A Rare Case of Tubercular Pyo–Pneumothorax Herniating through the Inter-Costal Drainage Site
Peter George1, Maroli Roshan2, Swapna Ponmaleri Koroth3
1 Associate Professor,Department of Medicine, Father Muller Medical College, Mangalore – 575002, India.
2 Professor,Department of Medicine, Father Muller Medical College, Mangalore – 575002, India.
3 Assistant Professor,Department of Medicine, Father Muller Medical College, Mangalore – 575002, India.
Name, Address, E-Mail Id of The Corresponding Author: Dr Peter George, Associate Professor, Department of Medicine, Father Muller Medical College, Father Muller Road, Mangalore, Karnataka, India.
Phone: +91-9845177660, +91-824 2238000 Fax: +91-824 2436352
E-mail: drpetergeorge2002@yahoo.com
Pyo-pneumothorax, Tuberculosis, Intercostal drainage site, Herniation
A 53 year old diabetic male, who was on anti – tubercular treatment, presented with an expansile swelling on his chest, at the intercostal drainage (ICD) site. He was diagnosed to have a left sided tubercular hydro – pneumothorax, about six weeks earlier. He had noticed the swelling at the ICD site, 5 days ago and he had no pain. Clinically, an expansile swelling of size 5 x 4 cm, was seen at the 6th ICS, in the mid axillary line, which was partially reducible, with palpable crepitations [Table/Fig-1]. The left hemi – thorax showed reduced movements and breath sounds. Contrast enhanced computer tomographic (CECT) images of thorax showed left upper lobe consolidation, with cavities and a hydro – pneumothorax. The left pleural space was seen to extend through the dehiscence on lateral chest wall, forming an air – filled subcutaneous swelling. [Table/Fig-2]. Anti-tubercular therapy was continued and a fresh ICD was inserted at the lower intercostal space, which drained the purulent fluid. After a week, repair and layered suturing was done at the site of dehiscence. The wounds approximated and healed over the next 3 – 4 weeks. A pyo-pneumothorax which is caused by tuberculosis is common in endemic areas [1]. There is one report in the literature on herniation of an emphysematous bulla through an ICD site [2]. However, herniation of a pyo-pneumothorax through a closed ICD site was not found in our literature review.
Serial photographs demonstrating an expansile swelling with expiratory and inspiratory movements in left infra axillary area(marked with black arrows)

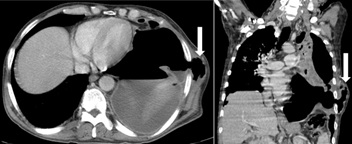
Transverse and coronal images by CECT of thorax showing pleural space extending through the left lateral chest wall dehiscence forming an air-filled subcutaneous swelling(marked with white arrows)
[1]. Kim HY, Song KS, Goo JM, Lee JS, Lee KS, Lim TH, Thoracic sequelae and complications of tuberculosisRadiographics 2001 21:839-58. [Google Scholar]
[2]. Okur E, Tezel C, Baysungur V, Halezeroglu S, Extrathoracic herniation of a lung bulla through a tube thoracostomy siteInteract Cardiovasc Thorac Surg 2008 7:1210-11. [Google Scholar]