Oommen A, Muliyil J, Active epilepsy as an index of burden of neurocysticercosis in Vellore district, IndiaNeurology 2006 67:2135-39. [Google Scholar]
[11]. García HH, Del Brutto OH, Imaging findings in neurocysticercosisActa Trop 2003 87:71-78. [Google Scholar]
[12]. Jakhere SG, Chemburkar VC, Yeragi BS, Bharambay HV, Imaging findings of disseminated cysticercosis with unusual involvement of spleen and pancreasJ Glob Infect Dis 2011 Jul 3(3):306-8.doi: 10.4103/0974-777X.83547 [Google Scholar]