Aneurysmal Bone Cyst of the Pubis: A Case Report
Ashok Nayak1, Shreepad Kulkarni2, Avinash Kulkarni3, K. Natesh4, Monish Bami5
1 Professor and Unit Chief, Department of Orthopaedics, BLDEU’s, Shri B M Patil Medical College, Bijapur, Karnataka, India.
2 Assistant Professor, Department of Orthopaedics, BLDEU’s, Shri B M Patil Medical College, Bijapur, Karnataka, India.
3 Assistant Professor, Department of Orthopaedics, BLDEU’s, Shri B M Patil Medical College, Bijapur, Karnataka, India.
4 PG Student, Department of Orthopaedics, BLDEU’s, Shri B M Patil Medical College, Bijapur, Karnataka, India.
5 PG Student, Department of Orthopaedics, BLDEU’s, Shri B M Patil Medical College, Bijapur, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Monish Bami, Post Graduate Student, Department of Orthopaedics, Shri B M Patil Medical College, Bijapur-586103, Karnataka, India.
Phone: 9901050672,
E-mail: Monishbami86@gmail.com
An aneurysmal bone cyst is considered as a locally aggressive benign tumour. Intra-lesional extended curettage and bone-grafting is the mainstay of the treatment for aneurysmal bone cysts. Grafting is used usually in cases where the lesion compromises the mechanical strength of the bone. However, the massive size of the highly vascular tumour and the relative inaccessibility of its deeper extensions into the femoral vessels and the intra-abdominal structures, especially the urinary bladder, make it a relatively challenging case to perform excision and curettage.Presenting a case of a 15 years old male patient with the complaint of a right inguinal swelling since the past eight months. The swelling had started growing since the past two months and it was associated with pain. X-ray showed a lytic blowout legion of the entire right pubic ramus. An intra-lesional curettage was done. Complete tumour excision which was done by intra-lesional curettage and biopsy yielded satisfactory results with low complications and low recurrence of aneurysmal bone cyst of the superior ramus of the pubis.
Aneurysmal bone cyst of the superior ramus of the pubis, Primary involvement, Surgical excision with intra lesional curettage
Introduction
An aneurysmal bone cyst is a benign, reactive, non-neoplastic, expansile and a highly vascular osseous lesion which has been widely regarded a reactive process of uncertain aetiology, since its initial description which was made by Jaffe and Lichtenstein in 1942 [1]. Many hypotheses have been proposed to explain the aetiology and pathogenesis of aneurysmal bone cysts, and until very recently, the most commonly accepted idea was that an aneurysmal bone cyst was the consequence of an increased venous pressure and a resultant dilation and rupture of the local vascular network. However, studies which were done by Panoutsakopoulus et al., and Oliveira et al., uncovered the clonal neoplastic nature of aneurysmal bone cysts. Its primary aetiology has been regarded as an arteriovenous fistula within the bone. Primary aneurysmal bone cysts are rare, representing 1.4% of the primary bone tumours and 10% of them are primary pubic tumours. This lesion may be encountered in virtually any bone, although the metaphyses of the long bones are the most common location [2]. Previous studies have shown that > 70% of the cases occur during the first two decades of life [2,3]. Aneurysmal bone cysts are usually considered as benign but locally aggressive lesions; the lesion is usually successfully managed by extensive curettage and bone-grafting when a long bone is affected [2,4]. The tendency to develop an intra-operative bleeding, owing to the massive size of the highly vascular tumour and the relative inaccessibility of its deeper extensions into the adjacent ischium, made the direct surgical attack upon the lesion seem complicated, as the tumour was closely related to the pelvic vessels and the intra-abdominal structures. There is only limited information regarding the treatment of aneurysmal bone cysts in the pubis, with only very few articles being published on it. The literature on aneurysmal bone cysts in the pubis is limited to isolated case reports [5–9]. The aim of the present study was to report the results of the surgical treatment, complications, and rate of local recurrence following a total intra-lesional curettage of aneurysmal bone cysts of the superior ramus of the pubis.
Case Report
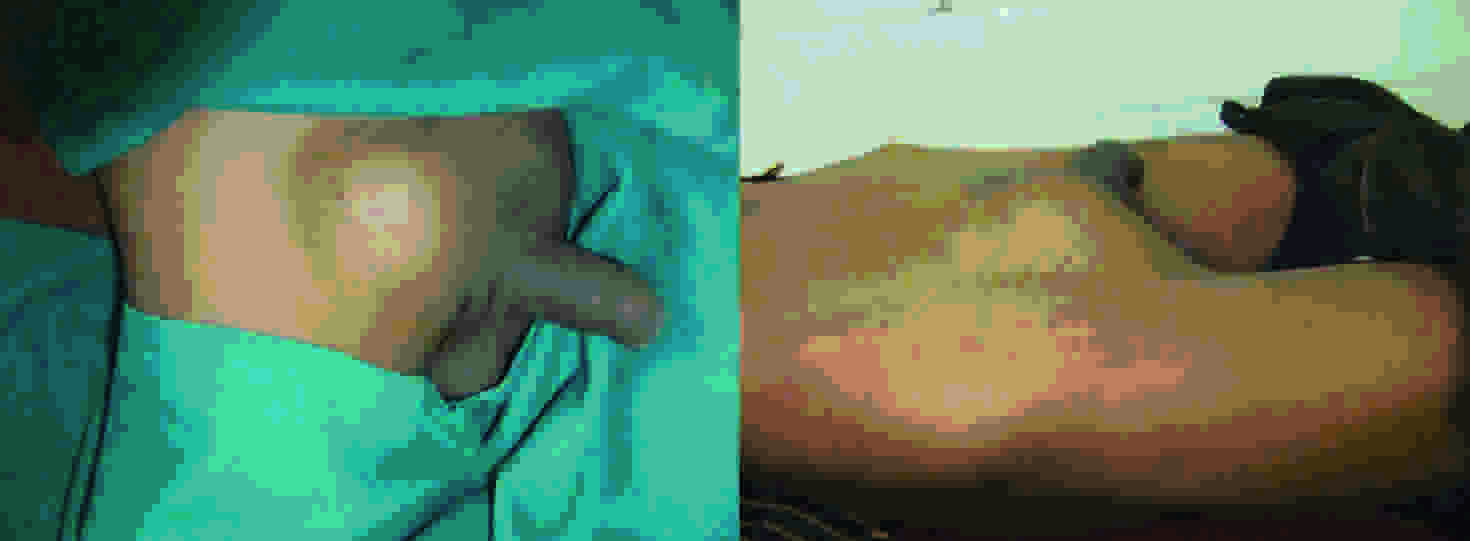
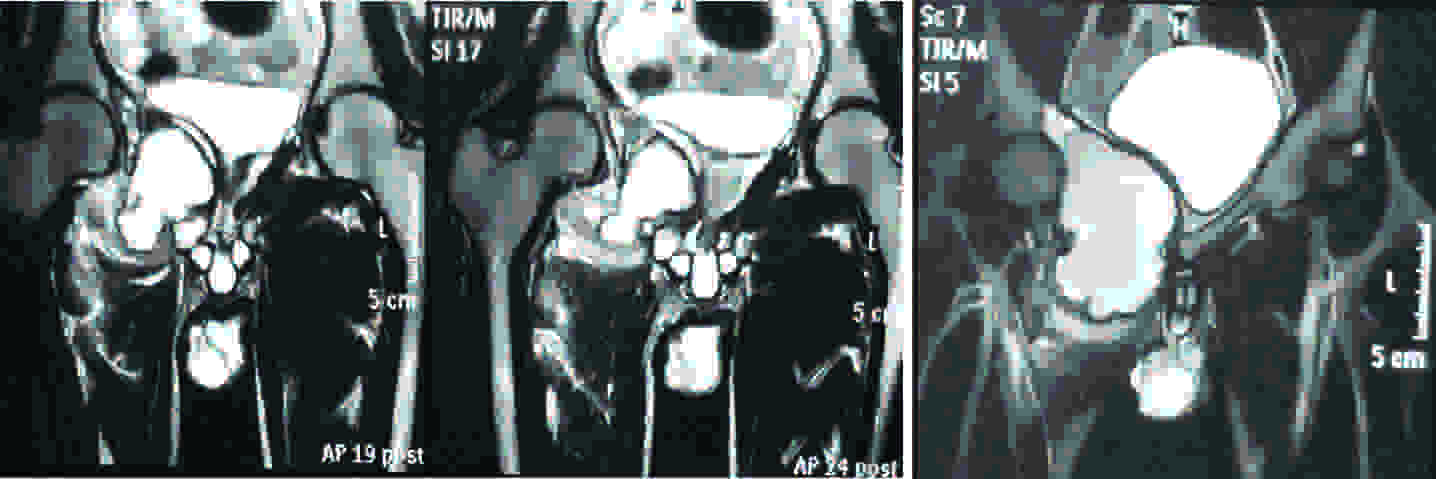
A 15-years old male patient presented with the chief complaint of a swelling over the right inguinal region which was there since eight months, which had rapidly grown in the past two months. The lesion was initially painless to start with, but the patient had started developing pain in the the past two months and had been unable to squat and sit cross legged. Range of motion at the hip joint was normal except that internal/external rotation was terminally painful. The swelling was 12x10 cm in size, solitary and fixed to the bone, with no local rise in temperature over the swelling. There were no visible pulsations or discolouration of the swelling. His gait was antalgic, with no history of fever or urinary complaints. A radiograph of the pelvis and both hips was taken, which showed a lytic blownout lesion which occupied the entire right superior pubic ramus. An MRI scan was done and it revealed a cystic lesion over the pubic ramus, which compressed the urinary bladder. Routine blood investigations were within normal limits. The HIV and HbsAg tests were negative. Serum alkaline phosphatase levels were elevated.
The patient was posted for surgical excision and curettage of the lesion with biopsy, along with consultation of a general surgeon.
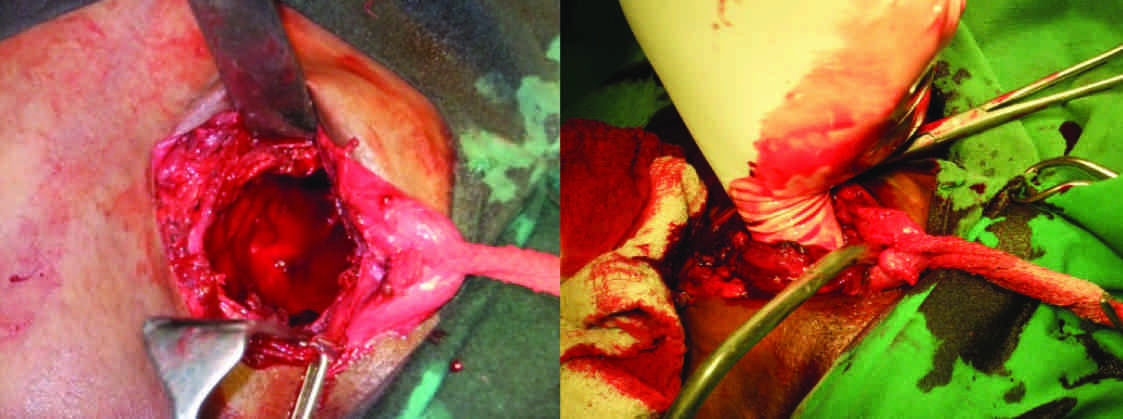
At operation, the mass was exposed extra-peritonially through a right supra-inguinal incision. The spermatic cord was isolated from the tumour mass and it was retracted and held separately, being secured from the surgical field. After the dissection, the protruding portion of the tumour was exposed. A 20cc syringe was taken and the lesion was punctured and aspirated. About 80cc of haematogenous fluid was removed from the anterior and inferior portions of the lesion and the posterior and superior portions of the lesion were palpated. They were found to be in close proximity to the intra-abdominal structures and their removal was not attempted, considering the risk. Bleeding from the cavity which had resulted from the curettage, could only be partially controlled by packing it with ribbon gauze. The spermatic cord was placed back and the wound was closed directly with 2-0 ethylon for skin with simple sutures, keeping the ribbon gauze in-situ, so that there was a way out for the drainage of the intra-lesional collection of the blood. Routine dressings were done by keeping the ribbon gauze in the lesion and it was left in position until the next dressing. Intra-lesional rubber catheter was removed after five days and sutures were removed after 13 days. There were no complications in the post operative period, except for scrotal oedema which had occurred due to the handling of the spermatic cord, which required pressure dressings for it to subside.
Clinical Photograph of the picture
X-ray Pelvis Ap view showing the lesion

MRI showing a cystic swelling with intraabdominal extension and compression of urinary bladder
Intra-operative photograph showing aspiration of the haematogenous fluid from the swelling

Picture showing the cavity in the bone
The patient came for follow up after 10 days, one month and sixmonths and he is doing fine, without any previous complaints. Now the activity in the pubis has healed, with no evidence of recurrence and the patient is doing well and is able to squat and sit cross legged [Table/Fig-1,Table/Fig-2,Table/Fig-3,Table/Fig-4,Table/Fig-5,Table/Fig-6andTable/Fig-7].
Discussion
Aneurysmal bone cysts are aggressive lesions with a potential for rapid growth and destruction of the bone, with a risk of pathologic fractures and high rates of local recurrence [2,10–13]. An aneurysmal bone cyst may be a primary bone lesion or it may occur as a secondary lesion in other tumours [2]. The average duration of the symptoms until diagnosis was six months [3,5,6,8]. In this study, we faced an average delay of 8 months before the diagnosis was established.
The method of treatment of an aneurysmal bone cyst of the pelvis must be individualized, depending on the location, aggressiveness and extent of the lesion. The treatment options include complete resection of the lesion, simple curettage, curettage and bone grafting, selective arterial embolization (primary treatment or preoperative adjuvant therapy) and a percutaneous injection of a fibrosing agent. Yildirim et al., [14] reported their experiences with aneurysmal bone cysts of the adult pelvis. Lesions which are less than 5 cm, that exhibit minimal destruction or expansion of cortical bone and don’t threaten the integrity of acetabulum or the sacroiliac joint, are best treated with intra-lesional curettage, with or without the use of bone grafts. Lesions which are greater than 5 cm, which exhibit large areas of destruction or major expansion of the cortical bone and which threaten the integrity of the acetabulum or the sacroiliac joint require more aggressive treatment with the use of the excision or curettage technique.
Tissues excised out of the lesion their approx sizes and fluid aspirated out of the lesion

Histologic pictures of ABC showing gaint cells

Schwering et al., [15] described the successful management of a large iliac aneurysmal bone cyst with the use of cystoscopic controlled curettage. Chemical cauterization with phenol is recommended for the relatively large primary lesions, to kill any surface tumour cells which are present in the curetted cavity. Cryotherapy has also been proposed as an adjuvant therapy, with surgical treatment, to achieve a local control. Radiation is used in inaccessible sites where no surgical options are available, but it has high recurrence rates. Recently, the percutaneous injection of a fibrosing agent has been employed in the treatment of aneurysmal bone cysts. This technique is often associated with high complication rates and it is also expensive. Selective arterial embolization is currently recommended as the procedure of choice for lesions whose sites or sizes make other types of treatment difficult or dangerous. It is especially useful for managing huge lesions which pose a surgical risk due to intra-operative bleeding and the surrounding neural structures. Its cost and availability, however, preclude its use in developing countries.
The adequacy of surgical resection plays an important role in avoiding a recurrence. The surgical approach which is chosen is important, and a wide surgical exposure that allows adequate visualization for a complete excision of the tumour is advised [6]. Management of a superior ramus pubic aneurysmal bone cyst is surgically demanding, because of the tendency of an intra-operative bleeding, owing to the massive size of the highly vascular tumour and the relative inaccessibility of its deeper extensions into the adjacent ischium and the intra-abdominal extension of the lesion. Since aneurysmal bone cysts are usually easily eradicated by curettement, irradiation should ordinarily be reserved for the inaccessible lesions.
A long-term follow-up is necessary, so as to ensure that no deformity develops. Extensive pre-operative planning, with use of advanced imaging to determine the extent of the lesion, is one of the important steps in the management of aneurysmal bone cysts of the pubis. A wide surgical approach is crucial, for allowing a complete exposure and excision of the lesion. No clinical deformity was observed at six months of follow-up. We believe that these surgical principles yield satisfactory results with a low rate of local recurrence and complications during the surgical excision and also after surgical treatment of aneurysmal bone cysts of the pubis.
[1]. Jaffe HL, Lichtenstein L, Solitary unicameral bone cyst with emphasis on the roentgen picture, the pathologic appearance and the pathogenesisArch Surg 1942 44:1004-25. [Google Scholar]
[2]. Vergel De Dios AM, Bond JR, Shives TC, McLeod RA, Aneurysmal bone cyst. A clinicopathologic study of 238 casesCancer 1992 69:2921-31. [Google Scholar]
[3]. Biesecker JL, Marcove RC, Huvos AG, Mike V, Aneurysmal bone cysts- A clini-copathologic study of 66 casesCancer 1970 26:615-25. [Google Scholar]
[4]. Clough JR, Price CH, Aneurysmal bone cyst: pathogenesis and long term results of treatmentClin Orthop Relat Res 1973 97:52-63. [Google Scholar]
[5]. Beiner JM, Sastry A, Berchuck M, Grauer JN, Kwon BK, An aneurysmal bone cyst in the cervical spine of a 10-year-old girl: a case reportSpine 2006 31:475-9. [Google Scholar]
[6]. Giddings CE, Bray D, Stapleton S, Daya H, Aneurysmal bone cyst of the spineJ Laryngol Otol 2005 119:495-7. [Google Scholar]
[7]. Khalil IM, Alaraj AM, Otrock ZK, Chamoun RB, Sabbagh AS, Aneurys-mal bone cyst of the cervical spine in a child: case report and review of the surgical roleSurg Neurol 2006 65:298-303. [Google Scholar]
[8]. Pennekamp W, Peters S, Schinkel C, Kuhnen C, Nicolas V, Aneurysmal bone cyst of the cervical spine (2008:7b)EurRadiol 2008 18:2356-60. [Google Scholar]
[9]. Perlmutter DH, Campbell S, Rubery PT, Vates EG, Silberstein HJ, Aneurysmal bone cyst: surgical management in the pediatric cervical spineSpine 2009 34:50-3. [Google Scholar]
[10]. Capanna R, Albisinni U, Picci P, Calderoni P, Campanacci M, Aneurysmal bone cyst of the spineJ Bone Joint Surg Am 1985 67:527-31. [Google Scholar]
[11]. MacCarty CS, Dahlin DC, Doyle JB Jr, Lipscomb PR, Pugh DG, Aneurysmal bone cysts of the neural axisJ Neurosurg 1961 18:671-7. [Google Scholar]
[12]. Radanović B, Simunić S, Stojanović J, Orlić D, Potocki K, Thera- peutic embolization of aneurysmal bone cystCardiovascIntervent Radiol 1989 12:313-6. [Google Scholar]
[13]. Ruiter DJ, Van Rijssel TG, Van der Velde EA, Aneurysmal bone cysts: a clinico-pathological study of 105 casesCancer 1977 39:2231-39. [Google Scholar]
[14]. Yildirim E, Ersözlü S, Kirbas I, Özgür AF, Akkaya T, Karadeli E, Treatment of pelvic aneurysmal bone cysts in two children: selective arterial embolization as an adjunct to curettage and bone graftingDiagn Interv Radiol 2007 13:49-52. [Google Scholar]
[15]. Schwering L, Uhl M, Herget GW, Iliac aneurysmal bone cyst treated by cystoscopic controlled curettage. SICOT Online reports E054 [Google Scholar]