A Comparative Study of Lipid Profile and Oestradiol in Pre- and Post-Menopausal Women
Srinivas Reddy Kilim1, Srinivasa Rao Chandala2
1 Associate Professor, Depatment of Physiology, Rangaraya Medical College, Kakinada-533003, Andhra Pradesh, India.
2 Associate Professor, Department of Physiology, Siddhartha Medical College, Gunadala, Vijayawada-520 008 Andhra Pradesh, India.
NAME, ADRESS, E-MAIL ID OF THE CORESPONDING AUTHOR: Dr. Srinivas Reddy Kilim, Associate Professor, Depatment of Physiology, Rangaraya Medical College, Kakinada-533003, Andhra Pradesh, India.
E-mail: drvasuk@yahoo.com
Objectives: To investigate the relationship between the menopausal status and related hormonal variation of oestradiol with plasma lipid concentrations.
Material and Methods: Fifty premenopausal women and fifty postmenopausal women subjects were selected. Data was collected through clinical evaluation from questionnaires and laboratory investigations. Plasma oestradiol and lipid profile determinations were done by using competitive binding immunoassay methods and enzymatic methods respectively. Student’s T test and Pearson’s test of correlation were used for the statistical analysis. P-values of < 0.05 were considered to be statistically significant.
Results: There was a significant increase in serum Total Cholesterol (TC), Triglycerides (TG), LDL-cholesterol and VLDL-cholesterol levels in post-menopausal women. HDL-cholesterol level was significantly decreased in post-menopausal women. The calculated atherogenic index (Total Cholesterol/HDL ratio) was significantly increased in post-menopausal women as compared to that in premenopausal women. Oestradiol concentration was significantly lower (p<0.001) in post-menopausal women.
Discussion: Oestrogen changes the vascular permeability by increasing nitrous oxide production. It maintains a healthy lipoprotein profile. It stabilizes the endothelial cells, enhances antioxidant effect and alters fibrinolysis protein. All these cardioprotective mechanisms are lost in menopause. Postmenopausal women develop an increased risk for cardiovascular disease.
Conclusion: Menopause leads to changes in lipid profile by reducing HDL, and elevating Total Cholesterol (TC), triglycerides (TG), LDL-cholesterol and VLDL-cholesterol, thus increasing the risk for cardiovascular disease. These changes are caused by reduced oestrogen concentrations which are seen in menopause.
Menopause, Oestrogen, Cardiovascular disease, Plasma lipids, Coronary heart disease
Introduction
Studies have shown that women are at a lesser risk of developing cardiovascular disease than their male counterparts before menopause, but this advantage is abolished after menopause [1,2].Data from the Framingham Study suggest that female coronary heart disease (CHD) morbidity rates accelerate more quickly than do those of males after the age of 45 years [3].
Menopause is the permanent cessation of menstruation; it occurs at a mean age of 51 years. Menopause literally refers to the last menstrual period. The exact time of menopause is usually made in retrospect; that is, 1 year without menses [4]. A woman today, will live approximately for about a third of her life, beyond the menopause. After menopause, the ovaries cease to produce significant amounts of oestrogen; therefore, symptoms and diseases which are associated with oestrogen deficiency are of increasing importance to women’s health [5].
The incidence of cardiovascular disease after menopause may be partly caused by changes in the plasma lipid levels that occur following the menopausal transition [6–8]. Low-density lipoprotein has been implicated in the development of Coronary Heart Diseases (CHD). Deposition of fatty plaques on arterial walls (arteriosclerosis) is a predisposing factor for CHD [9].
Despite the extensive research on the effects of oestrogens and progestagens on lipid and lipoprotein metabolism [10,11] it is not yet clear whether changes in sex steroid concentrations are related to changes in lipid concentrations, which are associated with menopausal status. Coronary Artery Disease (CAD) is clearly polyfactorial, and data on endogenous hormones may improve our prediction of CAD [12].
Our study aimed to establish differences in lipid status in women who were in menopause and in women who underwent regular menstruation and to investigate the relationship between the menopausal status and related hormonal variation with plasma lipid concentrations.
Material and Methods
In this present study, groups of fifty premenopausal women and fifty postmenopausal women were randomly selected .The postmenopausal women who were studied were those with a history of natural menopause, who had cessation of menstruation for a minimum of one year, and premenopausal women who were studied were those who had regular menstruation.
Subjects with cardiovascular disease, hypertension, diabetes mellitus, hepatic, metabolic and renal disease, and those who were on exogenous hormones or on hormone replacement therapy, or lipid lowering drugs, were excluded from the study. In the assessment protocol, the daily eating and physical activity patterns were noted. To minimize the effect of life style on lipid profile, smokers, alcoholics, sedentary women and trained athletes or sports persons were excluded from the study.
The study was approved by the institutional ethics committee. After getting their informed consents, venous blood samples were collected from subjects after an overnight fasting of 12-14 hours. This however, was done on the 7th day of the last menstrual period for the premenopausal group. Samples were centrifuged, plasma was separated and it was used for analysis. The total cholesterol, triglyceride and HDL were estimated by an enzymatic method and serum LDL and VLDL were calculated by using Friedewald’s formula LDL = TC - HDL - TG/5.0 (mg/dL) [13]. Oestradiol was determined by using an Enzyme Linked-Immuno-Sorbent Assay kit, which is a competitive binding immunoassay for the quantitative determination of 17-beta–oestradiol. Body Mass Index (BMI), as a measure of body fat was determined, based on height and weight of Pre-and Post-menopausal women. Measurements of waist circumference on the narrowest area and hip circumference on the widest area, were made. Thewaist-hip ratio was calculated, according to this formula: WH ratio = waist circumference (cm)/hip circumference (cm). Calculated values were processed by using: arithmetic mean, standard deviation, Student’s ‘t’ test and Pearson’s test of correlation. p-values of < 0.05 were considered to be statistically significant.
Results
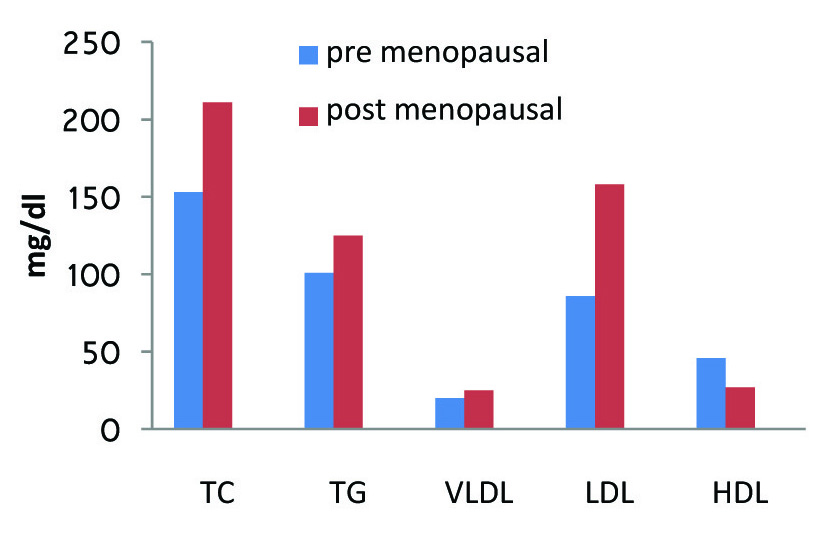
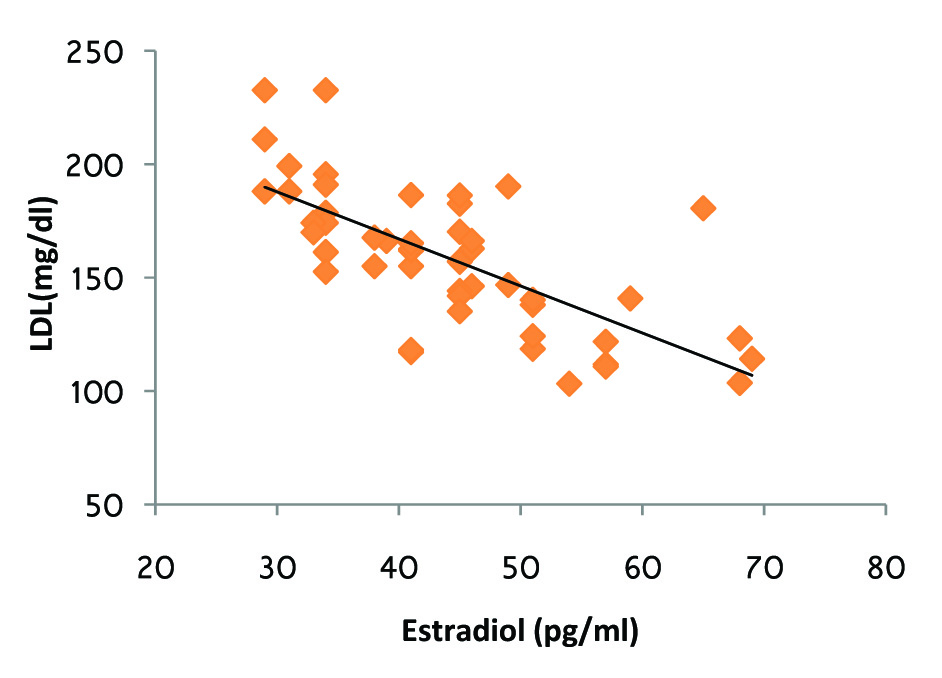
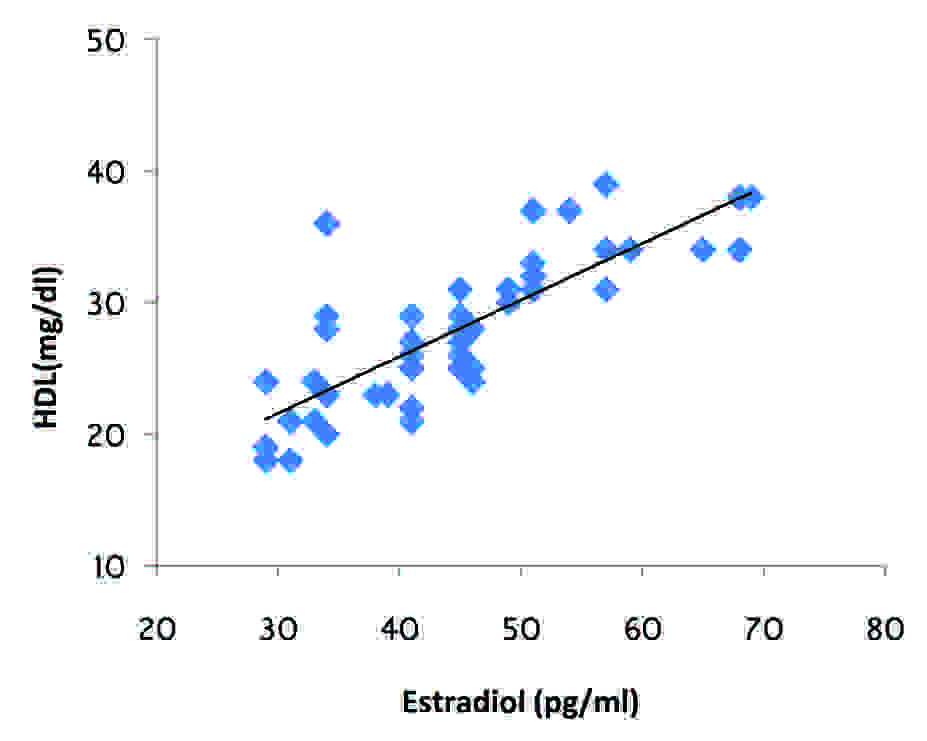
In our study, we observed a significant increase in serum Total Cholesterol (TC), Triglycerides (TG), LDL-cholesterol and VLDL-cholesterol level in post-menopausal women as compared to those in pre-menopausal women (p<0.001). HDL-cholesterol level was significantly decreased in post-menopausal women as compared to that in pre-menopausal women (p<0.001).The calculated atherogenic index (Total Cholesterol/HDL ratio) significantly increased in post-menopausal women as compared to that in premenopausal women (p<0.001). The oestradiol concentration was significantly lower (p<0.001) in post-menopausal women [Table/Fig-1,2]. According to the results of this research, there was no significant difference in BMI and WHR [Table/Fig-3] between postmenopausal women and pre-menopausal women (p>0.05). The concentration of oestrogen showed a negative correlation with TC, TG, LDL [Table/Fig-4] and VLDL while its correlation with HDL concentration was positive [Table/Fig-5].
Comparison of plasma lipids in Premenopausal and Postmenopausal Women
| Plasma lipids | Pre-menopausal n=50 | Post-menopausal n=50 | P-Value |
|---|
| TC | 153.38 ± 17.44 | 211.24 ± 29.58 | < 0.001 |
| TGL | 101.06 ± 7.40 | 125.5 ± 14.57 | < 0.001 |
| HDL | 46.66 ± 7.27 | 27.7 ± 5.6 | < 0.001 |
| VLDL | 20.21 ±1.48 | 25.1 ± 2.91 | < 0.001 |
| LDL | 86.50 ±22.15 | 158.44 ±31.38 | < 0.001 |
Comparision of lipid profile in pre and post menopausal women
Comparison of Estradiol in Premenopausal and Postmenopausal Women
| Pre-menopausal n=50 | Post-menopausal n=50 | p-Value |
|---|
| Estradiol (Pg/ml) | 175.48 ± 43.20 | 44.18 ±10.52 | < 0.001 |
| BMI (kg/m2) | 22.9 ± 2.3 | 24.1 ±4.03 | >0.05 |
| W/H ratio | 0.71 ± 0.04 | 0.73 ± 0.06 | > 0.05 |
Correlation between LDL concentration and Estradiol in post menopausal women
Correlation between HDL concentration and Estradiol in post menopausal women
Discussion
After menopause, the reduced oestrogen production from ovaries results in derangement of lipoprotein profile, adverse changes in glucose and insulin metabolism, body fat distribution, coagulation and fibrinolysis and dysfunction of vascular endothelium [14,15]. Oestrogens have several cardio-protective mechanisms that change the vascular tone by increasing nitrous oxide production. Oestrogens stabilize the endothelial cells, they enhance antioxidant effects and alter fibrinolytic protein. All these are cardio protective mechanisms which get lost with the onset of menopause [16,17].
As plasma lipids can be divided into the proatherogenic lipoproteins and antiatherogenic HDL. Assessment of the relative proportions of cholesterol in these two fractions can be valuable than the individual lipid measurements. One method is to compare levels of HDL and non-HDL cholesterol [18]. Another method is the ratio of total cholesterol to HDL-C [19,20], the average ratio of healthy individuals is about 3.5 or lower (i.e., at least 30% of the plasma cholesterol is in the HDL fraction). A lower atherogenic index in premenopausal women indicates a greater proportion of HDL-C, and it thus satisfies the criteria for a reduced risk of coronary heart disease [21]. Postmenopausal women in our study had lower HDL concentrations, which was confirmed by many studies, although studies that contradict these findings also exist. Data from randomized trials have demonstrated that exogenous oestrogen lowers plasma Low-Density Lipoprotein (LDL) cholesterol and that it raises High-Density Lipoprotein (HDL) cholesterol levels by 10-15%. Numerous studies have demonstrated that high levels of HDL-C are associated with a lower incidence of CHD. Conversely, low levels of HDL-C are associated with a higher incidence of CHD. The oestrogen therapy enhances LDL clearance, which probably results from an increased hepatic LDL receptor expression. The LDL oxidation and results in lipid peroxidation. Lipid peroxidation may be a component of the general aging process. Modification is inhibited by antioxidants and oestrogens. Oxidized LDLs increase macrophage uptake, they are cytotoxic, they serve as chemoattractants for circulating monocyte-macrophages, and are immunogenic. The oxidized or modified LDLs are taken up by macrophages, by the scavenger receptors.
The protective mechanism which involves HDL may be due to its role in reverse cholesterol transport, which results in redistribution of cholesterol away from the artery wall and by inhibition of monocyte adhesion and antioxidative activities, that could prevent LDL oxidation.
The plasma LDL-C concentration in this study was calculated by using Friedewald’s formula. This formula relies on an estimate of the VLDL cholesterol that assumes that the cholesterol content of VLDL is about 20% of the fasting plasma triglyceride level. It is reliable only when triglyceride levels are 400 mg/dL or less. None of the women in our study had triglyceride levels above 400 mg/dL. In our study, VLDL showed a significant negative correlation with oestradiol concentration in postmenopausal women, which indicated that oestrogens can modify VLDL concentration, as well as triglycerides. It is well established that VLDL alone is a cardiovascular diseases risk factor.
Menopause leads to changes in lipid profile by reducing HDL, and elevating Total Cholesterol (TC), triglycerides (TG), LDL-cholesterol and VLDL-cholesterol, thus increasing the risk for cardiovascular disease. The results of this study were in agreement with those of earlier studies, which suggested that changes in lipid profile were caused by reduced oestrogen concentrations which were seen in menopause.
[1]. Couderc R, Machi M, Lipoprotein(a): risk factor for atherosclerotic vascular disease important to take into account inpracticeAnn-Biol-Clin 1999 57(2):157-67. [Google Scholar]
[2]. Rich-Edward JW, Manson JE, Hennokeni CH, The Primary prevention of coronary heart disease in womenN. Engl. J Med 1995 332(20):1758-66. [Google Scholar]
[3]. Lerner DJ, Kannel WB, Patterns of coronary heart disease morbidity and mortality in the sexes: a 26 year follow-up of the Framingham populationAm Heart J 1986 383-90. [Google Scholar]
[4]. Laufer Larry R, Gambone-Climacteric Joseph C, Hacker Essentials of Obstetrics and Gynecology4 th editionElsevier Saunders [Google Scholar]
[5]. Shifren Jan L, Schiff Isaac, Section VII - Reproductive Endocrinology 32 – Menopause, Editors: Berek, Jonathan S.TitleBerek and Novak’s Gynecology 2007 14th EditionLippincott Williams and Wilkins [Google Scholar]
[6]. Matthews KA, Meilahn E, Kuller LH, Menopause and risk Factors for coronary heart diseaseN Engl J Med 1989 321:641-46. [Google Scholar]
[7]. Stevenson JC, Crook D, Godsland lF, Influence of age and menopause on serum lipids and lipoproteins in healthy womenAtherosclerosis 1993 98:83-90. [Google Scholar]
[8]. Kuller LH, Meilahn EN, Cauley JA, Gutai JP, Mathews KA, Epidemiologic studies of menopause: Changes in risk factors and diseaseExp Gerontol 1994 29:495-509. [Google Scholar]
[9]. Kannel WB, Studies of Coronary heart disease risk factors: perspective from the Framingham studyAm. Heart J 1987 114:413-19. [Google Scholar]
[10]. Lobo RA, Effects of hormonal replacement on lipids lipoprotein in post-menopausal womenJ Clin Endocrinol 1991 73:925-30.M et al. [Google Scholar]
[11]. Newnham HH, Oestroges and atherosclerotic vascular disease- lipid factorsJ Clin Endocrinol Metab 1993 76:61-93. [Google Scholar]
[12]. Cauley Serum Estrogens and Coronary Artery Disease, in postmenopausal womenArterioscler Thromb Vasc Biol 1994 14:14-18. [Google Scholar]
[13]. Friedewald William T, Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, Without Use of the Preparative UltracentrifugeClinical Chemistry June 1972 18(6):499-502. [Google Scholar]
[14]. Bales AC, In search of lipid balance in older women; New studies raise questions about what works bestPostgrad. Med 2000 108(7):57-72. [Google Scholar]
[15]. Spencer CP, Godsland H, Stevenson JC, Is there a menopausal metabolic syndrome?Gynecol. Endocrinol 1977 11:341-55. [Google Scholar]
[16]. Taddec S, Virdis A, Ghiadoni L, Mattec P, Sudano I, Bernini G, Menopause is associated with endothelial dysfunction in womenHypertension 1996 28:576-82. [Google Scholar]
[17]. Igweh JC, The effects of menopause on the serum lipid profile of normal females of south east NigeriaNigerian Journal of Physiological Sciences 2005 20(1-2):48-53. [Google Scholar]
[18]. The Expert Panel : Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Final reportCirculation 2002 106:3143-421. [Google Scholar]
[19]. Castelli WP, Garrison RJ, Wilson PWF, Incidence of coronary heart disease and lipoproteincholesterol levels. The Framingham StudyJAMA 1986 256:2835-38. [Google Scholar]
[20]. Castelli WP, Abbott RD, McNamara PM, Summary estimates of cholesterol used to predict coronary heart diseaseCirculation 1983 67:730-34. [Google Scholar]
[21]. Grady D, Robin SM, Petitti DB, Fox CS, D. Black- Expert Panel,. Report of the National Cholesterol education programme. Expert panel on detection and evaluation and treatment of high blood cholesterol in adultsArch. Int. Med 1993 148:36-69. [Google Scholar]