Introduction
On seeing the extreme variations in the gross anatomy of the thyroid gland, Marshall stated that it was difficult to speak about a normal thyroid gland [1]. The thyroid gland in man is located in the lower half of the front of the neck. It consists of two lateral lobes which are connected by an isthmus. In some cases, an additional lobe is present, which is known as the Pyramidal Lobe (PL). It forms a long pyramid which is attached by its base to the superior border of the isthmus, usually at its junction with the left lobe. Its apex is attached to the body of the hyoid bone by a fibrous band, which sometimes contains muscular fibres which are known as the Levator Glandulae Thyroideae (LGT). It is seldom midline in position [2–5].
The organogenesis of the thyroid gland in humans is often disturbed, leading to a variety of morphological variations of the gland, such as hypoplasia, ectopy, hemiagenesis and agenesis [6]. It is well known for its developmental anomalies which range from common to rare. The common anomalies include persistence of pyramidal lobe and thyroglossal duct cysts. Rare anomalies are agenesis or hemi-agenesis of thyroid gland, agenesis of isthmus alone or aberrant thyroid glands and origin of levator glandulae thyroidae from isthmus, of which very few cases have been reported in literature [1,7].
According to Standring, musculus levator glandulae thyroideae is a fibrous or fibromuscular band that stretches from the pyramidal lobe or upper border of isthmus of thyroid gland, usually on the left side, to the body of the hyoid bone above [8]. Based on the observations of 210 levators, Mori [9] classified levator glandulae thyroideae into five types; a) Hyopyramidalis, b) Thyreopyramidalis, c) Thyreoglandularis, d) Hyoglandularis, and e) Tracheoglandularis.
In the present case, Levator Glandulae Thyroideae was seen (pyramidal lobe absent ) on the left side. It directly came from upper border of isthmus and went upto hyoid bone (the Hyoglandularis type according to Mori’s classification). Moreover, the knowledge about the fleshy slip of the levator glandulae thyroideae is also very important during neck surgeries, for preventing iatrogenic injuries [10].
Case Report
During a routine dissection of neck on a male cadaver who was aged about 55 years, in the Department of Anatomy, Guru Gobind Singh Medical College, Faridkot Punjab, India, the presence of levator glandulae thyroideae was observed on the left side. It was dissected carefully, to look for its attachments above and below and for its innervation. A thin band of muscular like tissue stretched from the upper border of isthmus of thyroid gland, to the body of hyoid, on the left side [Table/Fig-1]. According to Mori’s classification, the levator glandulae thyroideae in this case was of the Hyoglandularis type. It measured 3 cm. in length and 0.6 cm in breadth. A careful dissection which was done, revealed that there was no pyramidal lobe. This band had an innervation from branches of external laryngeal nerve. The thyroid gland and other structures in the vicinity appeared to be normal. However, the superior thyroid artery was absent on the left side. Instead, the lobe was being supplied by the inferior thyroid artery, which came out as the branch of the thyrocervical trunk. On right side, superior thyroid artery was normal.
Incidence of occurance of pyramidal lobe & levator glandul aethyroideae, originating from pyramidal lobe
| Sl. No. | Author | % incidence of pyramidal lobe | % incidence of LGT associated with pyramidal lobe |
|---|
| 1 | Enayetullah [11] | 50% | 32% |
| 2 | Begum [12] | 26.7% | 15% |
| 3 | Ranade et al., [6] | 58% | 49.5% |
| 4 | Sultana et al., [13 & 14] | 50%* | 37%# |
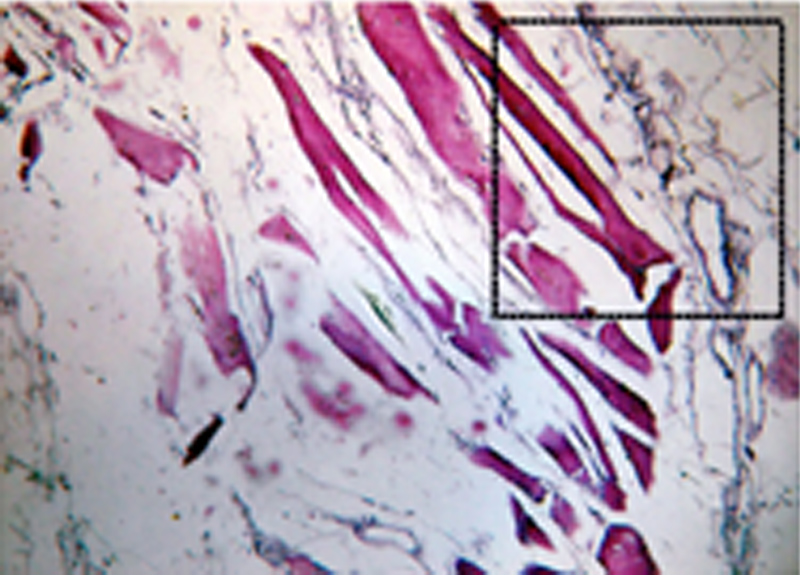
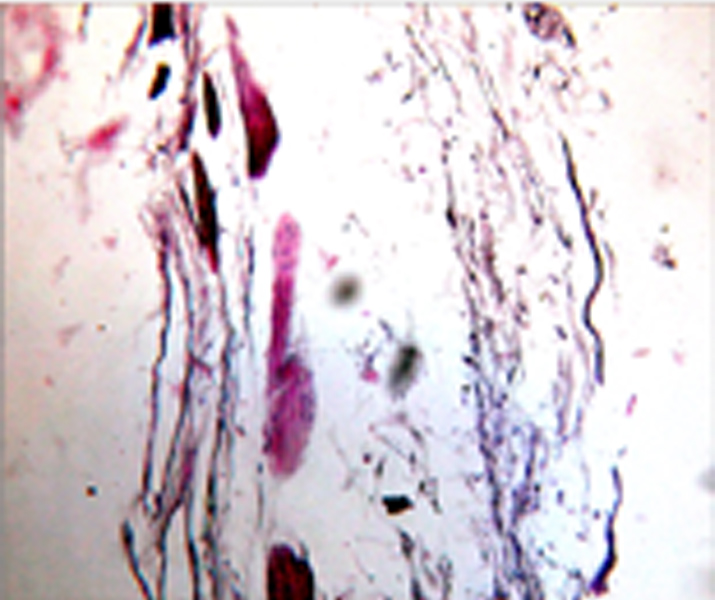
This tissue of the levator glandulae thyroideae was subjected to a microscopic examination. The tissue was dissected out from the cadaver and it was sectioned at three levels – upper, middle and lower regions. The tissues were then processed and they were stained by haematoxylin and eosin stain. The examination revealed the presence of thyroid follicles which were lined by cuboidal epithelium, with a moderate amount of colloid in their lumina and surrounding fibrous tissue, with skeletal muscle fibres at the lower levels [Table/Fig-2a, 2b, 3a, 3b, 4a and 4b] and skeletal muscle fibres with fibrocollagenous stroma in the section which was taken from the upper level (towards the hyoid bone).
A general view of fibromusculoglandular tissue of Levator glandulae thyroideae
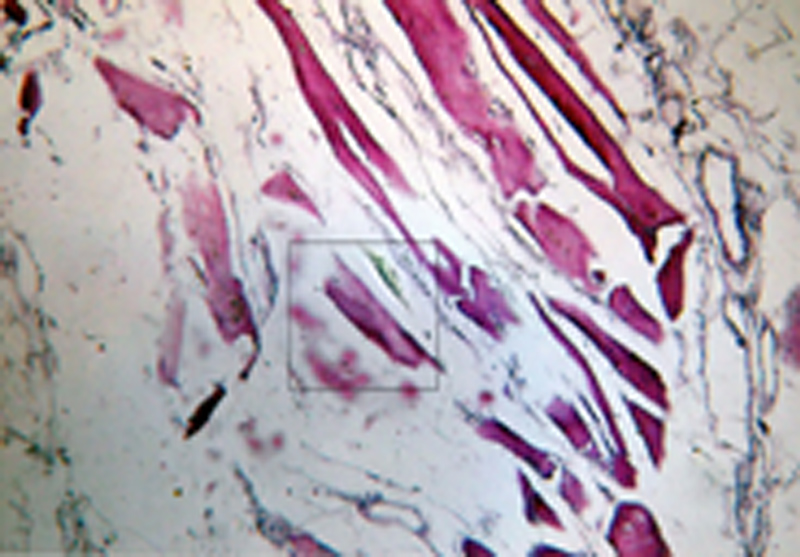
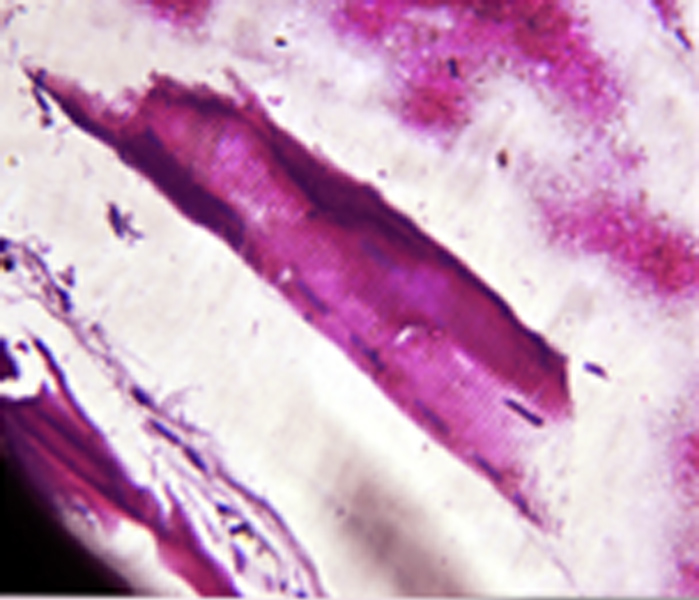
Magnified view of area marked showing skeletal muscle fibre
A general view of fibromusculoglandular tissue of Levator glandulae thyroideae
Magnified view of area marked showing fibrous tissue
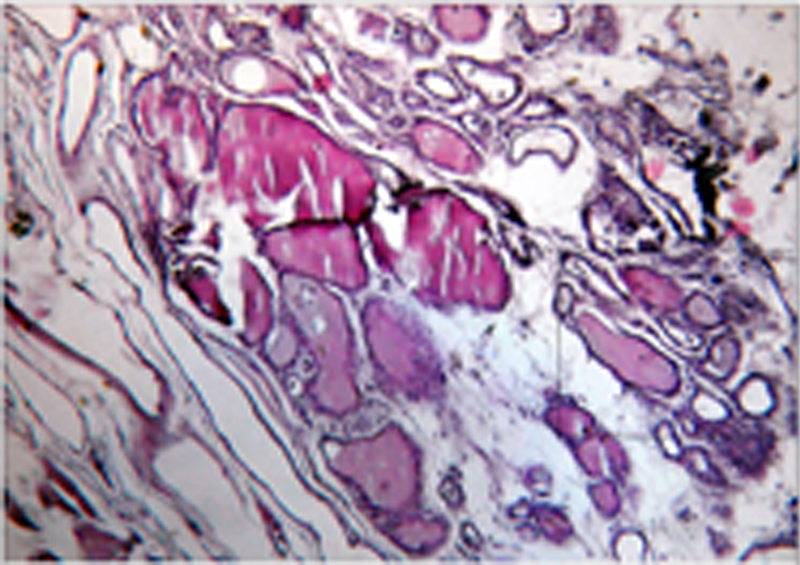
A general view of fibromusculoglandular tissue of Levator glandulae thyroideae
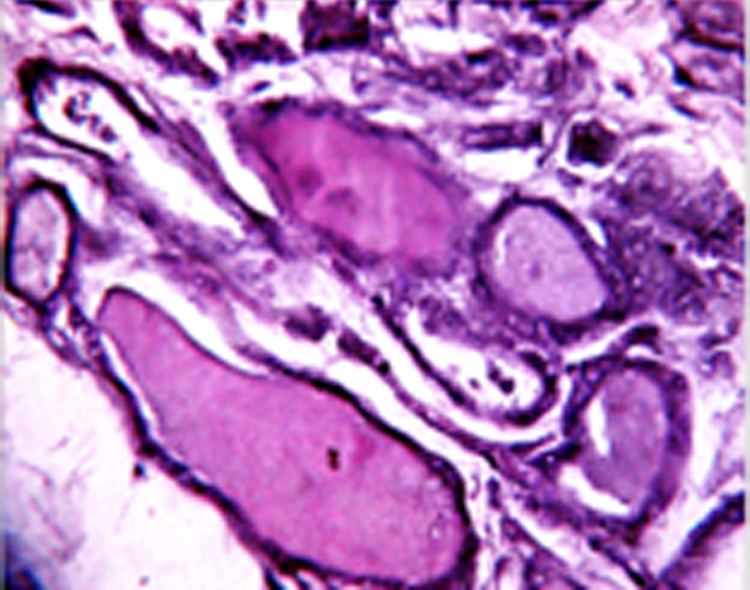
Magnified view of area marked showing thyroid follicle
Discussion
Anatomical variations in the musculature surrounding the thyroid gland have the potential to cause iatrogenic injuries during neck and thyroid surgical procedures. Presence of pyramidal lobe and levator glandulae thyroideae which originating from pyramidal lobe are common, but origin of levator glandulae thyroidae from isthmus is rare.
Sultana et al.,* [13] observed that a half of the cases (30 out of 60) had pyramidal lobe. In another study, Sultana et al.,# [14] found that the levator glandulae thyroideae was evident in 43.33% cases (26 cases out of 60). Among those, 22 (84.65%) were associated with the pyramidal lobe, all extending from the apex of the pyramidal lobe to the hyoid bone. In 4 cases, they found it to take origin from the isthmus, of which 2 were attached to the hyoid bone, as in the present case and the other 2 with the corresponding oblique line of the thyroid cartilage above. So, it is obvious from above discussion, that extent of levator glandulae thyroideae from isthmus to hyoid bone is a rare occurance.
The levator glandulae thyroideae which was observed in the present study was of Hyoglandularis type (Mori’s classification), which was found to be attached to body of hyoid bone above and it stretched from the upper border of isthmus of thyroid gland on the left side, with innervation from branches of external laryngeal nerve. The pyramidal lobe was, however, absent. Sinnatamby [15] stated that it may receive its innervation from external laryngeal nerve, an observation which was confirmed in the present case also.
Gunapriya et al., [16] also reported a case of presence of levator glandulae thyroideae with absence of pyramidal lobe on the right side, which stretched from the upper border of isthmus of thyroid gland, to the lower border of the lamina of thyroid cartilage, which measured 1 cm in length and 0.6 cm in breadth. Hence, according to Mori’s classification, the levator glandulae thyroideae in this case was of Thyreoglandularis type. This band was made up of fibroglandular tissue, it did not have innervation from any nerve and it did not extend up to hyoid bone.
Eisler and Der [17] did an extensive study on the levator glandulae thyroideae and its innervation. They stated that the levator of the thyroid gland may be innervated, either by ansacervicalis or through vagus. They also regarded the levators of the thyroid gland, to be divisible into three groups viz., the anterior, lateral and posterior levators which were derived from cricothryoid, infrahyoid and inferior constrictor muscles of pharynx. The morphological difference in the evolutionary origin does not result in any changes in thyroid function.
According to Ranganathan [18], leavator glandulae thyroidae is said to represent the detached part of infrahyoid muscles and it may be innervated by a twig from ansacervicalis. Loukas et al., [19] also stated the nerve supply of the levator glandulae thyroideae by a twig of the ansacervicalis.
According to Hamilton and Mossman [20], it may be considered as a fibrous or a muscular replacement of the pyramidal lobe. In a study which was done by Bergman et al., [21] of the 104 specimens in which the pyramidal process was found to be present, 55 were glandular up to the hyoid bone; in 12, the process was connected to the hyoid by fibrous tissue, and in two, it was connected by muscle. The muscular fasciculi which are occasionally found to descend from the hyoid bone to the thyroid gland or its pyramidal process, are known as the levator glandulae thyroideae. The muscle fibres are most frequently derived from the thyrohyoid muscle, but occasionally, they are independent of it. The isthmus of the gland may be joined to the hyoid bone which is above the organ, by a fibrous cord, which is a remnant of the embryologic thyroglossal duct.
According to Gregory and Guse [22], levator glandulae thyroideae is an accessory muscle which runs from the hyoid bone to insert partly on the thyroid cartilage and partly on the isthmus of the thyroid gland. Merkel [23] thought that the levator glandulae was constant and glandular, though it was usually surrounded by muscle fibres. Huschke [24] spoke of the structure only as glandular and he mentioned nothing about the muscle. Bourgery [25] described and illustrated a muscle, which he called as “hyo-thyroïdien”, which occupied the place of the pyramidal lobe. Finally, Godart [26] reported a case in which the structure was indeed muscular, as it was found on the basis of the nitric acid test for muscles. Its usual full name in the literature is levator glandulae thyroideae of Soemmerring. Allan [27] reported levator glandulae thyroideae, a band of connective tissue, which extended from the apex of right or left lobe or isthmus of the thyroid gland to the hyoid bone. So, it is obvious from above discussion, that its fibromusculogandular nature was not simultaneously reported by any of the authors as in the present case, where the microscopic examination revealed that leavator glandulae thyroideae was mainly made up of glandular, muscular and fibrous tissue. Hence, in this case, the levator glandulae thyroideae which had innervation from branches of external laryngeal nerve, was fibromusculoglandular in nature.It may represent the detached part of infrahyoid muscles or remnants of the connective tissue of the thyroglossal duct.
Morrigyl and Sturm [28] reported a rare case in which both the inferior thyroid arteries and the left superior thyroid artery were absent. Probably, so far, none have encountered a case of origin of levator glandulae thyroideae from isthmus, which was associated with absence of superior thyroid artery on the same side, as was found in the present case. Knowledge on vascular aberrations is essential in routine surgical procedures. Hence, a thorough knowledge on the thyroid anatomy and its associated anatomical variations is very much essential, so that these anomalies may not be overlooked in the differential diagnosis.
Clinical Significance
The knowledge on the extent and innervations of the levator glandulae thyroideae is very important during neck surgeries, to avoid iatrogenic injuries. As has been discussed earlier, leavator glandulae thyroideae may represent the persisting distal end of thyroglossal duct. Accessory nodules/ectopic thyroid tissues of the thyroid are usually found at the embryonic origin of thyroid, at the foramen caecum and along the thyroglossal tract. Therefore, the anterior cervical region has to be investigated very carefully during surgeries, so as not to leave behind any residual thyroid tissue, during total thyroidectomies. Knowledge on vascular aberrations and proper identification of vessels, (as in this case, superior thyroid artery was absent), are very important, in order to avoid major complications, especially during head and neck surgeries.
Conclusion
The purpose of this report was to highlight different anatomical variations with respect to the thyroid gland and thereby, to form a cornerstone for safe and effective surgeries.
[1]. Marshall CF, Variation in the form of the thyroid in manJ Anat Physiol 1895 29:234-39. [Google Scholar]
[2]. Wood JF, Buchanan’s Manual of Anatomy 1953 8th EdLondonBilliere Tendall and Cox [Google Scholar]
[3]. Du Plessis DJ, In synopsis of surgical anatomy 1975 11th EdBristolJohn Wright and Sons [Google Scholar]
[4]. Hollinshead WH, Rosse C, Textbook of anatomy 1985 4th EdPhiladelphia, NewYork, LondonHarper and Row Publishers [Google Scholar]
[5]. Standring S, In: Gray’s Anatomy 2005 39th EditionLondon, New YorkElsevier Churchill Livingstone [Google Scholar]
[6]. Ranade AV, Rai R, Pai MM, Nayak SR, Prakash Krishnamurthy A, Anatomical variations of the thyroid gland: possible surgical implicationsSingapore Med J 2008 49:831-34. [Google Scholar]
[7]. Testut L, Latarjet A, Anatomia Humana. Tomo 1978 IV. EdBarcelonaSalvat:402-04.Spanish [Google Scholar]
[8]. Standring S, In: Gray’s Anatomy 2006 39th EditionLondonElsevier Churchill Livingstone:561 [Google Scholar]
[9]. Mori M, Statistics on the musculature of the JapaneseOkajimas Folia Japan 1964 40:195-300. [Google Scholar]
[10]. Geraci G, Pisello F, Li Volsi F, Modica G, Sciumè C, The importance of pyramidal lobe in thyroid surgeryG. Chir 2008 Nov-Dec 29(11-12):479-82. [Google Scholar]
[11]. Enayetullah M, Gross and histomorphological study of the thyroid and parathyroid glands in Bangladeshi people (M.Phil.Thesis). Dhaka: University of Dhaka; 1996 [Google Scholar]
[12]. Begum M, Gross and histomorphological study of human postmortem thyroid gland in Bangladeshi people (M.Phil.Thesis). Dhaka: University of Dhaka; 2004 [Google Scholar]
[13]. Sultana SZ, Mannan S, Ahmed MS, Rahman MM, Khan MK, Khalil M, An anatomical study on pyramidal lobe of thyroid gland in Bangladeshi peopleMymensingh Med J 2008 Jan 17(1):8-13. [Google Scholar]
[14]. Sultana SZ, Khalil M, Khan MK, Shamim R, Parveen S, Ara ZG, Morphological study of levator glandulae thyroideae in Bangladeshi cadaverMymensingh Med J 2009 July 18(2):179-83. [Google Scholar]
[15]. Sinnatamby CS, In: Last’s anatomy, regional and applied 2007 11th EditionLondonElsevier -Churchill Livingstone:352 [Google Scholar]
[16]. Gunapriya R, Varsha S, Senthil Kumar B, Levator Glandulae Thyroideae with the absence of Pyramidal Lobe – A case reportInternational Journal of Anatomical Sciences 2010 1:45-47. [Google Scholar]
[17]. Eisler P, Der M, Levator glandulae thyreoidea und verw and tepraelaryngeale MuskelbildungenAant Anz 1922 17:183-96. [Google Scholar]
[18]. Ranganathan TS, In: A Textbook of Human Anatomy 2002 4976th EditionNew DelhiS. Chand and Company Ltd:496-97. [Google Scholar]
[19]. Loukas M, Merbs W, Tubbs RS, Curry B, Jordan R, Levator glandulae thyroideae muscle with three slipsAnatomical Science International 2007 83(4):273-276.DOI:10.1111/j.1447-073X.2007.00198.x [Google Scholar]
[20]. Hamilton WJ, Mossman HW, Hamilton Boyd, Mossman’s human embryology: prenatal development of form and function 1978 4th edLondonWilliams and Wilkins:223-26. [Google Scholar]
[21]. Bergman RA, Afifi AK, Miyauchi R, Thyroid gland In: Illustrated Encyclopedia of Human Anatomic Variation: Opus IV Organ Systems: Endocrine System. (www.anatomyatlases.org/Anatomic.variants/organ.system/text/thyroidgland.html/) 2007 [Google Scholar]
[22]. Gregory JK, Guse DM, Unique variant of levator glandulae thyroideae muscleClinAnat 2007 20:966-67. [Google Scholar]
[23]. Merkel FS, Die Anatomie des Menschemmit Hinweisen auf die arztliche Praxis, Abt. 3 1913 50WiesbadenJF BergmanGerman [Google Scholar]
[24]. Huschke E, Traité de splanchnologieet des organes des sensIn: Encyclopedie Anatomique 1845 Vol VParisJB Bailliere:274 [Google Scholar]
[25]. Bourgery JM, Traitecompletd’anatomie de l’homme, comprenant la medecineoperatoire, avec planches lithographieesd’apres nature par NH Jacob. Atlas. Paris. C. [-A.] Delaunay 1831; Tome II: 90, 1836; Tome IV: 91. French [Google Scholar]
[26]. Godart J, Muscle de la glandethyroide, muscle de Duvernoi, musculus levator glandulae thyreoideae. (Exemple du Soemmerring.) [Abstr.]Bull Soc Anat Paris 1847 22:202-05.French [Google Scholar]
[27]. Allan FD, An accessory or superficial inferior thyroid artery in a full term infant AnatomyRec. 1952 112:53 [Google Scholar]
[28]. Morigyl B, Sturm W, Absence of three regular thyroid arteries which are replaced by an unusual lowest thyroid artery (A thyroideaima)Surg Radiol Anat 1996 18:147-45. [Google Scholar]