A Report of an Indian Boy with a Delayed Diagnosis of Pseudochondroplasia
Ankur Singh1, T Abiramalatha2, Gaurav Pradhan3, Dong- Kyu Jin4, Seema Kapoor5
1 Senior Research Associate, MAMC Associated Lok Nayak Hospital, New Delhi, India.
2 Pediatrics, MAMC Associated Lok Nayak HospitalNew Delhi, India.
3 Department of Radiology, MAMC Associated Lok Nayak Hospital, New Delhi, India.
4 Professor, Department of Pediatrics, Samsung Medical Center Sungkyumkwan University, Seoul Korea.
5 Professor Pediatrics, MAMC Associated Lok Nayak Hospital, New Delhi, India.
Name, Address, E-Mail Id of The Corresponding Author: Dr Seema Kapoor, M-439, Ground Floor, Guruharkishan Nagar, Paschim Vihar, New Delhi, India.
Phone: 9968604313
E-mail: drseemakapoor@gmail.com
The mutations in the Cartilage Oligomeric Matrix Protein (COMP) gene are associated two common and allelic bony dysplasias: Psuedoachondroplasia (PSACH) and Multiple epiphyseal dysplasias-1 (MED-1). The characteristic radiological features of both has been well established in the literature, with areas of overlap between the two in certain forms of mild PSACH and severe MED. MED is also a genotypically and a phenotypically heterogeneous disease. Here, we emphasise the salient radiological features which aid in the diagnosis of PSACH and COMP MED; which may enable a targeted molecular analysis.
Pseudochondroplasia, Multiple Epiphyseal Dysplasia, COMP gene
Introduction
Pseudoachondroplasia (PSACH) and Multiple Epiphyseal Dysplasia type 1 (MED1) are autosomal dominant skeletal dysplasias which are caused by mutations in the COMP gene. PSACH manifests around 2 years of age and it is characterised by a moderate to severe short stature, deformities of the lower limbs, vertebral anomalies and early onset progressive osteoarthritis. MED 1, on the other hand, is characterised by an onset in mid or late childhood, a mild to moderate short stature and a normal spine. The radiological changes progress and they change or evolve with increasing age and if they are seen later, it may be difficult to differentiate between mild PSACH and severe COMP MED. The COMP gene mutations, though they are available as clinical tests, are expensive. So, we attempted to highlight the salient features which could help the clinicians in making the decision of COMP testing.
Case Report
A 9-years old male child presented with a short stature and bony deformities. He was born of a non – consanguineous parentage. The antenatal and the perinatal periods were uneventful. The child’s growth was normal till the age of two years. Thereafter, he started showing a decrease in the growth velocity and he developed lower limb deformities. The child achieved his developmental (motor, fine motor, language, personal and social) milestones normally and he presently studies in class seventh and is doing average in studies.
On examination, he was found to have a severe short stature with a height of 92cm (< - 3 SD scores) with disproportionately short limbs (US/LS= 1.24). He had micromelia and his arm span was 82 cm. He had widening at all the joints, a bilateral genu varus deformity, a waddling gait and short stubby fingers. He did not have any dysmorphic facial features, contractures or kyphoscoliosis. He had a normal dentition and a normal IQ (IQ-110, was assessed by DASII). His systemic examination was normal.
Radiography revealed a marked flaring of the metaphyses at all the joints [Table/Fig-1 and 2]. The epiphyses were fragmented and deformed, with a delay in their ossification [Table/Fig-1]. The carpal bones were deformed and there was a markedly delayed carpal bone age [Table/Fig-3]. The spine showed undulations of the superior and the inferior plates of the multiple dorsolumbar vertebrae, which resembled Schmorl’s nodes and anterior tonguing [Table/Fig-4 and 5]. An X-ray of the pelvis showed bilateral iliac flaring, coxa vara and a tri radiate acetabulum [Table/Fig-6].
Radiography revealed marked flaring of the metaphyses at all the joints ,epiphyses were fragmented, deformed with delay in ossification.

Small ,late appearing epiphysis and flared, ragged metaphyses

The carpal bones were deformed and there was a markedly delayed carpal bone age

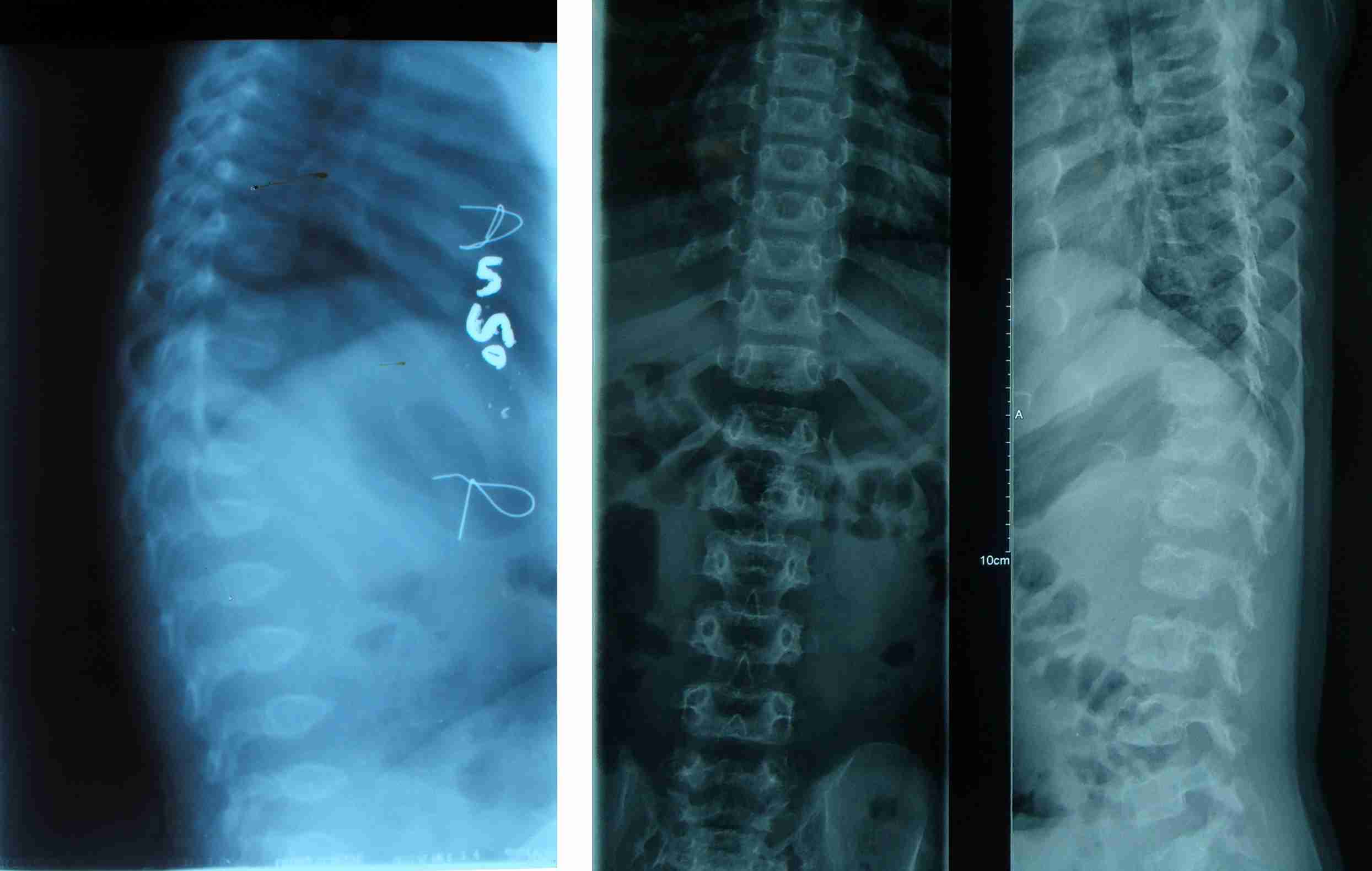
Spine showed undulations of the superior and inferior plates of multiple dorsolumbar vertebrae resembling Schmorl’s nodes and anterior tonguing
X-ray pelvis showed bilateral iliac flaring, coxa vara and tri radiate acetabulum

The skull radiograph was normal, with a J shaped sella. His bone age (4 – 5 years) was markedly delayed, as was assessed by the Greulich and Pyle method. His baseline investigations were within normal limits. His thyroid function tests were normal. Based on his history and radiographic examination, a working diagnosis of PSACH, MED and Spondylometaepiphyseal dysplasia was suspected. His mutational analysis revealed a novel de novo missense mutation in the exon 14 of the COMP gene [c.1554C>G (p.Asp518Glu)].
Discussion
PSACH and MED are a group of osteochondrodysplasias with variable phenotypes and heterogeneous genotypes. PSACH has a single genetic locus (19p13.11) with single gene (COMP) involvement, whereas MED has multiple genetic loci (19p13.11, 1p33-p33.2, 20q13.3, 5q32-q33.1, 2p24-p23,6q13) with multiple gene involvements (COMP, COL9A2, COL9A3, SLC26A2, MATN3, COL9A1). PSACH has frequency of 4 per million population, while MED has high frequency of 9-16 per million [1,2,3]. PSACH and MED [1–3, 5,6] are inherited in an autosomal dominant manner, except MED4, which is inherited in an autosomal recessive form. COMP-MED is the commonest of all the six MEDs and it is allelic to PSACH. The COMP mutations are responsible for these two allelic disorders [4,5].
COMP is a modular protein which comprises the amino- terminal coiled- coil oligomerization domain, 4 type II (EGF –like) domains, 8 type III Calmodulin like repeats (CLR) and a C – terminal globular domain (CTD); which are expressed in cartilage, tendons and ligament [6]. A majority of the COMP mutations (85 %) are clustered in the CLR repeats [7]. The COMP gene is comprised of 19 exons, with the maximum number of missense mutations clustering in the exons 13 and 14 [8]. Exon 14 is comprised of the CLR and the CTD domains. We found a missense mutation (c.1554C>G) in exon 14 in the CLR domain of chromosome 19, which had led to a protein change (p.Asp5218Glu). The calmodulin like repeats are highly conserved and so any change which involves the aspartic acid residue will lead to functional and conformational changes in the COMP gene product. This mutation was absent in the parents, sibs and and in the ethnic controls. Thus, it was a de novo pathogenic mutation, which was later substantiated by doing an in silico analysis.
PSACH and COMP-MED represents the two ends of a clinical spectrum, with many cases falling in between the two extremes. It is not unusual for PSCAH to get diagnosed as late as our present case (9 years). Hence, a diagnostic dilemma occurred, as this is the period of presentation of MED-1. It is difficult to distinguish mild PSACH from very severe MED, thus delaying the correct radiological diagnosis. There are certain radiological signs which have been designated as COMPY [Table/Fig-7] that can guide the clinicians in the COMP mutation testing [9].
Radiographic MED with “COMPY” changes (suggesting COMP mutations)
| Pelvis |
|---|
Very small capital femoral epiphysis Hypoplastic, poorly formed acetabular roofs.
|
| Knees |
Metaphyseal widening and irregularity.
|
| Hands |
Brachydactyly Proximal metacarpal rounding
|
| Spine |
Indentations of superior and inferior ring epiphyseal regions (early age)
|
We tabulated the radiological findings of our case and compared them with the characteristic radiological findings of PSACH and COMP-MED [Table/Fig-8]. The following radiological findings strongly favoured the diagnosis of PSACH- an anterior tongue, biconvex vertebrae, platyspondyly (Spine); short tubular bones with a frayed metaphysis and a fragmented epiphysis (All the large joints); a tri radiate appearance of the acetabulum with a short and beaked femoral neck (Pelvis). The findings which were characteristic of COMP-MED were- vertebral end plate irregularities with Schmorl bodies (Spine) and a delay in the appearance of the carpal/tarsal bones. However, a generalised epiphyseal ossification delay and deformed carpal/tarsal bones were the common radiological features which were seen in both. Thus, our case demonstrated major radiological findings which were suggestive of PSACH, which shared a few radiological features of COMP MED. So, tabulating and comparing the radiological features helped in predicting the correct phenotype and in targeting the molecular study to the COMP gene rather than to other genetic loci in MED.
Comparison of Radiographical findings of our case with characteristic PSACH and COMP-MED findings
| Radiograph | Psuedoachondroplasia (PSACH) | COMP-MED | OUR CASE |
|---|
| Skull | Normal | Normal | Normal |
| Odontoid process | Absent, hypoplastic, Normal | Normal | Normal |
| Spine (Lateral View) | Anterior tounge,Biconvex vertebra (Early features), Platyspondyly (Late feature) | Sometimes schmorl bodies@ vertebral endplate irregularities present | Anterior Tongue, biconvex vertebrae, (Present in 3 year old x ray) [Table/Fig-1]; vertebral end plate irregularities with schmorl bodies [Table/Fig-2] |
| Spine (Anterior) | Platyspondyly | Essentially normal | Platyspondyly [Table/Fig-2]
|
| Shoulder joint/ Elbow joint/ Wrist joint | Marked flaring of metaphysis, Fragmented epiphysis, Delay in ossification | Ossification delay in epiphysis, ossification centres are small and irregular in contour (Seen more in knee and hip joint), Metaphysis normal | Marked flaring of metaphysis, Fragmented epiphysis, epiphyseal ossification delay [Table/Fig-3] |
| Pelvis and Hip Joint | Slow development of Triradiate cartilage of acetabulam, Capital femoral epiphysis ossification delay, Femoral neck appears short and beaked. | Capital femoral epiphysis remains small ,round ,significant delay in maturation | Tri radiate appearance of acetabulum, Capital femoral epiphysis ossification delay, Femoral neck appear short and beaked. [Table/Fig-4] |
| Knee joint /Ankle joint | Small, late appearing epiphysis and flared, ragged metaphyses | Distal femoral and proximal tibial epiphyses are too small for chronological age. | Small, late appearing epiphysis and flared, ragged metaphyses [Table/Fig-5] |
| Hand /Feet | Small, Irregular carpals/tarsals, Proximal pointing of metacarpals/metatarsals, Epiphysis of phanages are small. | Delay in appearance of carpal/tarsal bones, contour is irregular, Phalanges epiphysis round and cone shaped | Deformed carpal /tarsals bones, Delay in appearance of carpal/tarsal bones, Epiphyses are round and irregular with ossification delay [Table/Fig-5 and 6] |
Note-Findings in BOLD LETTERS favour PSACH, Findings in ITALICS favour COMP-MED, Findings in UNDERLINED TEXT favour BOTH
To conclude, this is a case of PSACH with an overlap of some features of COMP MED. It shared two unusual features of COMP MED- vertebral end plate irregularities with Schmorl bodies and a delay in the appearance of the carpal and the tarsal bones. Though the features were classical of PSACH, the diagnosis was delayed till 9 years of age. There are psychological and treatment implications of making a late diagnosis and so, we emphasise an early diagnosis in the prototype patients and highlight certain radiological clues in milder PSACH and COMP MED, to direct the COMP gene testing to reach a correct molecular diagnosis.
Note-Findings in BOLD LETTERS favour PSACH, Findings in ITALICS favour COMP-MED, Findings in UNDERLINED TEXT favour BOTH
[1]. Andersen PE Jr, Hauge M, Congenital generalised bone dysplasias: a clinical, radiological, and epidemiological surveyJ Med Genet 1989 26:37-44. [Google Scholar]
[2]. Khungar A, Mahajan P, Gupte G, Vasundhara M, Kher A, Pseudoachondroplastic dysplasiaJ. Postgrad. Med 1993 39:91-93. [Google Scholar]
[3]. Wynne-Davies R, Gormley J, The prevalence of skeletal dysplasias. An estimate of their minimum frequency and the number of patients requiring orthopaedic careJ Bone Joint Surg Br 1985 67:113-17. [Google Scholar]
[4]. Briggs MD, Hoffman SM, King LM, Olsen AS, Mohrenweiser H, Pseudoachondroplasia and multiple epiphyseal dysplasia due to mutations in the cartilage oligomeric matrix protein geneNat Genet 1995 10:330-36. [Google Scholar]
[5]. Hecht JT, Nelson LD, Crowder E, Wang Y, Elder FF, Mutations in exon 17B of cartilage oligomeric matrix protein (COMP) cause pseudoachondroplasiaNat Genet 1995 10:325-29. [Google Scholar]
[6]. Hecht JT, Deere M, Putnam E, Cole W, Vertel B, Characterization of cartilage oligomeric matrix protein (COMP) in human normal and pseudoachondroplasia musculoskeletal tissuesMatrix Biol 1998 17:269-78. [Google Scholar]
[7]. Kennedy J, Jackson GC, Barker FS, Nundlall S, Bella J, Novel and recurrent mutations in the C-terminal domain of COMP cluster in two distinct regions and result in a spectrum of phenotypes within the pseudoachondroplasia – multiple epiphyseal dysplasia disease groupHum Mutat 2005 25:593-94. [Google Scholar]
[8]. Jackson GC, Mittaz-Crettol L, Taylor JA, Mortier GR, Spranger J, Pseudoachondroplasia and multiple epiphyseal dysplasia: a 7-year comprehensive analysis of the known disease genes identify novel and recurrent mutations and provides an accurate assessment of their relative contributionHum Mutat 2012 33:144-57. [Google Scholar]
[9]. Lachman RS, Krakow D, Cohn DH, Rimoin DL, MED, COMP, multilayered and NEIN: an overview of multiple epiphyseal dysplasiaPediatr Radiol 2005 35:116-23. [Google Scholar]