Pain relief is an important part of post-operative care of the patients who undergo any type of surgery. Patients deserve to be as pain free as possible. In addition to patient’s comfort, one of the important reasons for good pain management is that the patient needs to participate fully in post-operative rehabilitation like deep breathing, coughing and ambulation, as all these help in preventing unwanted complications [1]. Chronic post thoracotomy pain has highest incidence and therefore it needs attention. Chronic post thoracotomy pain is defined by the International Association for the Study of Pain as ‘a pain that recurs or persists along a thoracotomy incision, at least two months following a surgical procedure’ [2]. Usually, it is burning, dysaesthetic and aching in nature, which displays many features of neuropathic pain. It occurs in approximately 50% of patients after thoracotomy and is usually mild or moderate. However, in 5%, the pain is severe and disabling. No one technique of thoracotomy has been shown to reduce the incidence of chronic post thoracotomy pain [3].
The first reference to Chronic Post-thoracotomy Pain (CPP) was made in 1944 by United States Army surgeons who noted ‘chronic intercostal pain’ in men who had undergone thoracotomies for chest trauma during the Second World War. They identified the serious problem of chronic pain and the subsequent difficulty in getting rehabilitated and returning to duty [4]. CPP is one of the most challenging conditions which physicians confront. Different strategies have been described to reduce acute and chronic post-thoracotomy pain. These include non steroidal anti-inflammatory drugs, parenteral opiates, epidurals and paravertebral infusions of local anaesthetics, narcotics, intrapleural analgesia, transcutaneous nerve stimulation, intercostal and phrenic nerve blockades and cryotherapy [5]. However, the results were variable and no single strategy was shown to be effective in all patients.
Pregabalin, like gabapentin, is an amino acid derivative of gamma-amino butyric acid (GABA analogue). Both agents have been shown to be effective for neuropathic pain disorders. It has been observed that Pregabalin provides equivalent efficacy as compared to gabapentin, at much lower doses, because it has a much higher bioavailability (90% versus 33-66%) and is rapidly absorbed (peak: 1 hour). Also, its plasma concentration increases linearly with increasing doses. This is not true with gabapentin. We administered PREGABALIN (Dayanand Medical College and Hospital, Ludhiana, India) an anti-convulsant, to patients who underwent posterolateral thoracotomies. There is no study which has shown the effect of pregabalin in CPP. But its role in post-hernia repair was shown by one study.
Material and Methods
After getting approval from institutional thesis ethical committee, this study was conducted in the department of Surgery, DMCH, on 50 consenting patients who underwent thoracotomies.
Inclusion Criteria
Those with ages which were greater than 18 years and less than 70 years and those who underwent elective thoracotomies for primary thoracic surgeries.
Exclusion Criteria
Inability to adhere to study protocol
Intolerance or hypersensitivity to Pregabalin or Diclofenac
Contraindication to a thoracic epidural catheter placement
A previous ipsilateral or bilateral thoracotomy
Surgery for tumour which extended into the chest wall
Rest pain in proposed surgical area pre-operatively
A H/o substance abuse
A H/o chronic steroid use
H/O pre-existing (no space in H/O) chronic pain which required chronic analgesic use
A H/o a seizure disorder which required treatment with an anticonvulsant
A H/o current therapy with thiazolidinedione class oral hypoglycaemic agents
A H/o a major psychiatric disorder
The patients who fulfilled all inclusion criteria and none of the exclusion criteria were randomized to Group A (Pregabalin recipients) or Group B (Non-recipients).
In Group A, Pregabalin 150 mg was given one hour prior to the administration of general anaesthesia. Post-operative pain was recorded and quantified by using VAS. A second dose of pregabalin was given 12 hours after surgery and then, once daily for a total of 21 days. In Group B, patients were managed postoperatively by giving Diclofenac Sodium 75mg 8 hourly for first 7 days and then, on demand, as was required by the patient.
Escape treatment, in the form of Diclofenac sodium 75mg tablet, was also given to Group A patients, who had no pain relief after pregabalin ingestion [Table/Fig-1,Table/Fig-2].
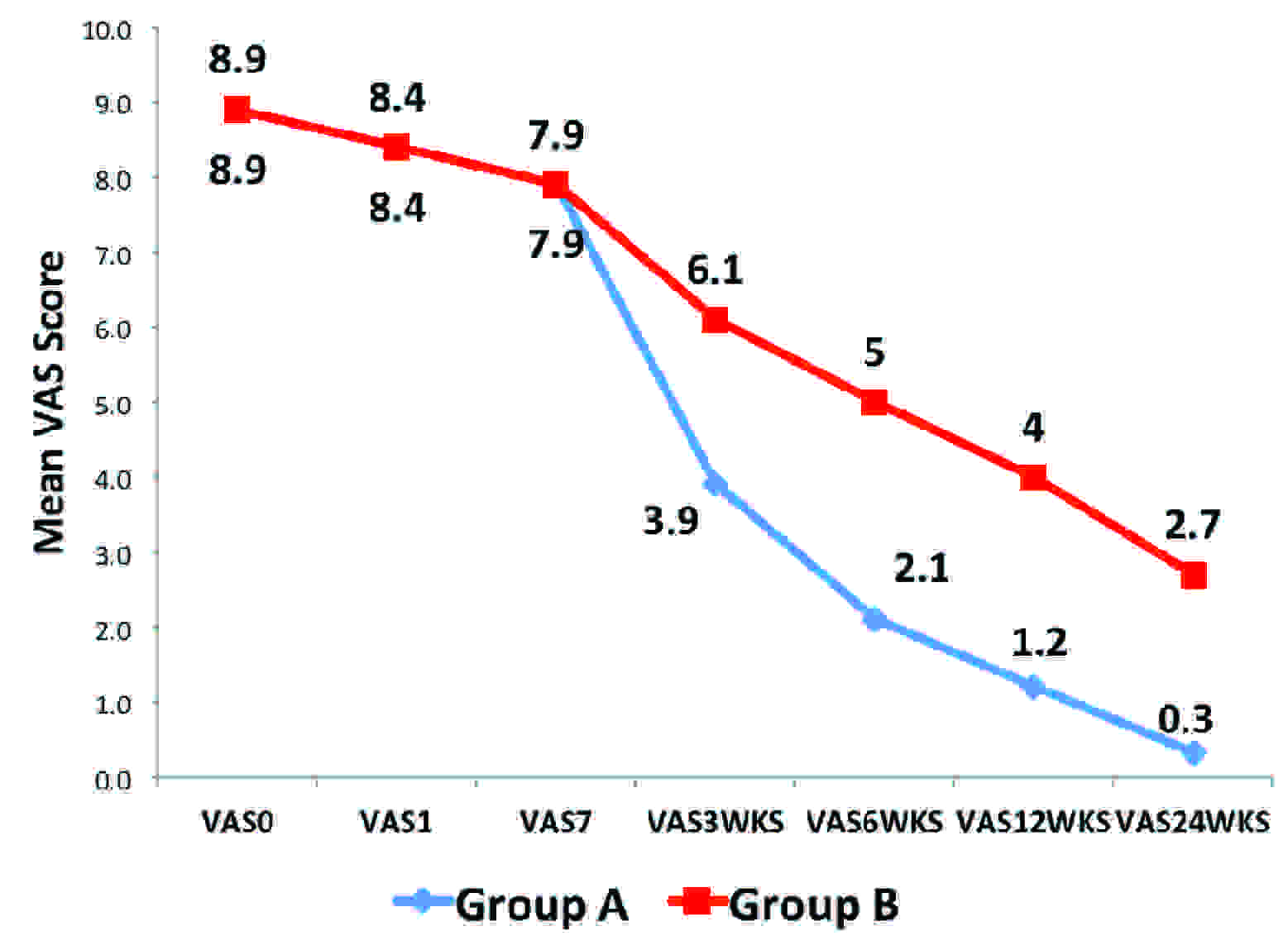
Distribution of Study Subjects According to VAS
| Vas Score | Mean (S.D.) | t- test | p value* |
|---|
| Group A | Group B |
|---|
| VAS0 | 8.9 (2.7) | 8.9 (2.7) | 0 | 1, NS |
| VAS1 | 8.4 (2.7) | 8.4 (2.7) | 0 | 1, NS |
| VAS7 | 7.9 (1.5) | 7.9 (1.5) | 0 | 1, NS |
| VAS3WKS | 3.9 (2.6) | 6.1 (2.4) | 3.20 | 0.0025, S |
| VAS6WKS | 2.1 (1.8) | 5.0 (2.1) | 5.24 | 3.5 X 10-6, HS |
| VAS12WKS | 1.2 (1.0) | 4.0 (2.1) | 6.01 | 2.3 X 10-7, HS |
| VAS24WKS | 0.3 (0.7) | 2.7 (1.8) | 6.21 | 1.2 X 10-7, HS |
*NS: Non-Significant; S: Significant; HS: Highly Significant
Distribution of Study Subjects According to VAS
While in the hospital, patients were assessed for pain intensity by VAS and number of Diclofenac tablets which were ingested. At follow-up, patients were re-assessed at 1 week, 3 weeks, 6 weeks, 12 weeks and 24 weeks.
Observations and Tables
In this randomized prospective study which was done from January 2011 to December 2012, 50 consenting patients of thoracotomy, who were admitted to Department of Surgery, Dayanand Medical College and Hospital, Ludhiana, were studied. Each patient was evaluated and following observations were made.
The pain VAS scores in group A were significantly low at all observation points except on day 0, day 1 and day 7 post-operatively, when the differences in pain scores in both the groups were comparable. The overall pain scores of Group A were comparable at day 0, day1 and at day 7 as compared to those of Group B. (p>0.9) Pain was significantly low at three weeks (p<0.05). Pain scores of Group A were significantly low at 6 weeks,12 weeks and 24 weeks as compared to those of Group B (p<0.001) and the difference was statistically significant [Table/Fig-3]. Number of diclofenac tablets which were ingested (escape treatment), which were required during the study period in Group A were significantly low as compared to those of Group B (p<0.001) and the differences in both the groups were statistically significant.
Distribution of Study Subjects According to Escape Treatment
| Follow up | Mean (S.D.) | t- test | p value* |
|---|
| Group A | Group B |
|---|
| No. of diclofenac tablets (escape treatments) | 10.3 (3.2) | 51.9 (17.3) | 11.85 | <0.001, HS |
*HS: Highly Significant.
Discussion
Pain relief is an important part of postoperative care of the patients who undergo any surgery. Intercostal nerve involvement is the most important reason behind severe wounds and neuropathic pain in chronic post thoracotomy pain [6]. Recently, attention was focused on the potential role of anticonvulsants in post-herpetic neuralgia and other neuropathic pain syndromes [1,7]. In two studies which were done on painful diabetic neuropathy [8] and post herpetic neuralgia [9], gabapentin was reported to produce significant pain relief as compared to placebo, and a significant improvement in measures of quality of life and mood [10].
Sihoe et al., investigated the effectiveness of gabapentin for post-operative and post-traumatic pain in thoracic surgery patients and reported a decrease in pain and chest wall paresthaesia in 73.3% and 75% of patients, respectively [11].
Gabapentin is slowly absorbed (peak: 3 to 4 hours post-dose) and more importantly, its plasma concentrations have been found to have a non-linear relationship to increasing doses. Thus, Pregabalin has been found to have distinct pharmacokinetic advantages over gabapentin [12].
Perioperative Pregabalin administration reduces early postsurgical pain at rest and particularly, during movements after major spine surgeries which are done with less opioid consumption and it seems to influence the improvement of overall quality of life three months after surgery [13].
50 consenting patients who were planned for thoracotomy, who were of variable ages and of either sex were selected and randomly allocated into two groups. GROUP A: Study group of 25 patients received Pregabalin postoperatively for 21 days and diclofenac was given on demand as escape treatment. GROUP B: Control group of 25 patient received only diclofenac on demand. Patients were randomized according to age, sex, presentation and type of surgery which was done. VAS was used for the assessment of postoperative pain on 0, 1 and 7 days and at 3, 6, 12 and 24 weeks.
Mean visual analogue pain scores (VAS) in Group A and in Group B were comparable in both the groups on 0, 1 and 7 days and the difference was not statistically significant. This could be explained by the fact that in the immediate post-operative period, both the groups had epidural catheters in situ. So, both the groups had same pain scores at day 0 and day 1. The pain scores were also comparable on day 7. This could be explained by the fact that Pregabalin is not effective for acute pain i.e. immediately in postoperative period.
Very significant differences were seen when VAS scores were calculated between Groups A and B, between 3, 6, 12 and 24 weeks (p<0.001), between 0 and 3 weeks (p<0.001), between 0 and 6 weeks, between 0 and 12 weeks and between 0 weeks and 24 weeks (p<0.001), but non significant results were obtained between 0, 1 and 7 days.
VAS decreased gradually in both the groups over a period of 24 weeks. Mean VAS was 0.3 in Group A as compared to 2.7 in Group B. The pain decreased in both the groups over a period of time, with VAS significantly decreasing in study Group (pregabalin recipients). This may be because of the subsiding inflammation with passage of time. The number of diclofenac tablets which were consumed by Group A were very less (10.3) as compared to those which were consumed by Group B (51.9) and the difference was highly significant. This could be explained by the fact that pregabalin prevents the chronic pain in thoracotomy patients. Our results correlated well with the observations of Okan Solak et al. The mean VAS score before the treatment (VAS0) was 6.4 ±0.6 for Gabapentin. VAS scores at days 0, 15, 30, 45 and 60 were compared within each group, to determine the decrease in wound pain. In the Gabapentin group, there was significant amelioration of wound pain (p = 0.001). On the 60th day of treatment, 17 (85%) patients of the Gabapentin group were found to have VAS scores of <5 (p = 0.001) [14].
There are no reports on treatment with Pregabalin for pain after thoracic surgeries. A small study which was done on 4 patients by Matsutani N et al. showed significant improvement of chronic pain after taking Pregabalin after thoracotomies [15].
In our study, we observed that pregabalin was safe and efficacious in the treatment of chronic post thoracotomy pain. All patients could tolerate pregabalin, as none of the patients had any adverse drug reactions/treatment stopped. This may be because of very small dose of pregabalin. In our study, minor side effects did not cause discontinuation of the treatment, in comparison to the findings of a study which was done by Sihoe et al. They reported the rate of minor side effects as 40% in their study [11]. Sihoe et al., administered gabapentin after thoracotomies and thorax trauma for a mean duration of 21.9 weeks [11]. However, as this was a small study, it needs verification by doing large, randomized control trials.
Conclusion
Pregabalin is an effective and a safe adjuvant for reducing chronic post thoracotomy pain, without significant side effects, in all age groups and either gender. The pain relief becomes statistically significant after three weeks of treatment and it continues till six months. However, larger randomized and placebo-controlled trials of longer durations are required to further validate these findings.
*NS: Non-Significant; S: Significant; HS: Highly Significant
*HS: Highly Significant.