“Redefining Smile-A Multidisciplinary Approach”
Prakash Manne1, Srujana Zakkula2, Jyothi Atla3, Suresh Babu Muvva4, Anche Sampath5
1 Professor, Department of Prosthodontics, SIBAR Institute of Dental sciences, Guntur-9, India.
2 PG Student, Department of Prosthodontics, SIBAR Institute of Dental Sciences, Guntur, AP, India.
3 Assistant Professor, Department of Prosthodontics, SIBAR Institute of Dental sciences, Guntur-9, India.
4 Assistant Professor, Department of Prosthodontics, SIBAR Institute of Dental sciences, Guntur-9, India.
5 Reader, Department of Prosthodontics, SIBAR Institute of Dental sciences, Guntur-9, India.
Name, Address, E-Mail Id of The Corresponding Author: Dr Jyothi Atla, Assistant Professor, Department of Prosthodontics, SIBAR Institute of Dental sciences, Guntur-9, India.
Phone: 9492776417
E-mail: drjyothimds@gmail.com
This article presents a case report of a 20 year old female who was very much dissatisfied with her facial appearance and smile.On examination, it was found that there was a Angles class II division 1 malocclusion and a generalised spacing in the anterior teeth, with a retained, deciduous, left maxillary canine and a malposed 15. On radiographic examination, an impacted 18, 23 was noticed. As the part of the treatment plan, the retained deciduous canine and the impacted permanent canine were extracted and an orthodontic correction of the malocclusion was accomplished. The missing canine was planned to be replaced with a fixed partial denture.The short clinical crown height of the abutment teeth was increased by crown lengthening procedures and the pontic space was contoured to receive a ovate pontic by using diode lasers. The missing tooth was restored by using an all ceramic three unit zirconia bridge. This multi–disciplinary approach improved the smile of the patient and it ultimately enhanced her aesthetics and self confidence.
Class II division I malocclusion, Edge wise appliance MBT 0.022 slot, Impacted canine, Crown lengthening, Diode lasers, Ovate pontic, Zirconia bridge
Case Report
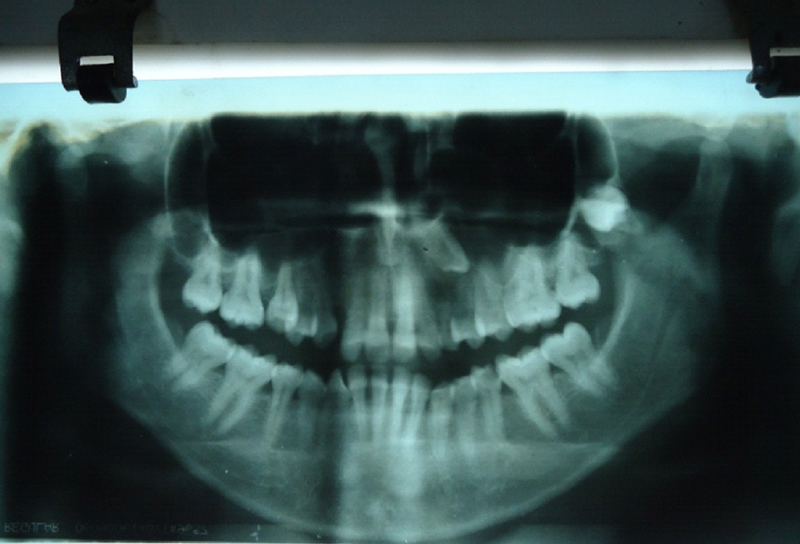
A 20-year-old female reported to the SIBAR Institute of Dental Sciences, with the chief complaint of a disproportionate display of teeth [Table/Fig-1]. On intra–oral examination, it was found that there was a Angles class II division 1 and a generalised spacing in the anterior teeth, with a retained deciduous left maxillary canine [Table/Fig-2] and a malposed 15. On radiographic examination, an impacted 18, 23 was noticed [Table/Fig-3].

Pre–operative intraoral view

The treatment plan was explained and a written consent was taken from the patient. The treatment plan involved extraction of the impacted teeth, orthodontic correction of the malocclusionwith a Pre–adjusted edge wise appliance MBT 0.022 slot [Table/Fig-4], crown lengthening of the abutment teeth,and recontouring of the pontic space by using a diode laser. The amount of soft tissue recontouring in the pontic region was determined by the proximity of the underlying bone, the final aesthetics and the emergence profile of the pontic. A radiographic and probing assessment revealed sufficient sulcular depth which could allow the removal of sufficient amount of gingival marginal tissues, which was consistent with the desired outcome.
Abutments-compromised clinical crown height
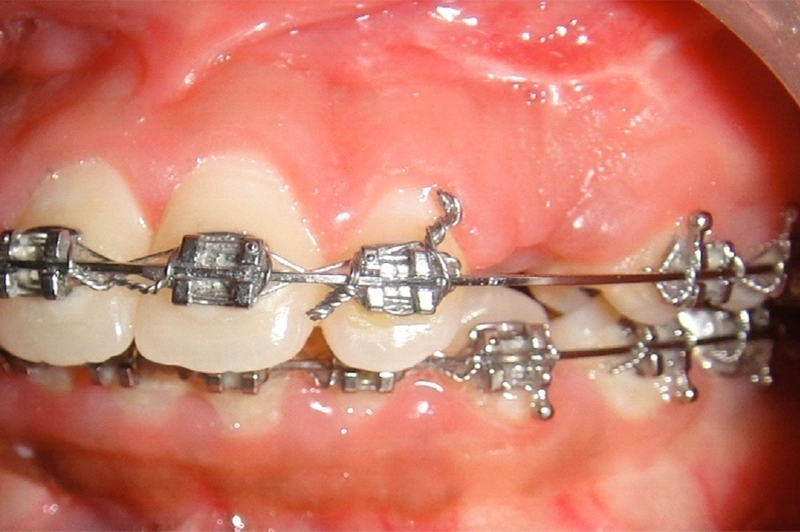
There was sufficient free gingival margin which could allow a simple gingivoplasty procedure at the abutment and adequate soft tissue for the pontic space modification. It was deemed appropriate to remove 2 mm of gingival tissue, and the need for accuracy demanded the use of a contact–mode fibre delivery laser. In this case presentation, an 810–nm diode laser (DENLASE) was used to establish the clinical crown lengthening and the pontic space modification [Table/Fig-5]. A study which was done on the clinical evaluation of the crown lengthening by Shobha et al had concluded that the biologic width can be re–established to its original vertical dimension along with 2 mm gain of coronal tooth structure at the end of six months [1].
Crown lengthening and pontic space modification with diode Laser

This procedure was accomplished by using a diode laser of wavelength 810-nm (DENLASE). The other parameters include the Beam diameter: 320 lm, the Emission mode: Gated pulse wave, the Delivery: quartz fiber–contact mode, the Average power: 1.5 W and the Exposurse time: 1.0 minutes per tooth.
Following infiltration and local anaesthesia (2%lidocaine, 1:80,000 epinephrine), the gingival tissue was incised with the laser to a point at which a separation was anticipated. In order to preserve the contours and the crown length, the abutments were prepared and the provisional restorations were fitted on the same day [Table/Fig-6]. At the one week’s recall visit, the healing was found to be uneventful and the patient had neither post–operative complaints nor any discomfort. At 2 weeks, the final impressions were taken, at which stage the soft tissue surgical sites appeared healed, firm, and healthy. The prosthetic stages proceeded as per the normal restorative treatment and a 6-month post–operative view of the final all ceramic bridge showed good adaptation of the gingival tissues at the crown margins [Table/Fig-7]. The patient’s consent was taken for presenting her pictures for publication.
Cemented Provisional restoration


Discussion
During the early times, the conventional surgical techniques (scalpel gingival recontouring) were the main treatment modalities for performing soft tissue surgeries [2]. Although the dental laser was initially introduced in 1959, the entire practice of dentistry has been revolutionizedever sinceLasers for dental applications were introduced in 1985 [3]. For most of the soft tissue surgeries, lasers were aviable treatment option. Some of the authors used the Nd:YAG laser fordefining the emergence profile of the abutment and the pontic space in a combined natural tooth/implant–supported fixed prosthesis. Stuart Coleton utilized the CO2 laser which was set at 4 W in a continuous wave for performing gingivoplasty procedures [4]. Govila V, Gulati M and Govila M, in 2011, performed various soft tissue surgical procedures like frenectomies,gingivoplasties,gingivectomies,vestibuloplasties, depigmentations and second stage implant surgeries by using diode lasers and they achieved significant results [5]. Kenneth used a diode laser to correct the gummy smile of a patient [2].
In the present case, we made use of a 810 nm gated pulse wave diode laser to recontour the tissues and also for crown lengthening. The teeth were prepared and the provisional restorations were given on the same day of the surgery, in order to maintain the surgically gained space. The clinical crown height and the gingival contour which were achieved with the laser therapy were highly remarkable.The ovate pontic which was initially described in the year 1933, was chosen as the pontic design, as it has been suggested to accurately duplicate the emergence profile for the natural teeth, in order to provide an aesthetic, cleanable prosthesis, a pleasing appearance and strength and also, it could act as a matrix for the formation of the stratified squamous epithelium. After two weeks, the patient was recalled and a permanent zirconia prosthesis with an ovate pontic design was fabricated and it was cemented in the patient’s mouth. All the ceramic restorations provide a solution for the patients with highaesthetic demands. The monolithic zirconia restorations have been proved to be the most popular materials for restoring the anterior single crowns and a full mouth rehabilitation and also for the patients with para–functional habits. The ceramic zirconia prosthesis which was cemented had an excellent colour match, which ultimately enhanced the aesthetics and the beauty of her smile.
[1]. Robbins JW, Tissue management in restorative dentistryFunct Esthet Restor Dent 2007 1:40-43. [Google Scholar]
[2]. Magid KS, Strauss RA, Laser Use for Esthetic Soft Tissue ModificationDent Clin N Am 2007 51:525-45. [Google Scholar]
[3]. Moritz A, Oral laser applicationQuintessence publication 2006 :274-75. [Google Scholar]
[4]. Coleton S, Lasers in surgical periodontics and oral medicineDent Clin N Am 2004 48:937-62. [Google Scholar]
[5]. Govila V, Gulati M, Govila M, Diode laser applications in periodonticsIJDS 2011 3:64-67. [Google Scholar]