Lipoma on Palmar Aspect of Thumb: A Rare Case Report
Hemlata T. Kamra1, Santosh L. Munde2
1 Associate Professor, Department of Pathology, Bhagat Phool Singh Government Medical College for women, Khanpur Kalan, Sonepat, Haryana, India.
2 Associate Professor, Department of Pathology, Bhagat Phool Singh Government Medical College for women, Khanpur Kalan, Sonepat, Haryana, India.
NAME, ADRESS, E-MAIL ID OF THE CORESPONDING AUTHOR: Dr. Hemlata T. Kamra, Associate Professor, Department of Pathology, Bhagat Phool Singh Government Medical College for women, Khanpur Kalan, Sonepat, Haryana.
Phone: 08983483407,
E-mail: hemlatamunde@rediffmail.com
Lipomas account for approximately 16% of soft tissue mesenchymal tumours. They are uncommon in hand and those which involve the fingers are very rare, with a reported incidence of 1%. In extremities, they often arise from the sub–fascial tissues of the hands and feet, where they may be mistaken for ganglion cysts. A careful dissection is necessary during the surgical procedure, in order to avoid recurrence. Here, we are presenting the case of an 8 years old boy who had Lipoma on palmar aspect of thumb.
Lipoma, Thumb, Tendon sheath
Case Report
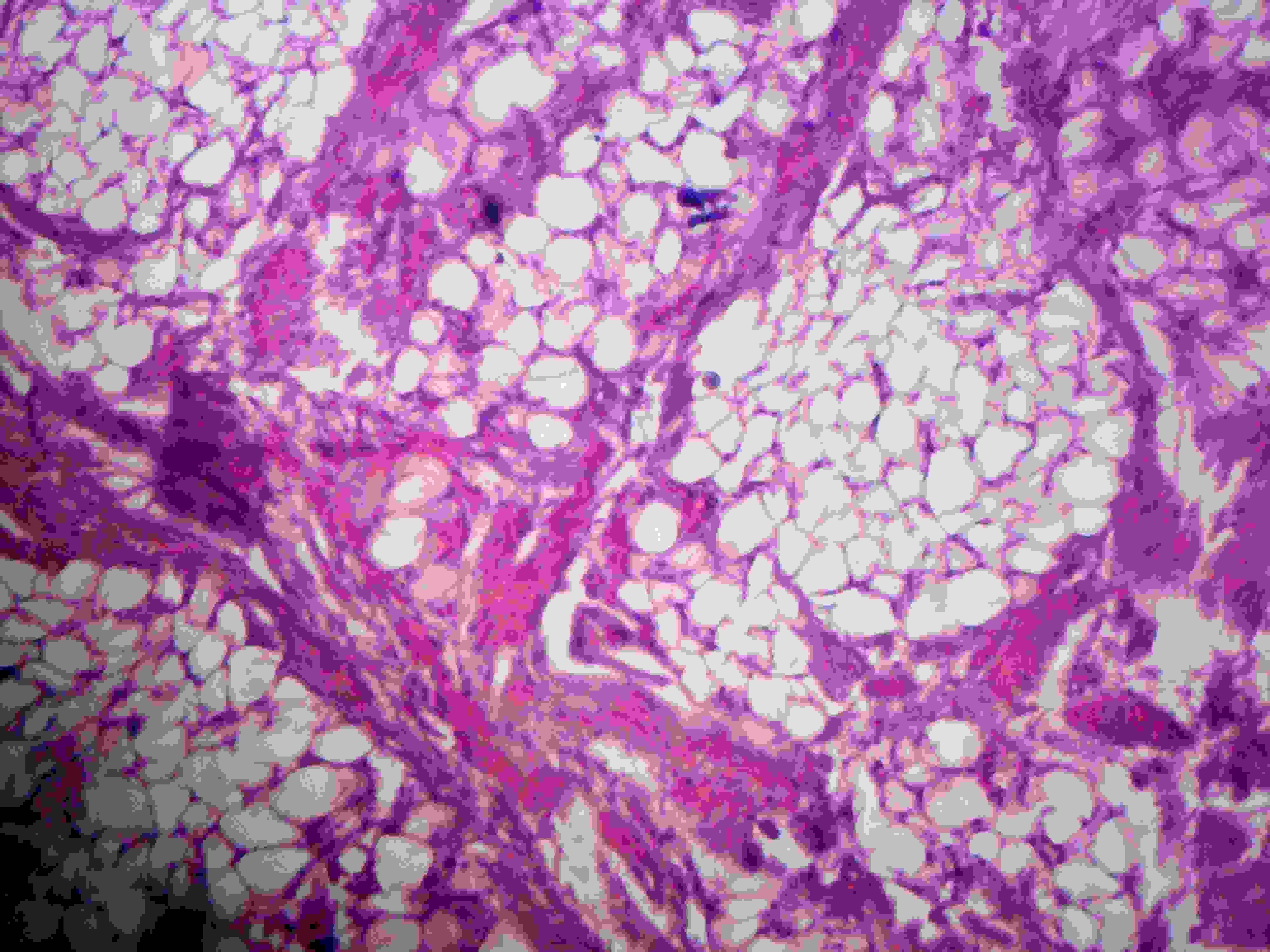
An 8 years old boy presented with a swelling on flexor aspect of proximal and distal phalanx of right thumb.The patient had noticed a diffuse swelling six months ago, which had gradually reached the present size of 5 × 4 × 2.5 cm. The mass was superficial, painless, soft and mobile. Patient had visited the Orthopaedics Outpatients Department because of a difficulty in writing in school and a limitation in the range of movement. Blood counts and RBS were within normal limits. On Fine needle aspiration, 0.2 ml of oily material was aspirated.Smears which were prepared showed clusters of mature adipocytes only and the case was reported as a Lipoma. A plain X ray showed no invasion of the bone.The tumour was removed completely, including its extensions into the tendon sheath, without damaging neurovascular bundle. Grossly, the specimen comprised of a thinly encapsulated, yellow, fibrofatty tissue which measured 5x3x2.5cm, along with the tendon, which measured 2.5cms [Table/Fig-1]. Cut section was yellow, glistening and lobulated [Table/Fig-2]. Microscopic examination revealed a thinly encapsulated tumour which was composed of mature fatty tissue, where a central lipid droplet and a peripherally located nucleus formed the characteristic signet ring cell. Sections near the tendon revealed lobules of fatty tissue which were traversed by mature fibrous tissue [Table/Fig-3 and 4].
Gross photograph showing thinly encapsulated fibrofatty tissue along with a tendon attached to it

Cut section shows yellow, glistening, lobulated fibrofatty tissue

Shows aggregates of mature adipocytes with tendon
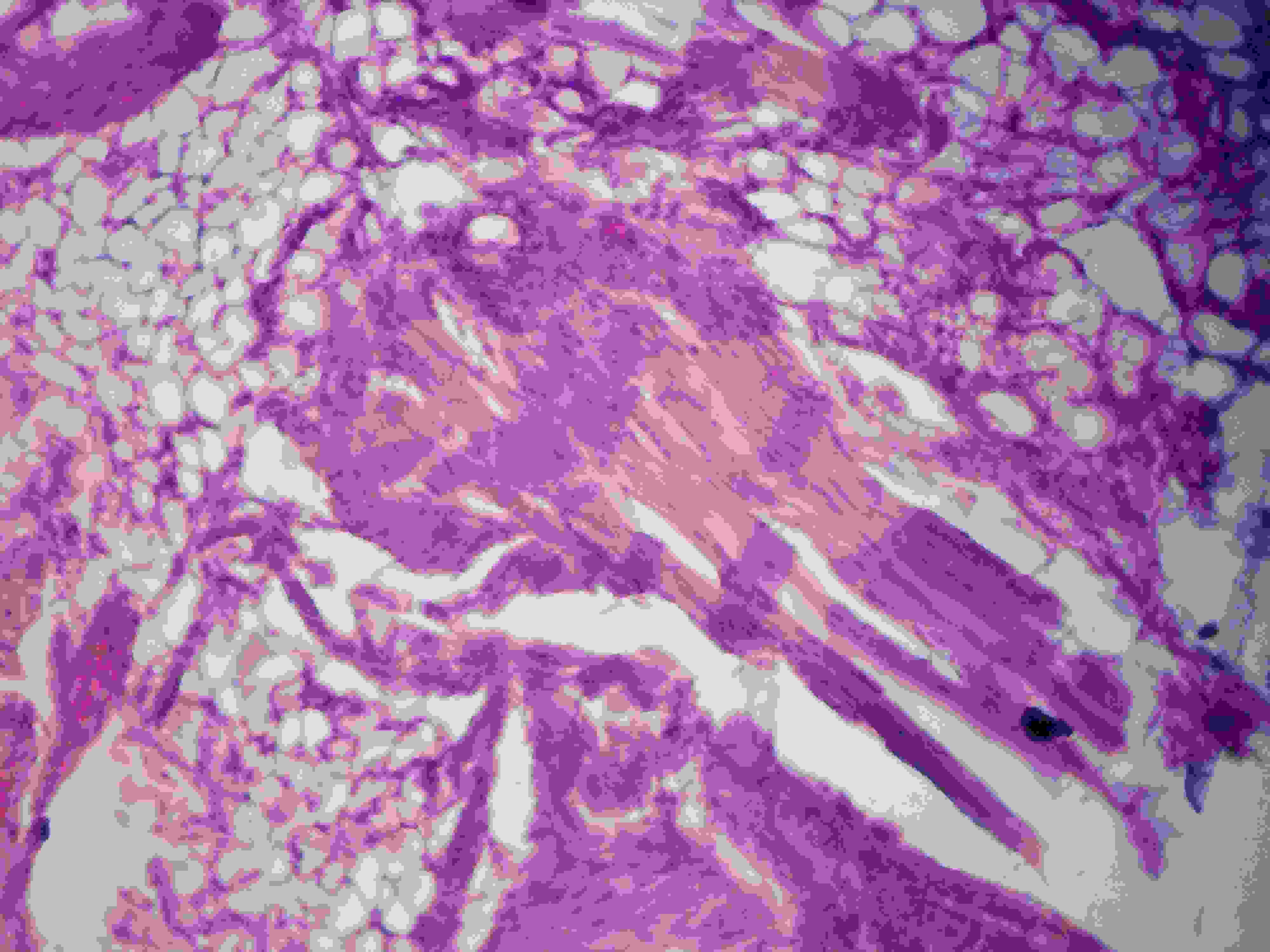
shows lobule of mature adipocytes traversed by fibrous tissue.
Discussion
Lipomas of the tendon sheaths of fingers are very rare. Reported incidence is 1% [1]. The first case of lipoma of finger was reported by Stein in 1959 [2]. Approximately 15 cases of lipomas of fingers have been published in literature [2]. But lipomas, particularly of thumb, have been reported only rarely.
Lipomas of the tendon sheaths and joints are of two types: 1) solid fatty masses that extend along tendons for varying distances are known as Lipoma simplex symmetricum and 2) lipoma like lesions that consist chiefly of hypertrophic synovial villi which are distended by fat ,most commonly in the region of the knee joint, are known as Lipoma arborescens [3]. When they occur in tendon sheath, these lesions are called endovaginal tumours whereas deep lipomas which arise outside the tendon sheath are known as epivaginal tumours [4].
They may also arise from juxtra-articular regions or the periosteum (parosteal lipoma), sometimes causing nerve compression, erosion of bone or focal cortical hyperostosis [5].
Patients generally present with mild aching pain in affected parts. Occasionally, it presents as an acute inflammatory condition with swelling, redness and warmth in overlying tissue. Frequently, crepitus of the soft tissue is observed [3]. Rarely do patients present with trigger finger [6]. In 2008, Baena–Ocampo LC et al., reported tendon sheath lipoma which was associated with quadriceps tendon rupture [7]. Campbell, in 1954, reported a lipoma producing lesion in the deep branch of the radial nerve, which was detected by applying pressure only [8].
The aetiology of a lipoma is unknown. The leading genetic theory for lipoma formation proposes that spontaneous karyotypic anomalies lead to chromosomal fusion products which promote proliferation of adipocytes. It is most commonly associated with translocations and rearrangements of the 12q13~q15 chromosomal region [9]. A competing theory which was proposed for lipoma following trauma revealed that growth factors, cytokines, and other inflammatory mediators which are released following blunt trauma to soft tissue, induce preadipocyte differentiation into mature adipocytes and form a clinically apparent mass [10].
CT scan and MRI are diagnostic in 71% of cases. MR images reveal a tissue that is isointense and relative to subcutaneous fat, regardless of pulse sequences. When contrast is applied, the mass is not enhanced, except its capsule. In 37–49% of cases CT or MR images reveal intrinsic thin septa (of less than 2 mm), a sign that is considered almost pathogonomic for the diagnosis of lipoma [2]. Lipoma on fingers is uncommon and it is rarely considered because of other common conditions like ganglion cysts, giant cell tumours of tendon sheath, epidermal inclusion cysts, lipomas, neuromas, nerve sheath tumours, fibromas and glomus tumours. CT and MRI generally rule out neoplastic lesions like liposarcomas. After surgical excisions, the recurrence rate is less than 5% within 1 year of resections [11].
In our case, diagnosis was easy, as the tumour was located sub–cutaneously, with a part extending into the tendon sheath.The tumour was removed surgically and patient attained his full range of motion after three weeks of undergoing surgery.
Conclusion
Uncommon lipomas of tendon sheath should be considered as a differential diagnosis in swelling of hands, especially of fingers.
[1]. de Giorgi V, Salvini C, Sestini S, Alfaioli B, Carli P, Lipoma of the finger: A case report and differential diagnosisClin Exp Dermatol 2005 30:439-40. [Google Scholar]
[2]. Chronopoulos E, Ptohis N, Karanikas C, Kalliakmanis A, Plessas S, NeofytouIoannis. Patient presenting with lipoma of the index finger: a case reportCases Journal 2010 3:20 [Google Scholar]
[3]. Sullivan CR, Dahlin DC, Bryan RS, Lipoma of the tendon sheath. From the section of Orthopaedic Surgery and section of Surgical pathology(Mayo Clinic and Mayo Foundation, Rochester) 1956 38(6):1275-80. [Google Scholar]
[4]. Enzinger FM, Weiss SW, Soft tissue tumors3rd editionSt. LouisMosby:381-430. [Google Scholar]
[5]. Kraus MD, Guillou L, Fletcher CD, Well differentiated inflammatory liposarcoma, an uncommon and easily overlooked variant of a common sarcomaAm J Surg Pathol 1997 21:518 [Google Scholar]
[6]. Pampliega T, Arenas AJ, An unusual trigger fingerActa Orthopaedica Belgica 1997 63(2):132-33. [Google Scholar]
[7]. Baena-Ocampo L del, Encalada-Diazl Marin-Arriaga Tendon sheath lipoma associated with quadriceps tendon ruptureCir Cir 2008 76(3):265-69. [Google Scholar]
[8]. Mikhail IK, Median nerve lipoma in the handThe Journal of Bone and Joint Surgery 1964 46(4):726-30. [Google Scholar]
[9]. Nadar MM, Bartoli CR, Kasdam ML, Lipomas of the Hand:A review and 13 patient case seriesePlasty 2010 10:549-59. [Google Scholar]
[10]. Aust MC, Spies M, Kall S, Lipomas after blunt soft tissue trauma: are they real? Analysis of 31 casesBr J Dermatol 2007 157(1):92-99. [Google Scholar]
[11]. Adair FE, Pack GT, Farrier JH, LipomaAm J Cancer 1932 16:1104 [Google Scholar]