Intra–articular synovial lipomas are very rare and only few cases have been reported till now. We are reporting a rare case of a unilateral intra–articular lipoma of osteoarthritic knee joint in a 62 years old male. Patient had two episodes of sudden locking of knee joint, which resolved spontaneously. A plain X-ray showed changes which were suggestive of osteoarthritis. Clinically, patient was diagnosed as a case of loose bodies in left knee joint. An arthrotomy was performed. After a Histopathological Examination (HPE) of loose bodies, a diagnosis of an intra–articular synovial lipoma was made. Due to wide differentials and varied clinical behaviour of loose bodies, lipoma should be included in differential diagnosis of osteroarthritic patients who complain of episodic locking of knees. Intraarticular lipomas, on arthroscopic guided excision, get cured permanently, with no recurrence. The differentiation of an intra-articular lipoma from a relatively more common entity, Lipoma arborescens, has also been discussed.
Synovial lipoma, Loose bodies, Lipoma arborescens
Introduction
Lipoma is a frequent, benign tumour of the soft tissue. True intra-articular lipomas are extremely rare. Very few cases have been reported till now, with knee joint being the most common site which was involved [1,2]. Clinically, intra-articular lipomas mostly manifest as pressure symptoms which are caused by mass lesions, rarely with knee locking and pain which are caused by loose bodies or joint mice. Occasionally, Liposarcomas which arise as secondary malignancies in settings of synovial lipomas, have also been reported in the literature [3]. An intra-articular synovial lipoma should be considered in the differential diagnosis of loose bodies, when patients complain of sudden knee pain, and brief episodes of catching or locking knees.
Case History
A 62-years old male presented with knee pain and a progressive difficulty in walking which he had since two years. He was diagnosed as case of osteoarthritis and was on irregular medications. Recently, patient had suffered from two episodes of sudden pain with locking of knee, which had remained for 2-3 days and had resolved spontaneously. On examination, left knee was found to be swollen and non–tender and overlying skin was not warm. ESR was raised to 50 mm in 1st hour. Serum uric acid and serum calcium levels were within normal limits. There was no history or clinico -pathological findings which were suggestive of tuberculosis or trauma. RA factor was negative. Synovial fluid aspiration smears were non–haemorrhagic and non–inflammatory and they did not reveal any organism on microbiological examination. X-ray findings were indicative of nonspecific changes of osteoarthritis. A soft tissue shadow which measured 1.5x1cm was seen on X-ray knee joint (lateral view) [Table/Fig-1]. Considering the history and X-ray findings, a clinical diagnosis of intra-articular loose bodies which were caused by osteoarthritis was made. An arthrotomy was performed and the excised tissue was found to be quantitatively more than that which was visualized as loose bodies on plain X-ray. Grossly, removed tissue appeared as a grey yellow, globular, soft tissue mass, which measured 2.5×1.5 cm. The tissue was sent for a histopathological examination.
X- Ray Lateral showing a single small loose body (arrow head) in knee joint

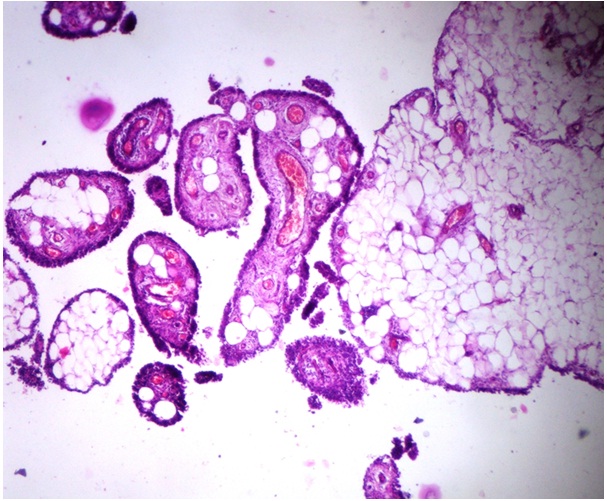
Microscopic examination of loose bodies revealed a tumour which was composed of well defined lobules of mature adipose tissue, which was lined by three to four layered synovial epithelial cells. Few lobules enclosed congested blood vessels. There was no evidence of necrosis, giant cell reaction, collagenization, cartilaginous or bonny metaplasia and presence of any foreign body or crystals.[Table/Fig-2 and 3] A diagnosis of an intra-articular synovial lipoma was made.
HPE showing lobules of mature adipose tissue lined by synovial lining with congested blood vessels (H&E , 100X)
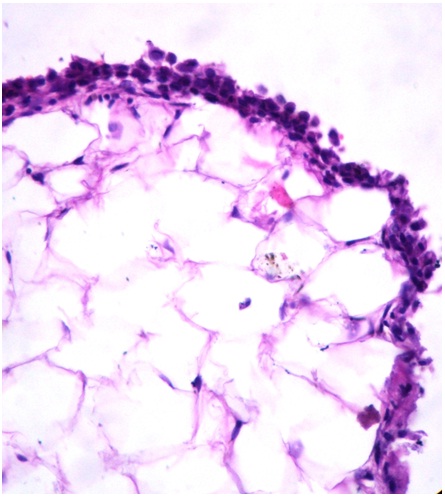
HPE showing lobules of mature adipose tissue lined by multilayered synovial lining (H&E , inset figure 2,400X)
Discussion
Lipoma is very common benign tumour which accounts for approximately 50% of soft tissue tumours, with an equal sex incidence. An intra-articular lipoma is a variant which is defined by its typical intra-articular location, which constitutes less than 1% of all lipomas [4]. In the intra-articular location, the knee joint is most commonly involved. Other sites which are less commonly involved are hip elbow, shoulder and spine [5].
Clinically, a synovial lipoma commonly presents as a mass with pressure effects or as a sudden locking of the joint, which is caused by loose bodies, which are formed by detachment of a part of a synovial lipoma in the joint cavity. Rarely, it may present with sudden pain which is caused by the torsion of the stalk of lipoma, if it is pedunculated [6,7]. In the present case, patient presented with pain and episodic locking of the left knee joint. A lateral view X-ray examination showed non–specific changes of osteoarthritis and a small radio-opaque soft tissue shadow which was labeled as a loose body within the joint cavity. In conjunction with clinical history, X-ray findings and other sero-microbiological investigations, clinical diagnosis of episodic locking of the knee joint was attributed to formation of loose bodies, which is a relatively common sequelae in osteoarthritis. In the present case, HPE revealed the nature of loose body as that of a true intra-articular synovial lipoma.
Commonly, the nature of loose body in osteoarthritis is either chondromatous or osteochondral. Various other causes of loose bodies joints include, Lipoma arborescens, synovial osteochondromatosis, Pigmented Villonodular Synovitis (PVNS) and diseases like gout, amyloid arthropathy, Hoffa’s disease ,synovial rheumatoid arthritis, tuberculous arthritis, coccidioidomycotic arthritis, deposition hemangioma and liposarcoma [8]. As the treatment modalities and prognoses vary with the specific diseases, on definition of exact nature of the loose body on the basis of findings of various modalities like imaging studies, histopathology carries utmost significance.
Most of the loose bodies are not visible on simple roentegenographs unless they are calcified. Air or double contrast arthrography may be necessary to visualize and quantify the nonossified and non calcified bodies. In the present case, arthrography was not done. Above mentioned loose bodies have characteristic radiological (especially with MRI scans) and histopathological characteristics with which they can be easily distinguished from each other and from synovial lipoma [8]. Synovial chondromatosis grossly and microscopically presents as a proliferating lesion with cartilaginous metaplasia of synovium. PVNS grossly appears as a villous to a multi–nodular lesion with a varied clinical presentation, but it microscopically shows proliferative synovial hyperplasis with extensive collagen laying, iron deposits, foam cells and giant cells. Gouty arthritis, rheumatoid arthritis and infectous arthritis have characteristic gross and histological features like tophaceous nodules, rheumatoid nodules and demonstration of infectious agents in lesions which show variable inflammatory and giant cell reactions respectively [9]. But the true intra-articular synovial lipoma must be distinguished from its more common and closer mimic i.e, Lipoma arborescens. In Lipoma arborescens, typical clinical presentation is a longstanding, painless joint swelling which is accompanied by intermittent effusions. Lipoma arborescens is grossly characterized by numerous villous projections of fatty synovial tissue within the joint and microscopically by patchy lipomatous metaplasia which is intermixed with a proliferating synovium [2]. The true Intraarticular lipoma clinically presents with a variable symptomatology and it is microscopically characterized by well defined lobules of fatty tissue which are lined by a hyperplastic, synovial epithelium [2,6,7]. Lipoma arborescens is usually associated with post-traumatic or inflammatory joint conditions, but it also may arise de novo. Exact aetiology of synovial lipoma is unknown. Some authors believe that it arises as a result of metabolic disturbances, while others have suggested role of repeated micro traumatization on mobile articular surfaces like knees [1,5,8,10,11]. On both T1- and T2-weighted images in MRI, a true intra-articular synovial lipoma is found to arise from the patellar fat, usually from suprapatellar pad of the fat, but a single case of synovial lipoma which arose from infra–patellar pad of fat has also been reported in China. On MRI, a lipoma appears as single pedunculated fatty mass with high signal intensities which match those of surrounding fat, whereas Lipoma arborescence appears as a thick frond like mass with signal intensities of all pulses. Hoffa’s disease, an another closer mimic of the above conditions, appears as areas of low signal intensities. Due to different prognostic factors, all these entities require excisions of loose bodies and this mandates their histopathological examination, which is gold standard of diagnosis [2,7,8].
Significant implication of making a diagnosis of a synovial lipoma, lies in the fact that due to its heteromorphic nature, it has a tendency to recur, damage the joint and cause joint dislocation. Rarely, it may transform to a liposarcoma [6,7]. Considering the magnitude of above complications, a Synovial lipoma requires immediate excision.
Intra–articular synovial lipomas, though they are very rare, should always be included in differential diagnosis of intra-articular loose bodies in patients who suffer from osteoarthritis as a cause of locking of the knee joints.
[1]. Pudlowski RM, Gilula LA, Kyriakos M, Intraarticular lipoma with osseous metaplasia: radiographic, pathologic correlationAm J Roentgenol 1979 132:471-73. [Google Scholar]
[2]. Weihong Z, Wanchun W, You C, Tao X, Synovial lipoma in intra-patellar fat pad of the knee jointPak J Med Sci 2012 28:228-30. [Google Scholar]
[3]. Khan AM, Cannon S, Levack B, Primary Intra-articular liposarcoma of the kneeThe Journal of Knee Surgery 2003 16(2):1-3. [Google Scholar]
[4]. Myhre OJ, A consecutive 7-year series of 1331 benign soft tissue tumoursActa Orthop. Scand 1981 52:287-93. [Google Scholar]
[5]. Hill JA, Martin WR, Milgram JW, Unusual arthroscopic knee lesions: case report of an intra-articular lipomaJ Natl Med Asso 1993 85(9):697-99. [Google Scholar]
[6]. Yeomans NP, Robertson A, Calder SJ, Torsion of an intra-articular lipoma as a cause of pseudo locking of the kneeArthroscopy 2003 19(3):E27 [Google Scholar]
[7]. Hirano K, Deguchi M, Kanamono T, Intra-articular synovial lipoma of the knee joint (located in the lateral recess): a case report and review of the literatureKnee 2007 14(1):63-67. [Google Scholar]
[8]. Sheldon PJ, Forrester MD, Learch JT, Imaging of Intraarticular MassesRadiographics 2005 25(1):105-19. [Google Scholar]
[9]. Peter GB, Diagnostic surgical pathology 1999 3rd edPhiladelphiaLippincott Williams and Wilkins:223-42.Chapter 6, Joint Diseases [Google Scholar]
[10]. Husson JL, Chales G, Lancien G, Pawlotsky Y, Masse A, True intra-articular lipoma of the lumbar spineSpine 1987 1(2):820-22. [Google Scholar]
[11]. Motsis E, Vasiliadis HS, Xenakis TA, Intraarticular synovial lipoma of the knee located in the intercondylar notch, between ACL and PCL: a case report and review of the literatureKnee Surg Sports Traumatol Arthrosc 2005 Nov 13(8):683-88. [Google Scholar]