Solitary Plasmacytoma of Skull: A Rare Cytological Diagnosis
Manmeet Kaur Gill1, Manisha Makkar2, Satinder Pal Singh Bains3
1 Senior Resident, Department of Pathology, SR in UCMS/GTBH, Delhi, India.
2 Assistant Professor, Department of Pathology, Adesh Medical College, Bathinda, Punjab, India.
3 Senior Resident, Department of Surgery, SR in Lok Nayak Hospital, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Manmeet Kaur Gill, H.N. 22265/A, Shant Nagar, Bathinda, Punjab, India.
Phone: 09876610985,
E-mail: drmanmeet16@hotmail.com
Solitary Plasmacytoma of the Skull (SPS) is very rare and only 35 cases have been reported in the English literature. It remains controversial whether a solitary plasmacytoma of the skull is essentially identical with a Solitary Plasmacytoma of Bone (SPB) or not. A solitary plasmacytoma of bone, which includes a solitary plasmacytoma of the skull, is characterized by a radiologically solitary bone lesion, neoplastic plasma cells in the biopsy specimen, fewer than 5% plasma cells in bone marrow, less than 2.0 g/dl monoclonal protein in the serum when it is present and a negative urine test for Bence Jones protein (monoclonal light chain). A solitary plasmacytoma of bone tends to disseminate or progress to multiple myeloma, even as long as 7-23 years after its presentation.
Fine needle aspiration cytology, Solitary plasmacytoma, Skull
Introduction
Plasma cell neoplasms are disorders which arise from the proliferation of a single clone of B-cell lymphocytes, 3% of which present as solitary lesions of bone or soft tissue [1]. Fine-needle aspiration cytology (FNAC) has been used as a first line investigation. We are reporting a rare case of a solitary plasmacytoma of the skull, where a diagnosis was distinctly made on cytology.
Case Report
A 48-year-old female first noted a painless, soft swelling which measured 4 x 3 cm, in the midfrontal region. On a neurological examination, no abnormalities were found. MRI of the brain revealed a mass lesion with a heterogeneous signal intensity in left frontal region, which measured 35 x 15 x 32 mm. There is an extra–cranial component of mass, which extended intracranially to the dural space through a defect in left frontal bone, near coronal suture. There was focal erosion of left frontal bone. The extra–axial component of the mass caused an indentation on the left frontal lobe, with buckling of the grey and white matter interface and a mass effect on left frontal lobe. Laboratory examinations found a red blood cell count of 4.07 x 106 /mm3, haemoglobin -13.0 g/dl, white blood cell count -5800/mm3, platelets -3.0 x 105 /mm3, total serum protein- 6.0 g/dl, globulin- 2.2 g/dl and serum calcium -4.7 mg/dl, all of which were within the normal range. Other serum electrolytes were also normal.
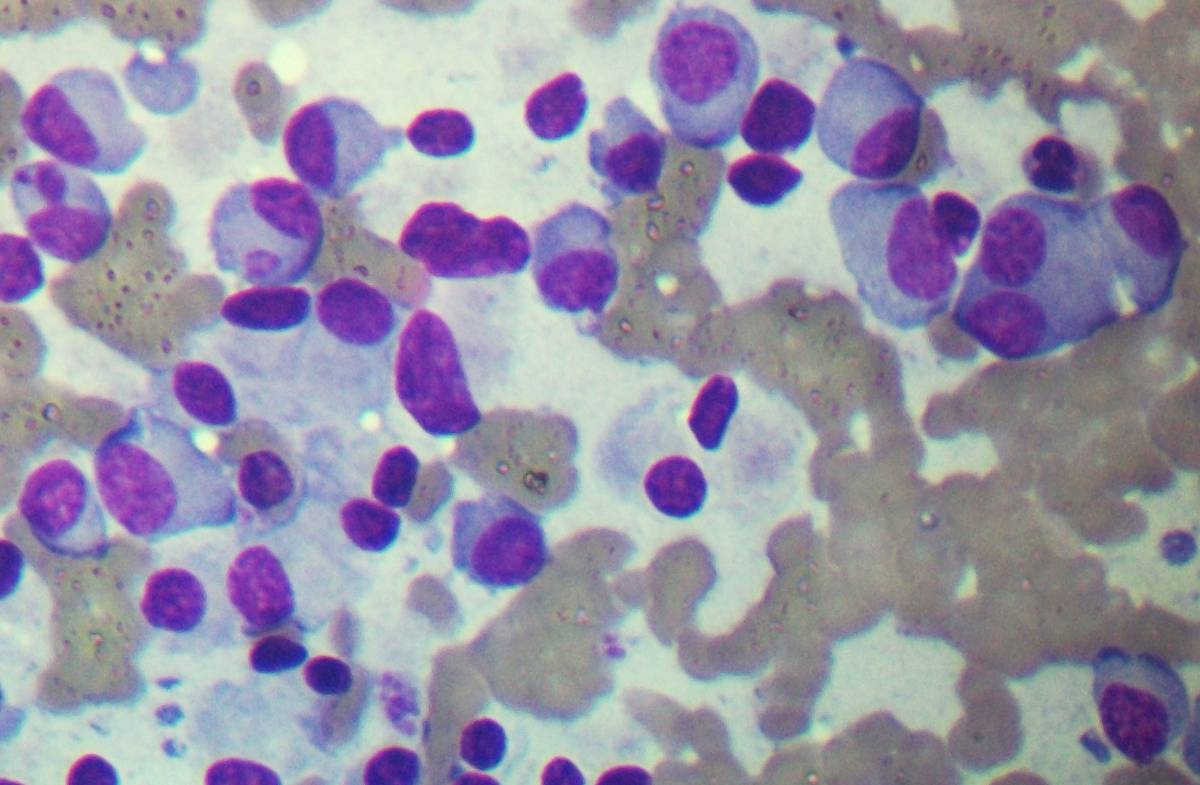
FNAC was done and cytologic smears which were stained with MGG revealed multiple plasma cells, both typical and atypical, which were arranged in sheets. Binucleated plasma cells with eccentric nuclei, a characteristic cartwheel appearance along with prominent nucleoli, a perinuclear halo, and abundant cytoplasm, were also seen. The cytologic picture was highly suggestive of a plasmacytoma. [Table/Fig-1] Bone marrow aspiration revealed a normocellular marrow and no systemic myelomatosis, with a myeloid:erythroid ratio (M:E) of 2:1. The immunoelectrophoresis of serum proteins was within the normal range. A urine test which was done for Bence Jones protein was negative and a skeletal survey which was done, which was inclusive of radiographs of the spine and pelvis revealed no abnormality, thus confirming the diagnosis of a solitary plasmacytoma of the skull. The patient refused surgery and was treated with radiotherapy, with a decrease in swelling after five weeks.
FNAC showing sheet of plasma cells with binucleated plasma cell
Discussion
Solitary Plasmacytomas of Bone (SPB) are defined as clonal proliferations of plasma cells which are identical to those of plasma cell myeloma, which manifest a localized osseous growth. Plasmacytomas can be divided into multiple, solitary osseous, and solitary extra–osseous or extra–medullary plasmacytomas and are rare as compared to multiple myeloma [2]. Localized SPB is a rare disease and it is characterized by one or two isolated bone lesions, with no evidence of disease dissemination and it has been considered to be curable with radiotherapy and surgical resection. This treatment is sufficient to achieve a long term survival [3]. The incidence of SPB has been reported to be approximately 3/10 00 000 annually [4].
As compared to that of a solitary plasmacytoma of the skull base, the prognosis for a solitary plasmacytoma of the skull vault seems to be good, when there is no evidence of systemic myelomatosis. Nevertheless, solitary plasmacytoma of the skull vault also has a possibility of being identical to SPB. True SPS is much rarer than SPB and only 35 cases have been reported in the English literature [5].
The two main differential diagnoses on cytology include metastatic carcinoma and osteoblasts in case of bony lesions. In metastatic carcinoma, clusters of cells which have an acinar or a glandular pattern, with features of malignancy are seen, whereas osteoblasts can be differentiated on the absence of a typical clear cytoplasm or a perinuclear halo, as is seen in plasmacytomas. Plasmacytomas exhibit monoclonal kappa or lambda light chains, whereas plasma cells of reactive conditions like chronic osteomyelitis are polyclonal. Also, myeloma cells usually stain positive for the natural killer antigen CD56, whereas reactive plasma cells usually do not. Immunohistochemistry also can be helpful in poorly differentiated cases, when lymphoma could be included in the differential diagnosis.
The diagnosis of SPB is based on the findings of a radiologically solitary bone lesion, plasma cells in the biopsy specimen, fewer than 5% plasma cells in bone marrow, less than 2.0 g/dl monoclonal protein (M-protein) in the serum when it is present, a negative urine test for Bence Jones protein, no evidence of hyperglobulinaemia and hypercalcaemia and absence of anaemia. A surgical removal, followed by a postoperative irradiation, is the treatment of choice, because SPB is very radiosensitive. High local control rates are reported with radiotherapy, although the optimum dose and extent of radiotherapy portals remain controversial. The local tumour recurrence rate is less than 10% by conventional radiotherapy. The efficacy of chemotherapy for SPB, however, is not certain. Shih et al., and Delauche-Cavallier et al., failed to find any benefit on the outcome for patients who had received chemotherapy [5].
On the other hand, the minimum criterion for the diagnosis of MM is the existence of more than 10% plasma cells in the bone marrow or those for plasmacytoma plus one of the following:
M-protein in the serum (usually 3.0 g/dl),
M-protein in the urine and
the presence of an osteolytic lesion [6].
A long term follow up is necessary, because in 35% to 55% of patients, multiple myeloma develops often 10 to 12 years after initial diagnosis.
Conculsion
The present case of a solitary plasmacytoma which is diagnosed on FNAC highlights the utility of FNAC and it stresses that cytology can not only be used as an investigative tool, but also as a diagnostic tool.
[1]. Wiltshaw E, The natural history of extramedullary plasmacytoma and its relation to solitary plasmacytoma of bone and myelomatosisMedicine (Baltimore) 1976 55:217-38. [Google Scholar]
[2]. Masood Ashiq, Hudhud Kanan H, Hegazi AZ, Syed Gaffar, Mediastinal plasmacytoma with multiple myeloma presenting as a diagnostic dilemmaCases J. 2008 1:116 [Google Scholar]
[3]. Ooi GC, Chim JC, Au WY, Khong PL, Radiologic Manifestations of Primary Solitary Extramedullary and Multiple Solitary PlasmacytomasAJR Am J Roentgenol 2006 186:821-27. [Google Scholar]
[4]. Mendenhall CM, Thar TL, Million RR, Solitary Plasmacytoma of bone and soft tissueInt J Radiat Oncol Biol Phys 1980 6:1497-501. [Google Scholar]
[5]. Minoru T, Soichiro S, Kazuhiro N, Yukihiro N, Solitary Plasmacytoma of the Skull: a Case ReportJpn J Clin Oncol 1998 28:626-30. [Google Scholar]
[6]. Kyle RA, Multiple myeloma. An update on diagnosis and managementActa Oncol 1990 29:1-8. [Google Scholar]