Osteochondroma of the OsCalcaneum- A Case Report
Ashok Kumar Patnala1, M. Eswara Babu2, M. Chandrasekharam Naidu3, S Shyam Kumar4, P. Varun Kumar5
1 Associate Professor, Department of Orthopaedics,Andhra Medical College, King George Hospital, Visakhapatnam ,Andhra Pradesh, India.
2 Professor, Department of Orthopaedics,Andhra Medical College, King George Hospital, Visakhapatnam ,Andhra Pradesh, India.
3 Assistant Professor, Department of Orthopaedics,Andhra Medical College, King George Hospital, Visakhapatnam ,Andhra Pradesh, India.
4 Junior Resident, Department of Orthopaedics,Andhra Medical College, King George Hospital, Visakhapatnam ,Andhra Pradesh, India.
5 Junior Resident, Department of Orthopaedics, Andhra Medical College, King George Hospital, Visakhapatnam ,Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORESPONDING AUTHOR: Dr. Ashok Kumar Patnala, Associate Professor, Department of Orthopaedics, King George Hospital, Visakhapatnam–530002, India.
Phone: 9849123602,
E-mail: ashok_ortho59@rediffmail.com
Osteochondromas are common benign bone tumours. They usually occur in the patients who are below thirty years of age. They probably are developmental malformations rather than true neoplasms. They are believed to originate within the periosteum as small cartilaginous nodules. The foot is rarely a common site of presentation for these tumours. The calcaneum is one of the most unusual regions for the occurrence of osteochondromas 1. The osteochondromas which arise from the calcaneum, especially those which project onto the plantar surface, pose considerable problem to the ambulation. Malignant transformations are seen in less than 1% to 2% of the patients with solitary osteochondromas 2. We herewith present a case of osteochondroma which arose from the calcaneum, which was surgically excised to improve the patient’s daily functioning. The patient was followed up for a period of one year. She is now able to walk comfortably.
Osteochondroma, Calcaneum
Introduction
Osteochondromas are the most common benign osseous neoplasms. These tumours originate from the physis and they are covered by distinct hyaline cartilaginous caps. They mostly involve the metaphyseal or the metadiaphyseal regions of the long bones. They rarely develop in the feet. The osteochondromas of the feet are mostly seen in the short tubular bones such as the metatarsal bones and the phalanges. They are seldom found in the calcaneum. We are reporting a rare case of an osteochondroma which involved the calcaneum, that was managed by doing a surgical excision.
Osteochondromas or exostoses are abnormal growths of the cartilage on the surface of bone, which are inherited as an autosomal dominant trait. Some have multiple exostoses that carry a more significant risk of a malignant transformation [1]. Less than 1% of the osteochondromas involve the tarsal bones [2]. Calcaneal osteochondromas are extremely rare. The patients may either present with asymptomatic masses or with multiple exostoses. The osteochondromas are usually asymptomatic, and they are seen incidentally on radiography [3].
Osteochondromas are seen in 2% to 3% of the general population and they represent approximately 36% to 41% of the cases with benign bone tumours [4]. About 60% of these occur in the patients who are below 30 years of age and about 63% of the patients are males [2]. Plane radiographs are usually sufficient to make a diagnosis. The radiographic features include a continuous cortex with a medullary cavity that flows into the lesion. The bone scanning is directly correlated with the degree of enchondral bone formation [5]. The lesion’s cap has a smooth subchondral cortex and a homogenous appearance. The cap bone destruction or mineralization which extends from the cap, may indicate a malignant transformation into a chondrosarcoma. Extension of the cap to greater than 2 cm on histological examination may indicate a malignant transformation, because it is usually not more than 2 mm to 3 mm thick. Ultrasonography can be used in the measurement of the hyaline cartilage cap thickness [3].
Case Report
We are reporting a case of osteochondroma of the calcaneum in a 30 year old female who presented with the complaints of pain and a difficulty in walking of four years duration. The patient was a house wife who had considerable difficulty in carrying out her day to day activities due to the swelling which arose on the plantar surface of her left foot. There was no preceding history of any trauma. There was no history of fever during the entire period of her presentation. There was no incidence of any spontaneous regression during the entire course of the events. On clinical examination, she was found to have multiple swellings which mostly involved the long bones. These swellings resulted in long bone deformities. She was symptomatic only on the involved side. No other members in her family had similar presentations. We did a radiographic evaluation and an MR imaging of the involved extremity. X–ray showed an irregular, sessile mass which was about 6 cm x 3 cm in size, which arose from the plantar surface of the calcaneum [Table/Fig-1]. The lesion was sclerotic, with lytic areas in between. Due to the persistent nature of the symptoms, which could not be relieved by a conservative management alone, the patient was offered surgery in view of the duration and the severity of her symptoms. In our case, the patient presented with multiple exostoses which involved most of the long bones in her body. These multiple swellings had resulted in growth disturbances like short stature and deformed extremities. She had a huge osteochondroma of size, 6.5 x 6.5 cm over the plantar surface of her left heel. A surgical option of management was chosen in view of the difficulty which the lesion caused her in carrying out her daily activities.
Pre – Operative X–ray of the foot with ankle showing the lesion arising from the plantar surface of the calcaneum

Procedure
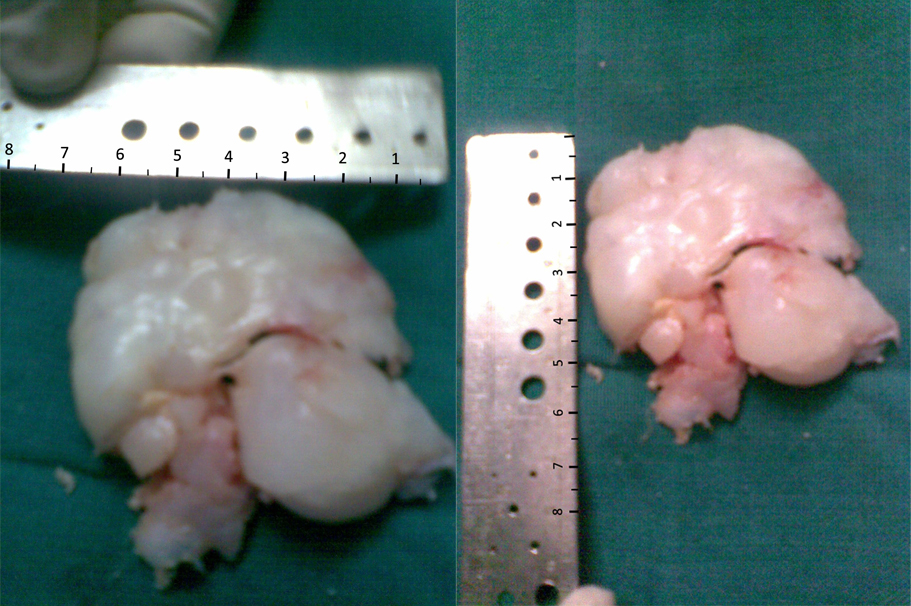
Through a Cincinnati incision, the tumour was excised, along with the cartilaginous cap and the specimen was sent for a histopathalogical examination [Table/Fig-2]. The histopathalogical reports confirmed the diagnosis of a osteochondroma. The histological examination showed the presence of a cartilaginous cap which was less than 1cm thickness and an overlying bursa which contained osteocartilagenous loose bodies. The benign nature of the lesion was confirmed by the thickness of the cartilaginous cap, which was less than 2 mm. The patient was followed up for a period of one year and there were no clinical or radiological signs which were suggestive of a recurrence. The patient showed significant improvement in her daily functional activities.
Tumour mass being measured following excision from the calcaneum
Discussion
Osteochondromas are developmental lesions rather than true neoplasms and they may occur as solitary or multiple lesions which are associated with the syndrome of multiple hereditary exostoses. The tumours of the hand and feet bones, which include those of the calcaneum, constitute only of 10% the osteochondromas [6]. Cartilage cap thicknesses of greater than 1 to 2 cm in adults and of 2 to 3 cm in growing children suggest a malignant transformation [7]. In the study of Kinoshita et al., among 83 cases of bone and soft tissue tumours of the foot, osteochondroma was the most commonly reported benign tumour. They reported a more common occurrence of the tumour in females who were under the age of 19 years. Radiologically, these tumours can be either sessile or pedunculated. A histological examination of the cartilaginous cap is suggestive of a malignant transformation, if it is more than 2 cm thick. Malignant transformations are seen in less than 1% to 2% of the patients of solitary osteochondroma and in 5%–25% of the patients with multiple hereditary exostoses. Although radiography alone is often diagnostic, other imaging modalities may be necessary for the surgical planning and to exclude a sarcomatous degeneration. MR imaging is the best radiologic imaging method for evaluating the hyaline cartilage cap. The mineralized areas in the cartilage cap had a low signal intensity on the T1 and T2–weighted images [8, 9].
The multiplanar reconstruction and the three–dimensional imaging features of CT give important information about these lesions [Table/Fig-3]. The treatment of the osteochondromas of the foot can be either conservative or surgical excisions. The size and the nature of the lesion generally guide the optimal treatment. The small, asymptomatic lesions are usually managed conservatively [10]. If the lesion is painful and if it is growing after the attainment of the skeletal maturity, or if it exhibits the signs of a malignant transformation, it should be treated surgically [Table/Fig-4 & 5]. A marginal resection is adequate and it shows a low rate of recurrence [11]. The histological findings serve as guides for assessing the risk of a recurrence, as was recommended by Blitz et al., in his case series. In their case series, the cartilaginous cap thickness proved to be the most important determinant of the risk of the malignancy. Though the lesion was sessile, which was a predictor of the malignant outcome in our case, there was no incidence of any changes which were suggestive of a malignancy during the entire course of the follow up. Karasick et al., determined the importance of the excision of these tumours when there are signs which are suggestive of an increased risk of malignancy like the sessile lesions, as in our case. Nogier et al., suggested the need of a surgical intervention (excision) for these tumours, for relief from the pain. In our case, the patient was relived of her pain following a surgical excision and there was a significant improvement in her functional status following her surgery.
Pre - operative 3D CT image of the foot showing the lesion over the plantar aspect of the calcaneum

Pre-operative clinical picture showing the tumour mass over the heel region

Intra operative image following excision of the tumour

Conclusion
Osteochondromas of the skeleton are common in the age group of thirty years, but osteochondromas which involve the calcaneum are relatively rare presentations. Most of the cases take a benign course, but the giant osteochondromas, as in our case, may undergo malignant transformations, according to the literature. Any cartilage cap which remains, following a surgical excision, may result in a recurrence; especially in the growing lesions. It is therefore necessary to manage these lesions through an appropriate, surgical, timely intervention, to prevent a malignant transformation.
[1]. Blitz NM, Lopez KT, Giant solitary osteochondroma of the inferior medial calcaneal tubercle: A casereport and review of the literatureJ Foot Ankle Surg 2008 47:206-12. [Google Scholar]
[2]. Karasick D, Schweitzer ME, Eschelman DJ, Symptomatic osteochondromas: imaging featuresAJR Am J Roentgenol 1997 168:1507-12. [Google Scholar]
[3]. Malghem J, Vande Berg B, Noel H, Maldague B, Benign osteochondromas and exostoticchondrosarcomas: evaluation of cartilage cap thickness by ultrasoundSkeletal Radiol 1992 21:33-37. [Google Scholar]
[4]. Griffiths HJ, Thompson RC Jr, Galloway HR, Everson LI, Suh JS, Bursitis in association with solitary osteochondromas presenting as mass lesionsSkeletal Radiol 1991 20:513-16. [Google Scholar]
[5]. Glassman SB, Delbeke D, Nuclear medicine case of the day: hereditary multiple exostosesAJR Am J Roentgenol 1992 158:1384 [Google Scholar]
[6]. Nogier A, De Pinieux G, Hottya G, Anract P, Case reports: enlargement of a calcaneal osteochondroma after skeletal maturityClin Orthop Relat Res 2006 447:260-66. [Google Scholar]
[7]. Woertler K, Lindner N, Gosheger G, Brinkschmidt C, Heindel W, Osteochondroma: MR imaging of tumor-related complicationsEur Radiol 2000 10:832-40. [Google Scholar]
[8]. Lee JK, Yao L, Wirth CR, MR imaging of solitary osteochondromas: report of eight casesAJR Am J Roentgenol 1987 149:557-60. [Google Scholar]
[9]. De Beuckeleer LH, De Schepper AM, Ramon F, Magnetic resonance imaging of cartilaginous tumors: is it useful or necessary?Skeletal Radiol 1996 25:137-41. [Google Scholar]
[10]. Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH, Imaging of osteochondroma: variants and complications with radiologic-pathologic correlationRadiographics 2000 20:1407-34. [Google Scholar]
[11]. Al Klin DPM, Subungual osteochondroma or exostosis cartilaginea of the hallux: A case report of recurrent bone tumor one year laterThe Foot and Ankle Online Journal 2010 3(2):2 [Google Scholar]