Chondroid Choriostoma of Palatine Tonsil – A Rare Entity
Jyotsna Naresh Bharti1, Nivedita Ghosh2, Prerna Arora3, Vasudha Goyal4
1 Senior Resident, Department of Pathology, Maulana Azad Medical College, New Delhi, India.
2 Senior Resident, Department of Pathology, Maulana Azad Medical College, New Delhi, India.
3 Assistant Professor, Department of Pathology, Maulana Azad Medical College, New Delhi, India.
4 Junior Resident, Department of Pathology, Maulana Azad Medical College, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jyotsna Naresh Bharti, Senior Resident, Department of Pathology, Maulana Azad Medical College, New Delhi, India.
Phone: +919899047062,
E-mail: jyotsnamamc@gmail.com
A choristoma or heterotopias is an aggregate of microscopically normal cells or tissues which occurs in aberrant locations. A choristoma is a tumour like mass, whereas heterotopias refers to a displaced tissue which is necessarily not a swelling or a neoplasm. We are reporting a case of a 24 year old female who presented with recurrent tonsillitis and halitosis. On examination, the tonsils were found to be enlarged. Because of the persistent symptoms, a tonsillectomy was performed. The histopathological examination showed features of chronic tonsillitis, along with presence of mature islands of hyaline cartilage which were surrounded by lymphoid follicles and focal areas of calcification and osseous metaplasia.
Osseous metaplasia, Calcification, Cartilage, Tonsilitis
Case Report
A 24 year old female presented to ENT OPD with the complaint of a difficulty in swallowing, snoring and halitosis, for four month duration. Along with off and on episodes of recurrent sore throat and fever. There was no history of other otological signs and symptoms. The local oral examination revealed grade three hypertrophy of bilateral palatine tonsil, which was covered with specks of whitish exudates. On palpation, the tonsils were found to be firm and gritty and rest of the head and neck examination was unremarkable. A clinical diagnosis of tonsillitis was made. The patient underwent a bilateral tonsillectomy and the specimen was sent for a histopathological examination.
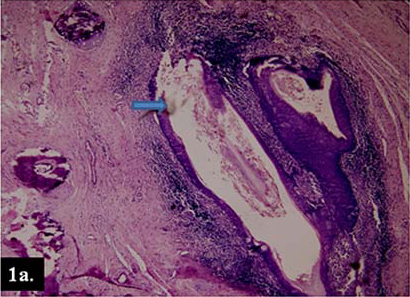
Grossly, the excised tissue was grey brown, globular, firm and gritty in consistency and each piece measured 1.5 x 1.5 x 1 cm. Cut surface was smooth, homogenous and pale brown. On histopathological examination, sections from both the tonsillar tissue were found to be covered by stratified squamous epithelium, with features of chronic tonsillitis and the intervening crypts showed keratinous flakes [Table/Fig-1a]. There were islands of mature hyaline cartilage which were surrounded by lymphoid follicles [Table/Fig-1b], with focal areas of calcification [Table/Fig-1c] and osseous metaplasia [Table/Fig-1d]. The patient did not report back to our centre and was lost to follow up.
Section revealing stratified squamous epithelium with intervening crypts showing keratinous flakes. (H&E x100)
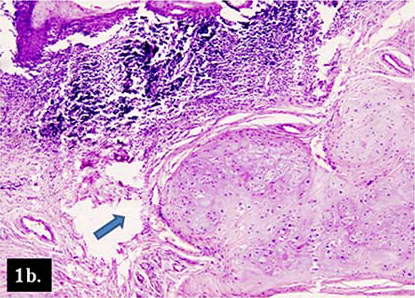
Lobules of hyaline cartilage surrounded by lymphoid follicles and stratified squamous epithelium. (H&E x400)
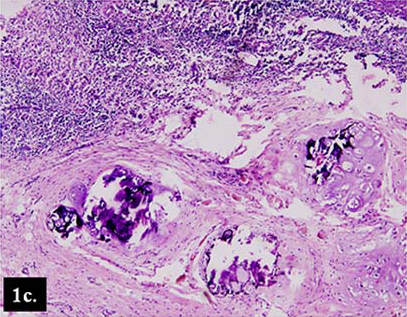
Calcification within the lobules of hyaline cartilage. (H&E x400)
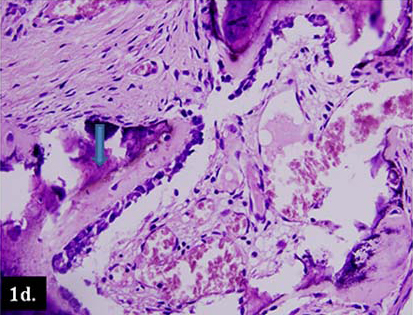
Foci of osseous metaplasia with calcification. (H&E x600)
Discussion
Choristomas which occur in the head and neck region are rare, benign lesions. The other sites at which they occur are pharynx, hypopharynx, oral mucosa and middle ear. Osseous and cartilaginous choristomas show a striking predilection for the posterior part of the tongue [1]. Heterotopic tissues which are seen in the oral cavity are gastric mucosa, glial tissue and sebaceous glands [2]. Here, we are reporting a case of chronic tonsillitis with a cartilaginous choristoma.
A chondroid choristoma was first described by Berry in 1890. The age at diagnosis of these patients varied greatly, ranging from 10 to 80 years, with a mean age of 47 years [3]. Chondroid choristomas of the tongue are more common in females, although in palatine tonsils, they do not have any sex predilection [4]. Various mechanisms have been suggested for pathogenesis of heterotopia, that are multi–lineage potential of mesenchymal progenitor cells which were able to differentiate into various mesenchymal lineages, as pro–posed by Haemel et al., [5]. The local chemical or physical changes and were brought about by chronic inflammation, may lead to liberation of osteogenic substances which produced by heterotopic cartilage proliferation and bone formation, as proposed by Lindholm et al., [6].
Cartilaginous choristomas should be distinguished from cartilaginous metaplasia, which are characterized by diffuse deposits of calcium and scattered cartilaginous cells, which are arranged in various stages of maturation in single or clustered cartilaginous foci, which are often associated with the soft tissue they is present beneath ill fitting dentures [7]. Simple excision of the lesion, along with surrounding soft tissue is recommended and it is also considered as curative.
Although recurrences have not been documented in head and neck choristomas, some oral cases have been reported to be recurrent and so, perichondrium should be removed, because it may have the potential to develop a new cartilage. However it is expected to follow a benign course as any normal cartilage, elsewhere in the body. Our case had a tonsillar enlargement with features of tonsillitis clinically, which on histopathology, showed focal areas of calcification and predominantly, the tonsillar tissue with presence of mature hyaline cartilage, which is not a normal constituent of oropharyngeal epithelium and, therefore, by definition, the lesion was a choristoma rather than a heterotopia.
To conclude, choristomas are rare entity and of academic interest. This case underscores that although they are rare, a high index of suspicion for choristomas is needed, when a patient with recurrent tonsillitis is being evaluated. Clinically, if they are large in size, they can also be confused with true neoplasms.
[1]. Neville BW, Damm DD, Allen CM, Soft tissue tumors. Oral and Maxillofacial Pathology 2002 2nd editionPhiladelphiaW.B. Saunders:479 [Google Scholar]
[2]. Chou LS, Hansen LS, Daniels TE, Choristomas of the oral cavity: a reviewOral Surg Oral Med Oral Pathol 1991 Nov 72(5):584-93. [Google Scholar]
[3]. Bhargava D, Raman R, Khalfan Al Abri R, Bushnurmath B, Heterotopia of the tonsilJ Laryngol Otol 1996 110(6):611-12. [Google Scholar]
[4]. Majeed AA Abdul, Farah CS, Mixed choristoma on the anterior dorsal tongue: a new case and review of the literatureOral surgery 2011 4:26-29. [Google Scholar]
[5]. Haemel A, Gnepp DR, Carlsten J, Heterotopic salivary gland tissue in the neckJ Am Acad Dermatol 2008 58(2):251-56. [Google Scholar]
[6]. Lindholm ST, Hackman R, Lindholm RV, Hisodynamics of experimental heterotopic osteogenesis by transitional epitheliumActa Chiruagica Scandinavia 1973 139:617-23. [Google Scholar]
[7]. Cutright DE, Osseous and chondromatous metaplasia caused by denturesOral Surg Oral Med Oral Pathol 1972 34(4):625-33. [Google Scholar]