Primary Osteosarcoma of Breast, A Rare Case.
Soumit Dey1, Mrinal K. Chaudhury2, Samar K. Basu3, Asim K. Manna4, Subir K. Dutta5
1 Demonstrator, N R S Medical College, Kolkata, India
2 Retired Professor and Chief, Department of Pathology (Histopathology), Scientific Clinical Research Laboratory Pvt Ltd, 2 Ram Chandra Das Row, Kolkata-700013, West Bengal, India.
3 Pathologist, Department of Pathology (Histopathology), Scientific Clinical Research Laboratory Pvt Ltd, 2 Ram Chandra Das Row, Kolkata-700013, West Bengal, India.
4 Pathologist, Department of Pathology (Histopathology), Scientific Clinical Research Laboratory Pvt Ltd, 2 Ram Chandra Das Row, Kolkata-700013, West Bengal, India.
5 Pathologist, Department of Pathology (Histopathology), Scientific Clinical Research Laboratory Pvt Ltd, 2 Ram Chandra Das Row, Kolkata-700013, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORESPONDING AUTHOR: Dr. Soumit Dey, 69E Mansatala Lane, Kidderpore, Kolkata-700023, India.
Phone: 8902159266,
E-mail: drsoumitdey@gmail.com
Mammary sarcomas are very uncommon and make up less than 1% of all primary breast malignancies.Primary osteosarcoma of the breast is extremely rare and represents 12.5% of mammary sarcomas. A secondary lesion from a primary osteosarcoma of the bone should be considered in the differential diagnosis. In addition, the absence of a direct connection between the tumour and the underlying skeleton is mandatory for the diagnosis.We report a case of primary osteosarcoma of the breast occurring in young patient with fatal evolution.
Osteosarcoma of breast, Stromal sarcoma
Introduction
Primary osteosarcoma of the breast is a very rare and an aggressive entity, which is histologically indistinguishable from the conventional osteosarcomas of the bone and other extra skeletal [1] ones. In this report, we have described a case with this uncommon tumour.
Case Report
A 40-years-old woman presented with a mass which arose in the left breast without any pain, which was noticed two months back.
Examination and Investigation: The physical examination at admission revealed a mobile mass in her left breast. The mass was not attached to the sternum or the underlying rib. No axillary lymphadenopathy was detected on the physical examination. The rest of the breast was unremarkable. On mammography, the mass was found to be well demarcated and partially calcified. Liver echography, chest radiography and bone scan were normal. The patient underwent a simple mastectomy.
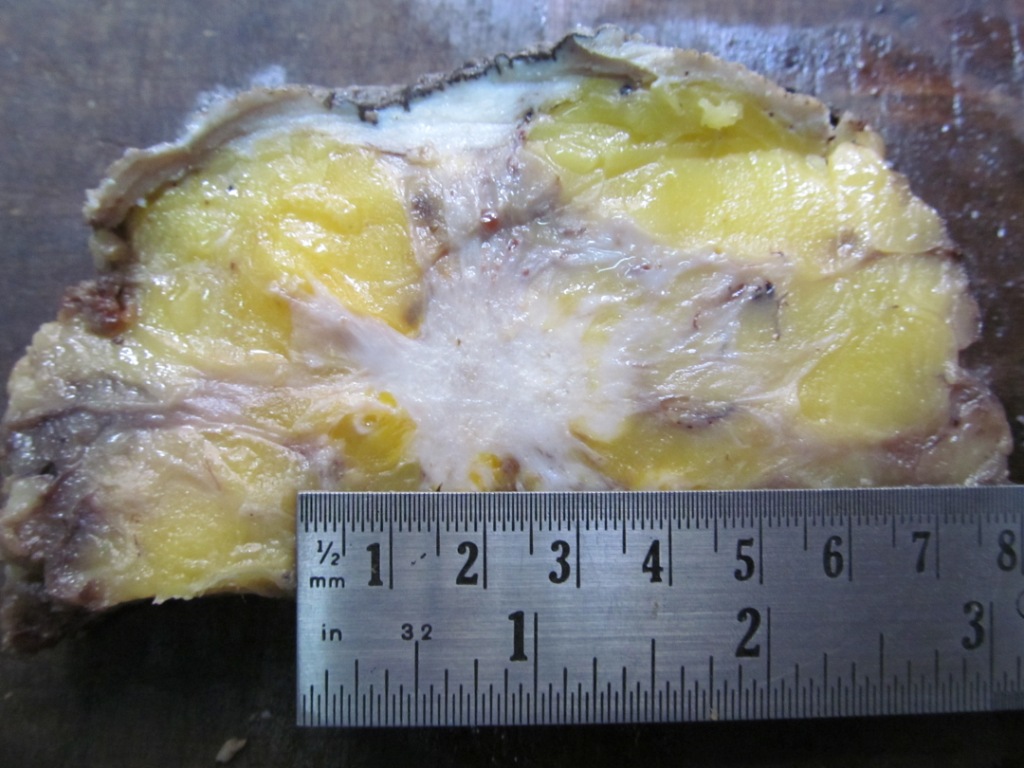
Histopathology: The gross examination of the specimen showed a firm mass with a variegated appearance, which measured 4cm x 3cm in the upper and the lateral quadrants of the breast and it was 1cm away from the deeper resection margin [Table/Figy-1].
Photograph of gross specimen showing a firm mass with a variegated appearance measuring 4cm x 3cm in the upper and lateral quadrant of breast.
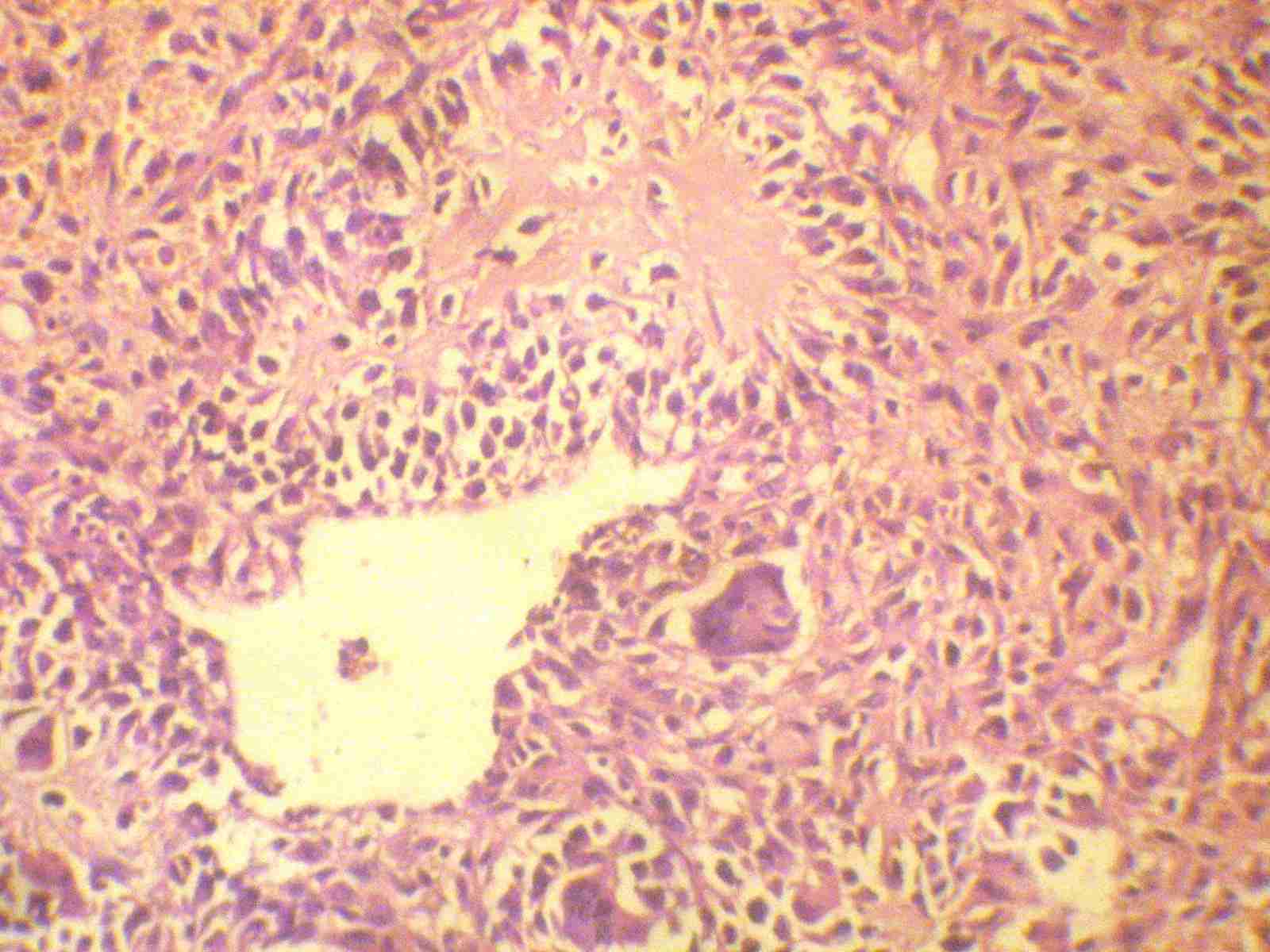
The histological examination revealed abundant osteoid formation, areas of calcification and oval to spindle shaped moderately pleomorphic stromal cells. There were scattered multinucleated osteoclastic tumour giant cells [Table/Fig-2], H and E, X400. Multiple sections were taken to detect an epithelial component if any, thus ruling out the possibility of a carcinosarcoma.
Photomicrograph showing abundant osteoid formation, oval to spindle shaped moderately pleomorphic neoplastic cells and multinucleated osteoclastic tumour giant cells
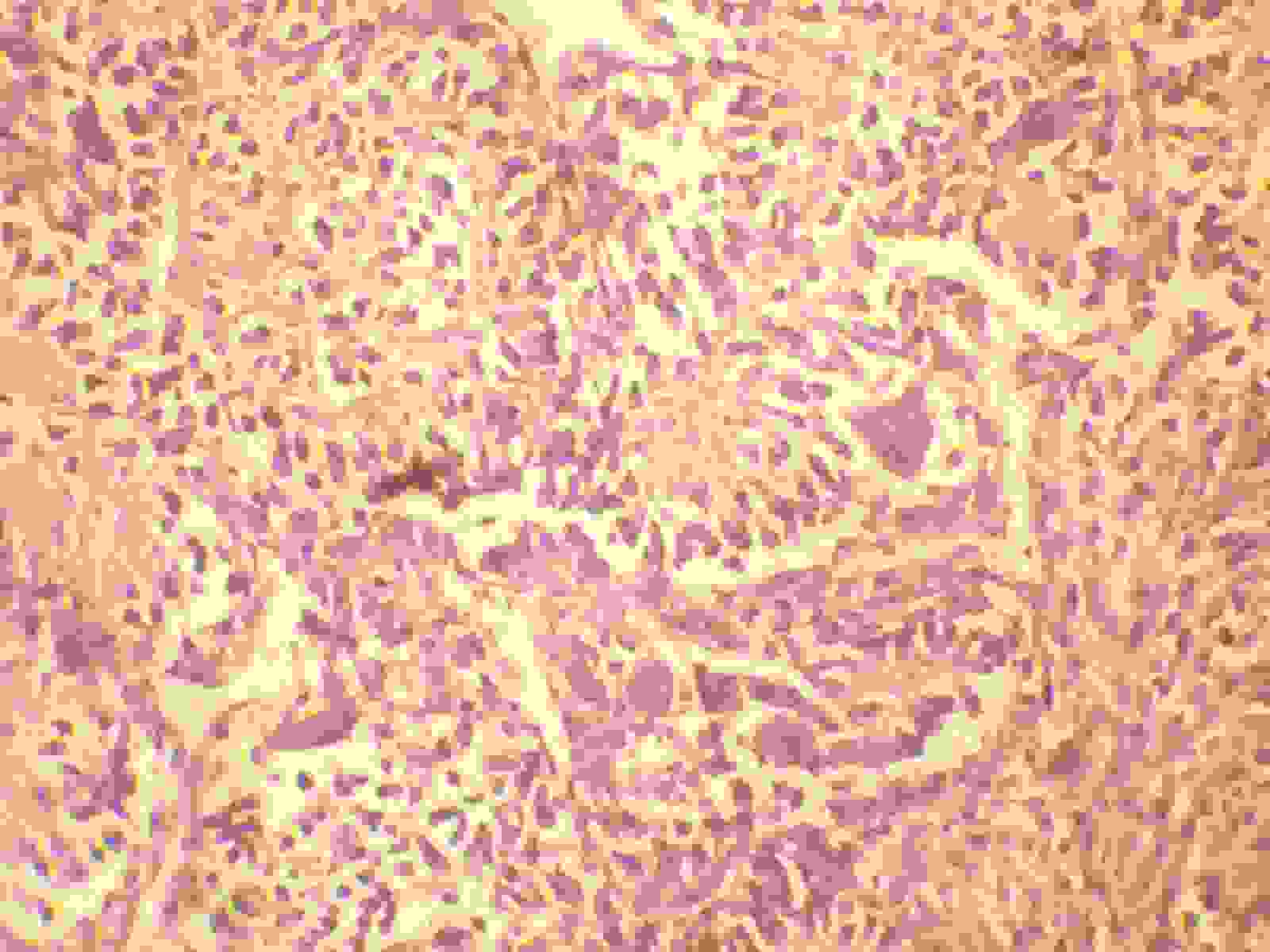
Photomicrograph showing lacy eosinophilic osteoid and osteoclastictumour giant cells
Immunohistochemistry: An immunoreactivity was detected for vimentine but not for for AE1/AE3, CK7, CK20 and the oestrogen and the progesterone receptors. There was also no over expression of the HER-2/neu oncoprotein.
Discussion
The mammary sarcomas are very uncommon and they make up less than 1% of all the primary breast malignancies [1–3]. Angiosarcomas are rare, but they are the most common pure malignant stromal tumours of the breast. Primary osteosarcomas of the breast are extremely rare and they represent 12.5% of all the mammary sarcomas [1]. The rarity of this case prompted us to publish this case report. The histogenesis of primary osteosarcoma of the breast is not clear, but an origin from the totipotent mesenchymal cells of the breast stroma or a transformation from a pre-existing fibroadenoma or a phyllodes tumour has been suggested [2–4]. Primary breast osteosarcomas behave as highly aggressive tumours which are associated with an early recurrence and a tendency for spread via blood rather than through the lymphatics, commonly to the lungs [1,2].
Mammographically, these tumours often present as well circumscribed, dense lesions within the breast parenchyma, with focal or extensive coarse calcifications [1,5]. Osteosarcoma of the breast, presents as fibroblastic, osteoblastic, osteoclastic (giant cell-rich) and fibroblastic subtypes [4–6], as may be seen in its common bony counterpart. Most of the cases of undifferentiated saromas of the breast, after an extensive sampling, may show a focal neoplastic epithelial differentiation, and may thus be regarded as metaplastic carcinomas. The diagnosis of a metaplastic mammary carcinoma should be excluded before a primary breast osteosarcoma is diagnosed. The term, ‘sarcomatoid carcinoma’ has been adapted to reflect the appearance of a mesenchymal neoplasm in these epithelial malignancies. The term, ‘carcinosarcoma’ is usually used to describe the biphasic tumours which are composed of distinguishable malignant epithelial and sarcomatoid components with heterologous elements [4,5].
A secondary lesion from a primary osteosarcoma of the bone should be considered in the differential diagnosis. In addition, the diagnosis of a primary breast osteosarcoma, which is similar to those of other extra skeletal tumours, requires the absence of a direct connection between the tumour and the underlying skeleton [7,8]. In similarity to the above observation, no connetion was noted with the overlying bony ribs in this case.
The first report of a malignant mammary neoplasm of the bone and cartilage was made by Bonet [9] in 1700. Jernstorm [10] observed one osteosarcoma among 3319 cases of mammary carcinomas within a period of 18 years.
The treatment for the localized disease should include a complete surgical removal of the tumour with an adequate margin. An axillary lymph node dissection is essentially not indicated because an axillary node involvement is exceptional [11,12]. Sarcomatoid carcinomas, in contrast, often require axillary node dissections, as do primary breast carcinomas. In a recent report, however, Carter et al., raised the question of benefit from an axillary dissection in the absence of adenopathy, in a subset of a metaplastic carcinoma with a predominant spindle component, given the rarity of the lymph node metastasis in their 29 cases [13]. Although an adjuvant combination chemotherapy has dramatically increased the survival of the patients with primary osteosarcomas of the bone, the responses of osteosarcomas of the breast are still unclear because of the limited data.
Conlusion
The awareness of this rare case and a proper doumentation with a systematic follow up, shall in future, lead to the development of an appropriate management for such cases.
[1]. Bahrami A, Resetkova E, Ro JY, Ibañez JD, Ayala AG, Primary osteosarcoma of the breast: report of 2 casesArch Pathol Lab Med 2007 131:792-95. [Google Scholar]
[2]. Remadi S, Doussis-Anagnostopoulu I, Mac GW, Primary osteosarcoma of the breastPathol Res Pract 1995 191:471-74. [Google Scholar]
[3]. Going JJ, Lumsden AB, Anderson TJ, A classical osteogenic sarcoma of the breast: histology, immunohistochemistry and ultrastructureHistopathology 1986 10:631-41. [Google Scholar]
[4]. Silver SA, Tavassoli FA, Primary osteogenic sarcoma of the breast: a clinicopathologic analysis of 50 casesAm J Surg Pathol 1998 22:925-33. [Google Scholar]
[5]. Ribeiro-Silva A, Zambelli Ramalho LN, Zucoloto S, Phyllodes tumour with osteosarcomatous differentiation: a comparative immunohistochemical study between epithelial and mesenchymal cellsTumori 2006 92:340-46. [Google Scholar]
[6]. Brustugun OT, Reed W, Poulsen JP, Bruland OS, Primary osteosarcoma of the breastActa Oncol 2005 44:767-70. [Google Scholar]
[7]. Momoi H, Wada Y, Sarumaru S, Tamaki N, Gomi T, Primary osteosarcoma of the breastBreast Cancer 2004 11:396-400. [Google Scholar]
[8]. Ellmann A, Jawa ZM, Maharaj M, Primary osteogenic sarcoma of the breast detected on skeletal scintigraphyClin Nucl Med 2006 31:474-75. [Google Scholar]
[9]. Norns HJ, Taylor HB, Sarcoma and mesenchymal tumour of breastCancer 1968 22:22-28. [Google Scholar]
[10]. Jernstrom P, Kindberg AI, Meland ON, Osteosarcoma of mammary glandAm J Clin Pathol 1963 40:521 [Google Scholar]
[11]. Barnes L, Pietruszka M, Sarcomas of the breast: a clinicopathologic analysis of ten casesCancer 1977 40:1577-85. [Google Scholar]
[12]. Ciatto S, Bonardi R, Cataliotti L, Cardona G, Sarcomas of the breast: a multicenter series of 70 casesNeoplasma 1992 39:375-79. [Google Scholar]
[13]. Carter MR, Hornick JL, Lester S, Fletcher CD, Spindle cell (sarcomatoid) carcinoma of the breast: a clinicopathologic and immunohistochemical analysis of 29 casesAm J Surg Pathol 2006 30:300-09. [Google Scholar]