The Rosai Dorfman Syndrome-The Report of A Rare Case
Snehalatha R1, Senthilnathan P2, Prathiba Ramani3, Sherlin J Herald4
1 Senior Lecturer, Department of Oral & Maxillofacial Pathology, SVS Institute of Dental Sciences, Mahboob Nagar, A.P., India.
2 Reader, Department of Oral & Maxillofacial Surgery, Saveetha University of Dental Sciences, Chennai, India.
3 Professor and Head, Department of Oral & Maxillofacial, Saveetha University of Dental Sciences, Chennai, India.
4 Reader, Department of Oral & Maxillofacial Pathology, Saveetha University of Dental Sciences, Chennai, India.
Name, Address, E-Mail Id of The Corresponding Author: Dr Snehalatha R, 12-2-823/5, F-201, Surya Residency, Santhosh Nagar, Mehdipatnam, Hyderabad, A.P., India.
Phone: 09885411661
E-mail: drrsneha@gmail.com
Rosai Dorfman syndrome known as Sinus Histiocytosis with Massive Lymphadenopathy (SHML) is an uncommon benign systemic histio-proliferative disease which affects lymph nodes , most often those of the neck (cervical lymphadenopathy). The characteristic histological feature is lymphophagocytosis which is specific for this syndrome. Evidence based survey reveals that many cases that have been reported in india are from medical fraternity other than dental colleagues. As dental professionals we document a rare case of Rosai – Dorfman syndrome , reported to the department of oral and maxillofacial pathology with the cheif complaint of swelling in the neck region.
The Rosai-Dorfman disease, Histiocytosis, Cervical lymph nodes, Emperipolesis
Case Report
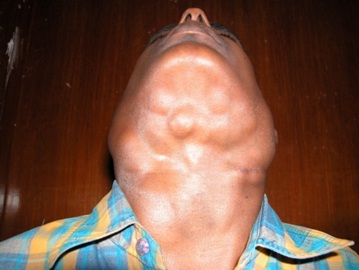
A 21 years old male reported to our hospital with the chief complaint of painful swellings in the neck. He also had swellings in the parotid and cervical region which were present for over a period of 6 months [Table/Fig-1]. History revealed that he had developed multiple swellings in the axillary, sacral and ingunal region 3 years ago. The swellings were initially small and had gradually progressed to the present size. The swellings were well defined and the overlying skin was normal with approximate size of 1-6 cm in diameter. On palpation they were soft in consistency, tender, well defined and non matted. His medical history was not contributory but he was suffering from low grade fever since the age of 12 years.
Patient with massive cervical lymphadenopathy
He was moderately built and anaemic. All the other family members were clinically normal. Intra oral findings showed that the periodontium and the dentition was normal. His Laboratory tests revealed normochromic and normocytic anaemia. There was no increase in ESR, leukocytosis, or hypergammaglobulinaemia. MRI findings of this case showed multiple nodular lesions on both sides of neck, extending from submandibular level, involving both posterior triangle and I J V chain groups, up to superior mediastinal right para tracheal region, appearing hypointense on T1 and bright on T2 images. The nasopharynx oropharynx and laryngopharynx region appear normal with no definite mass lesion identified. The parapharyngeal fat planes appear preserved. The soft tissues of the neck including the muscles and the intramuscular fat planes appear normal. The carotid vessels appear normal, except for the displacement. No evidence of bony destruction seen, Atlanto axial articulation appears normal. No features to suggest basilar invagination. Paranasal sinuses shows marked inflammatory changes.
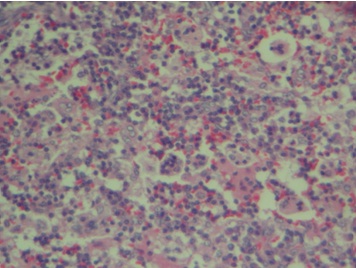
The incisional biopsy of cervical lymph nodes was done. The histopathological findings showed massively distended sinuses, Presence of numerous large histiocytes with vesicular nuclei , distinct nucleoli and abundant pale cytoplasm [Table/Fig-2]. Characteristic lymphophagocytosis was present with intracytoplasmic RBC, neutrophils and plasma cells (emperipolesis) [Table/Fig-3]. This (emperipolesis) is considered to be the hallmark of the disease. Based on the clinical findings of bilateral cervical lymphadenopathy ,MRI findings and Histopathological examination of cervical lymph nodes , the diagnosis was given as sinus histiocytosis with massive lymphadenopathy (Rosai Dorfman Syndrome).
Low power view lymph node showing distended sinuses

High power view showing Emperipolesis
Discussion
Rosai- Dorfman syndromes are rare, diseases of histiocytes. Initially it was described by Azoury and Reed and later by Rosai and Dorfman in 1969 which is now widely known as Rosai- Dorfman disease or syndrome [1], It primarily involves lymph nodes but in 43% of cases, extranodal involvement is also seen. The common sites for extranodal involvement are skin, mucosae, spinal cord, pancreas [2,3] and that of the head and neck are nasal cavity and major salivary glands [4] Though it is considered as a benign disorder , can some times behave in an aggressive manner leading to significant morbidity and mortality [5]. It can affect any age group but most commonly seen in second decade of life. The etiology of the disease is still controversial but it is presumed to be due to an immune regulation disorder, as well as infections caused by agents like Herpes viruses, Epstein – barr virus, Cytomegalovirus, Brucella and Klebsiella [6,7].
Two theories have been put forward to describe the pathogenesis of the disease. The first theory states that it is caused by a specific infectious process, based on the onset of the disease. (localized adenopathy, low grade fever). This theory holds true for our case where the patient was suffering from low grade fever since the age of 12 years.
Second theory states that the disease is due to an abnormal immunologic response. This theory is supported by the study done by Middel P et al., [8] where they concluded that stimulation of monocytes/macrophages via macrophage colony stimulating factor (M-CSF) leading to immune suppressive macrophages represents a main mechanism for the pathogenesis of SHML. The characteristic clinical feature of the disease is presence of massive, painless, bilateral cervical lymphadenopathy with other nodal sites including axillary, inguinal, para aortic and mediastinal lymph nodes. The same clinical picture was present in our case too. The histopathology of this disease is very characteristic. Lymph nodes shows massively distended sinuses, presence of numerous large histiocytes with vesicular nuclei, distinct nucleoli and abundant pale cytoplasm and Emperipolesis. Emperipolesis, a biological phenomenon, was defined by Humble et al., in 1956 as, “the active penetration of one cell by another which remains intact”. It differs from phagocytosis because the engulfed cell exists within another cell, remains viable, and can exit with no physiological and morphological consequence for either of them [9]. Laboratory alterations are frequent and include anemia in 66% of the cases, leukocytosis in 59%, neutrophilia in 68%, increased ESR in 88 % and hypergammaglobulinemia in 90% of the cases. However in our case the laboratory finding were not contributory. A differential diagnosis of lymphomas was considered because some of the diffuse large B-cell lymphomas showed extensive emperipolesis [10]. Which is considered to be a characteristic histological picture of Rosai Dorfman Syndrome, but the difference is immunohistochemically numerous CD68-positive and S-100-negative histiocytes are present in diffuse large B-cell lymphomas [10]. Although some histologic features are similar between Langerhans cell histiocytosis and Rosai Dorfman Syndrome there are several distinguishing features. In LCH, the histiocytes do not exhibit lymphophagocytosis and moreover electron microscopy often reveals the pathognomnic Birbeck granules [11]. The histiocytes of Rosai-Dorfman Syndrome are immunoreactive to [1] S-100 protein, [2] “pan-macrophage” antigens such as EBM [11], HAM 56, and Leu-M3, [3] antigens functionally associated with phagocytosis (Fc receptor for IgG, complement receptor 3), and lysosomal activity (lysozyme, alpha 1-antichymotrypsin, and alpha 1-antitrypsyn), [4] antigens associated with early inflammation (Mac-387, 27E10), [5] antigens commonly found on monocytes, but not tissue macrophages (OKM5, Leu-M1), and [6] “activation” antigens (Ki-1 and receptors for transferrin and interleukin 2). These data suggest that SHML cells are true functionally activated macrophages that may be recently derived from circulating monocytes [11]. However , these marker studies could not be done in our patient because they were not available. The reports of MRI findings in this case was normal. FNAC was also done but was not contributory. Thus histopathology plays an important role in making a definitive diagnosis. There is no ideal treatment but options range from surgery, radiotherapy and steroids to chemotherapy [12]. The disease typically pursues an indolent clinical course. In approximately 50% of patients , the disease resolves with out any sequelae , one third have residual asymptomatic adenopathy and 17% have persistent sympyomatology after 5 to 10 years [12]. in our patient was on steroid therapy for one year. To conclude, Rosai-Dorfman disease should be considered in the differential diagnosis of granulomatous infection, pseudogranulomatous lesion and malignancy.
[1]. Rosai J, Dorfman RF, Sinus histiocytosis with massive lymphadenopathy. A newly recognized benign clinicopathological entityArch Pathol 1969 87:63-70. [Google Scholar]
[2]. Azoury FJ, Reed RJ, Histiocytosis. Repirt of an unusual caseN Engl Med 1966 274:928-30. [Google Scholar]
[3]. Bhasker V, Swamy K, Reddy BK, Supe SS, Kumar RV, Sinus histiocytosis with nodal and extranodal involvement. A case reportJ Indian Med Assoc 2003 101:28-30. [Google Scholar]
[4]. Faucar E, Rosai J, Dorfman RF, Sinus histiocytosis with massive lymphadenopathy (Rosai – Dorfman Disease): review of the entitySemin Diagn Pathlo 1990 7:19-73. [Google Scholar]
[5]. Foucar E, Rosai J, Dorfman RF, Sinus histiocytosis with massive lymphadenopathy. An analysis of 14 deaths occurring in a patient registry.Cancer 1984 Nov 1 54(9):1834-40. [Google Scholar]
[6]. Kare M, Dang S, Dang A, Rosai- Dorfman syndrome with Sinonasal Mucosa and Intraocular InvolvementJAPI June 2007 Vol 55 [Google Scholar]
[7]. Fudenberg HH, Good RA, Hitzig W, Classification of the primary immune deficiencies : WHO recommendationN Engl J Med 1970 283:656-7. [Google Scholar]
[8]. Middel P, Hemmerlein B, Fayyazi A, Kaboth U, Radzun HJ, Sinus histiocytosis with massive lymphadenopathy: evidence for its relationship to macrophages and for a cytokine-related disorderHistopathology 1999 Dec 35(6):525-33. [Google Scholar]
[9]. Humble JG, Jaynee WHM, Pulvertaft RJ, Biological interaction between lymphocyte and other cellsBr J Hematol 1956 2:283 [Google Scholar]
[10]. Lopes LF, Bacchi MM, Coelho KI, Filho AA, Bacchi CE, Emperipolesis in a case of B-cell lymphoma: A rare phenomenon outside of Rosai-Dorfman diseaseAnn Diagn Pathol 2003 Oct 7(5):310-3. [Google Scholar]
[11]. Eisen RN, Buckley PJ, Rosai J, Immunophenotypic characterization of sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease)Semin Diagn Pathol 1990 Feb 7(1):74-82. [Google Scholar]
[12]. Raveenthiran V, Dhanlaxmi M, Hayavadana Rao PV, Vishwanathan P, Rosai dorfman disease: report of a 3 year old girl with review of treatment optionsEur J Paediatric Surg 2003 13:350-4. [Google Scholar]