Blood supply to kidney is characterised by the presence of variations, both in renal artery and renal vein, which are significantly predominant in most of the studies. So, a detailed knowledge of the anatomy and variational pattern in the blood supply of kidney is more important in an era of renal transplantations and conservative renal surgeries. The renal arteries are paired arteries which arise from the lateral side of the abdominal aorta [1]. The venous drainage occurs through the paired renal veins which drain into the inferior vena cava. Both these vessels enter through the hilum of the kidney. However, accessory renal vessels if present, may enter the kidney either through the hilum or through the surface of kidney. They may enter either through upper pole or lower pole as polar arteries [2]. Hence, this study would serve a useful guideline for performing uroradiological procedures and renal transplant surgeries and for treating renal trauma and hydronephrosis.
Material and Methods
The material for this study comprised of 15 well preserved human adult cadavers (30 kidneys) of both sexes, aged between 60-70 years, which we obtained from the Department of Anatomy, SRM Medical College, Chennai, Tamil Nadu, India. Abdomen opened as per Cunningham’s manure anterior abdominal wall was reflected and the abdominal viscera were removed. Both the kidneys were identified. Renal arteries and renal veins were traced from their origin to distribution. Accessory renal arteries and renal veins if present, were noted and they were documented by photography.
Results
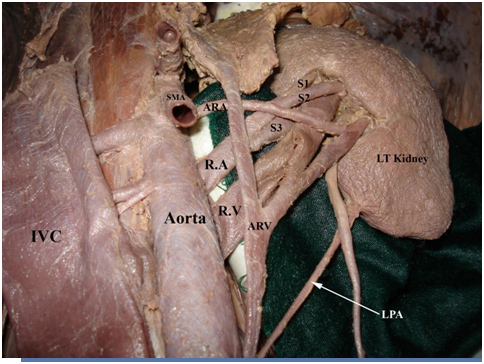
Among the 30 kidneys which were dissected from 15 preserved cadavers, the normal pattern of blood supply to the kidneys was observed in 86.6% cases. The following variations were observed in the remaining 13.4% cases. Pre segmental branches which arose from the renal artery were found in 4 cases (13.3 %) [Table/Fig-1, 2, 3, and 4]. Accessory renal artery could be traced in 4 specimens (13.3%) and all these 4 arteries arose from the abdomen aorta. Regarding the level of origin of accessory renal arteries, out of 4 specimens, in 1 case, it was found to be close to the superior mesenteric artery, in 1 specimen, it took origin below the renal artery, in another case, it was above the renal artery and in the last specimen, it was between the superior mesenteric and renal arteries [Table/Fig-1, 2, 3 and 4].
R.A-Renal artery; S1, S2, S3-pre segmental branches arising from renal artery; ARA-Accessory renal artery SMA-Superior mesenteric artery; R.V-Renal vein; ARV-Accessory renal vein; LPA-Lower polar artery; IVC-Inferiorvena cava
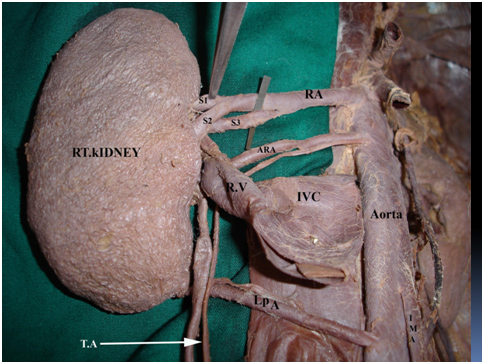
IVC- Inferior venacava reflected down to show the variations; RA-Renal artery; S1, S2, S3-pre segmental branches arising from renal artery; ARA-Accessory renal artery; LPA-Lower polar artery; R.V-Renal vein; IMA-Inferior mesenteric artery; T.A-Testicular artery
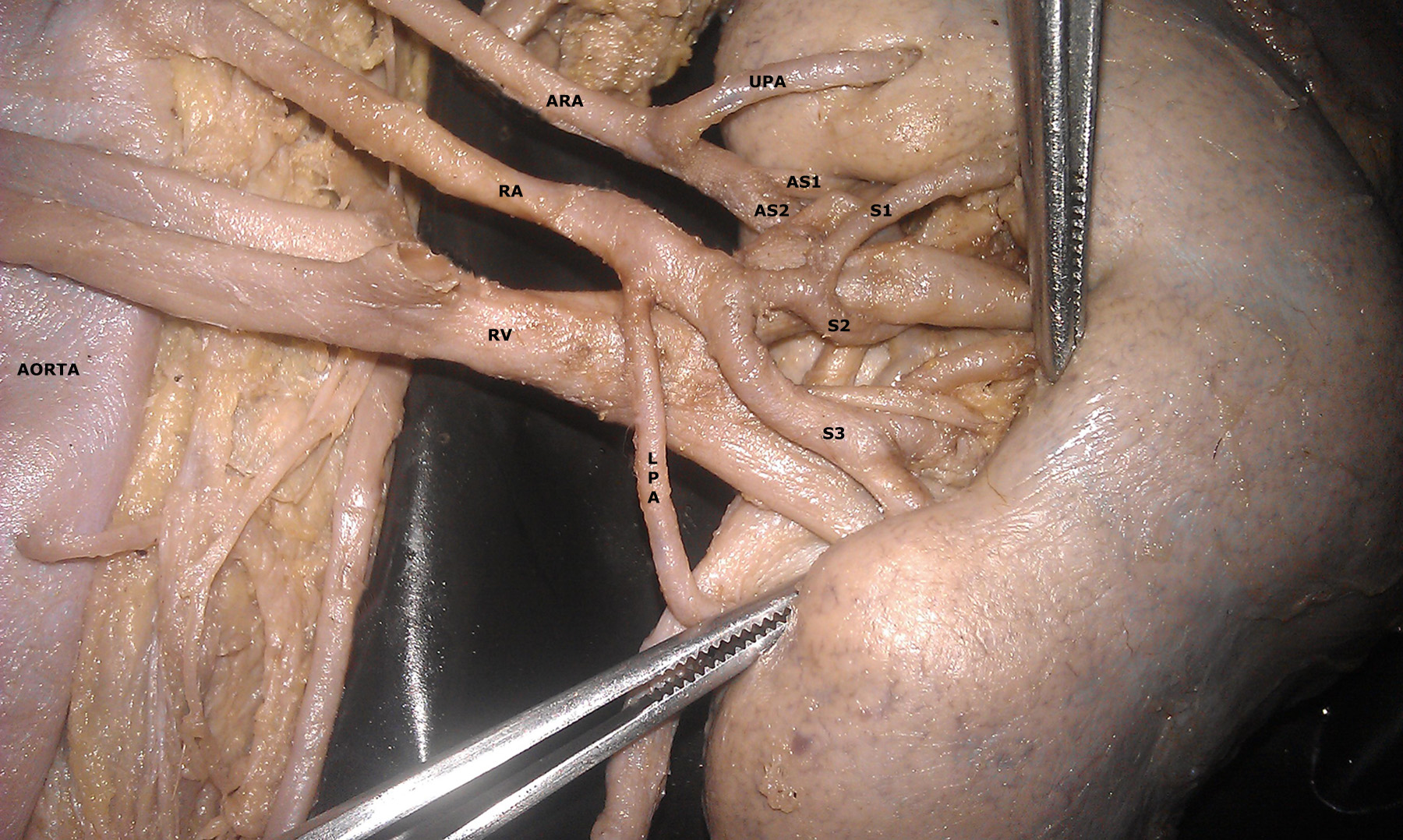
ARA-Accessory renal artery; AS1, AS2-pre segmental branches from accessory renal artery; UPA-upper polar artery RA-Renal artery; S1, S2, S3-pre segmental branches from renal artery LPA-lower polar artery from renal artery; RV-Renal vein
ARA-Accessory renal artery; AS1, AS2, AS3-presegmental branches from accessory renal artery RA-Renal artery-S1, S2, S3-presegmental branches from renal artery
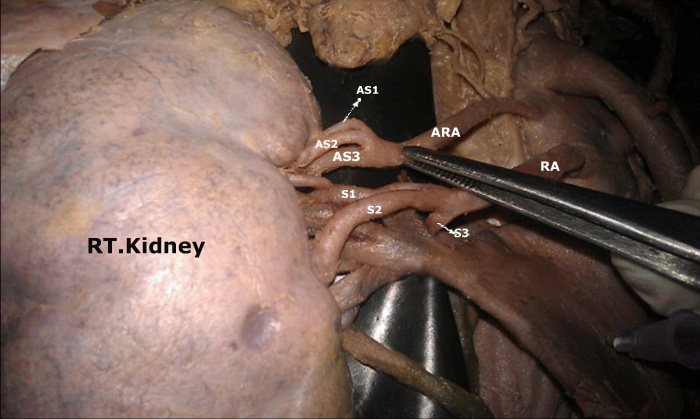
Pre–segmental branches which arose from accessory renal arteries were observed in 2 cases (6.6%). Out of 2 cases, in one specimen, the accessory renal divided into 2 pre hilar branches AS1 and AS2 and in other specimen, we could trace 3 pre segmental branches, namely, AS1, AS2 and AS3, as shown in [Table/Fig-3 and 4].
Presence of an upper polar artery which arose from the accessory renal artery was found in 1 specimen out of the 30 cases which were studied, which accounted for 3.3% cases [Table/Fig-3].
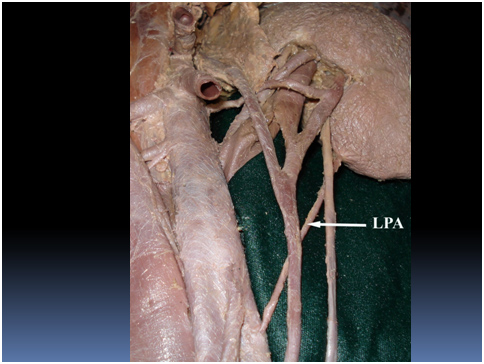
In 3 cadavers, lower polar arteries could be dissected out (10%). In 2 specimens, they arose from the abdominal aorta and in 1 case, they arose from the renal artery itself [Table/Fig-5, 2 and 3].
LPA-Lower polar artery arising from abdominal aorta
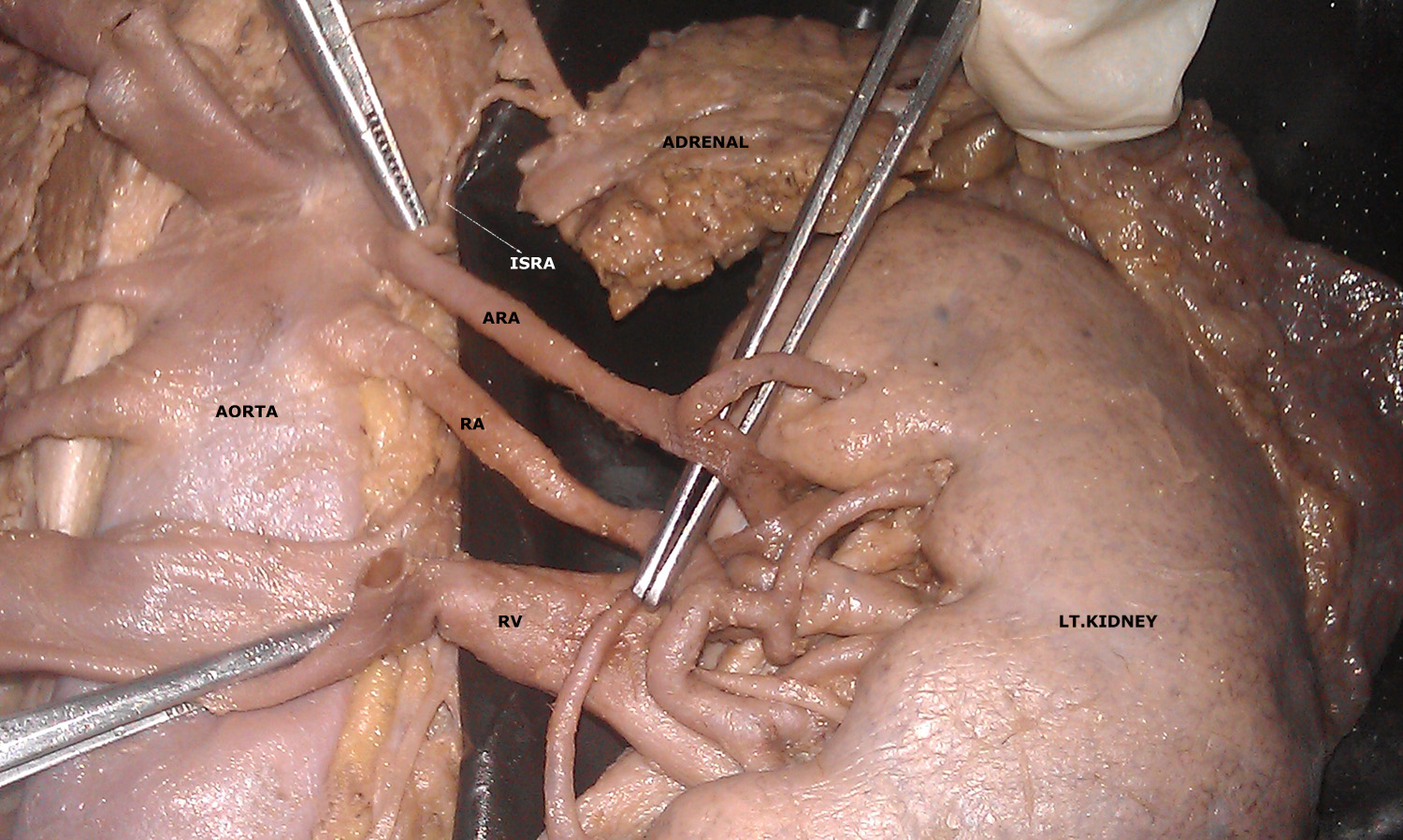
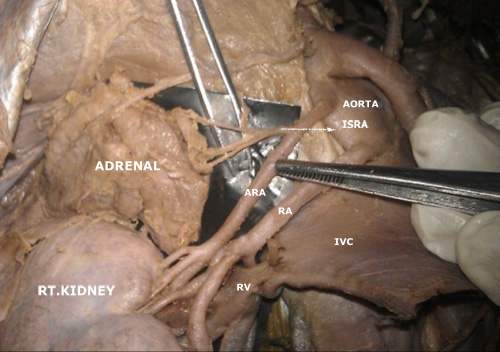
Accessory renal artery giving origin to inferior supra renal artery was noted in 2 cases (6.6%) In one of the specimens, this artery in turn, divided into 3 branches to supply the lower part of the gland [Table/Fig-6 and 7].
ARA-Accessory renal artery;RA-Renal artery; RV-Renal vein; ISRA-inferior suprarenal artery arising from accessory renal artery
ARV-Accessory renal vein; LTV-Left testicular vein; LU-Left ureter

Renal vein divided into upper hilar and lower hilar segments. This was noted in 2 specimens [Table/Fig-3 and 4].
Left accessory renal vein was traced in one specimen and the same vein showed upper hilar and lower hilar divisions with inferior supra renal vein and testicular vein as its tributaries and it drained into the inferior vena cava [Table/Fig-1 and 8].
IVC-Inferior venacava reflected down to show the variations; ARA-Accessory renal artery; ISRA-inferior supra renal artery from accessory renal artery; RA-Renal artery;RV-Renal vein
Discussion
Variations in renal arteries accounts for about 30% of its existence [1]. These variations are classified as accessory or aberrant renal arteries. Accessory renal arteries are additional arteries which pass along with normal renal arteries through the hilum. Aberrant arteries are those which enter the kidney by piercing the substance of the kidney, either through upper pole or lower pole as polar arteries. All these variations can be explained on embryological basis.
Renal, suprarenal and gonadal organs are supplied by dorsal aorta, by lateral mesonephric arteries. According to Felix, these lateral mesonephric arteries are divided into upper, middle and lower groups. The middle group, namely 6-9th segment, gives rise to renal arteries. Persistence of more than one renal artery in the middle group results in accessory renal arteries [3].
The various types of pre–hilar branching patterns which were observed were fork, duplicate, triplicate and ladder patterns. These multiple branches represent the segmental distribution of the kidney [4] and so, the risk of a haemorrhage during transplantation, segmental ischaemia and post operative haemorrhage are more. Saldarriage et al., observed a bilateral additional artery in 7.7% of the cases. He also reported that additional arteries had entered through the hilum in 12% of cases and in 1.8% of cases, it was inferior polar arteries [2]. In our case also, we observed bilateral additional renal arteries and they had entered through the hilum. Apart from this, we also encountered both inferior and superior polar arteries.
Bordei P et al., in their renal vasculature, studied 54 cases, out of which 24 cases had entered through the hilum,16 were inferior polar arteries and in 5 cases, it were superior polar arteries [5]. These double renal arteries arose from the abdominal aorta. In our study also, both the additional and aberrant arteries arose from the abdominal aorta. These aberrant arteries could arise as high as inferior phrenic or as low as internal iliac arteries.
The accessory or aberrant renal arteries may be important for the clinicians, since they have a vital role to play in causation of hydronephrosis, renal transplantations and in micro vascular surgeries. Variations in renal veins are usually discovered during venography or any operative procedures. Renal arterial variations are more frequently observed than renal veins, which account for about 18% of the cases [6]. Anupama et al., reported various congenital variations of renal veins, in which the study described about supernumerary renal vein, in which presence of an additional vein arising from the hilum of kidney and draining into inferior vena cava. Out of 30 cadavers which were studied, they described a right side supernumerary renal vein in 10 cases and in only one case, they described a bilateral renal vein variation [7].
Variations in renal veins are caused by anomalies which are related to the development of inferior vena cava [8]. The literature has described renal vein variations which were more common on the right side (28%) than on the left side (1%) [9]. In our study, we reported supernumerary renal vein on the left side.
Inferior supra renal artery arises mainly from renal artery. In a small percentage of cases, it arises from aorta, as a common trunk with superior polar renal artery, or from a supplementary renal artery and very rarely, from gonadal artery.
Inferior supra renal artery arises in common with superior testicular artery and variations in middle suprarenal arteries are the ones which are most frequently encountered in the literature [10]. Whereas, in our study, inferior suprarenal arteries on both side arose from the accessory renal arteries, which are considered as a rare entity.