An Abdominal Flap to Save the Right Forearm and the Hand, Following a High-voltage Electric Burn in a Child: A Case Report
Sharad Khandelwal1
1 Associate Professor, Department of General Surgery, Sri Aurobindo Institute of Medical Sciences, Indore, Madhya Pradesh – 453111, India.
Name, Address, E-Mail Id of The Corresponding Author: Dr Sharad Khandelwal, Associate Professor, Department of General Surgery, Sri Aurobindo Institute of Medical Sciences, Indore, Madhya Pradesh – 453111, India. Phone No: +91-731-2591131, 9755880888
E-mail: drsharadkh@gmail.com, drskhandelwal@sify.com
High – voltage electric burns are very rare in children. This is a report of a seven years old boy, who presented 20 days after severe burns following a contact with a high – voltage electric line during playing. He was treated for the above at another hospital and was referred for further management. His clinical examination revealed; exposed skull bones, a raw area over the right side of the chest wall and a raw area over the right upper limb, which completely exposed the distal radius and the ulnar bones. After properly explaining the purpose of the operation to his parents and getting their consent, the exposed skull bones were covered with multiple pedicle scalp flaps. A bipedicle abdominal flap was used to cover the exposed right forearm bones and a skin grafting was also provided to the chest wall wound at the same time. The abdominal flap was detached safely after three weeks. He withstood the above operations well and was discharged six weeks after the above operations. The bipedicle abdominal flap helped in saving his right forearm and hand and the reason for the publication of this case is its rarity in children.
Abdominal flaps, High-tension electric burn injuries, Pedicle flaps, Reconstructive surgery
Introduction
An improved understanding of the pathophysiology and the advances which have been made in burn management over the past 50 years, have contributed immensely to the dramatic rise in the survival and the reduced morbidity which result from major burn injuries [1]. Electrical burn injuries occur due to a contact with live electric wires or lightning. These electrical injuries are classified under major burns [1]. High-voltage electricity can cause devastating injuries which may result in major soft-tissue loss and limb loss and sometimes they pose a major threat to life [2]. A majority of the patients, following high – voltage electric burn injuries, required surgical interventions in the form of distant pedicle flaps, local pedicle flaps, free flaps, skin grafting, microvascular reconstructions, and limb amputations [2–5]. Herein, I’m reporting a seven years-old boy who sustained high – voltage severe electric burn injuries over the head, chest wall, and the right upper limb and hand. A bipedicle abdominal flap helped in saving his right forearm and hand.
Case Report
A seven years old boy was referred 20 days after getting a severe, high-voltage electric burn over his head, chest and right upper limb. He had an accidental contact with a high – voltage electric wire during playing. He was treated for the same for 20 days at other hospital and was referred for further management. His clinical examination revealed a burn area over the culvarium (cranium), with an exposed skull bone [Table/Fig-1]. The examination of his chest wall revealed a raw area with good granulation tissues over the right anterior and lateral chest wall [Table/Fig-2]. His right upper limb revealed a raw area which exposed the radius and the ulnar bones over the forearm, with no interviewing soft tissue/muscle over it [Table/Fig-3]. There was only a thin streak of granulation tissue over the radius, which probably contained the radial artery. The right hand looked clinically good, with a good blood supply. After explaining the purpose of the operation and providing counselling, consent of his parents was obtained; the exposed skull bones were covered with multiple pedicle scalp flaps. A bipedicle abdominal flap was used to cover the exposed right forearm bones [Table/Fig-4] and a skin grafting was also provided to the chest wall wound and the upper limb at the same time. The abdominal flap was detached safely after three weeks. At few places, a skin grafting was needed again to cover the raw area. He withstood the above operations well. The pedicle scalp flaps were accepted well over the exposed skull bones [Table/Fig-5]. The cosmetic appearance (following the above operations) of the upper limb was good [Table/Fig-6a] and acceptable to patient and as well as to his parents and he was also able to hold his limb [Table/Fig-6b] with limited movements. He was advised active and supervised physiotherapy and was discharged six weeks after the above operations. He was lost to follow up after three months of surgery. The bipedicle abdominal flap helped in saving his right forearm and hand.
Clinical photograph showing exposed skull bones

Clinical photograph showing chest wall and right upper limb wounds

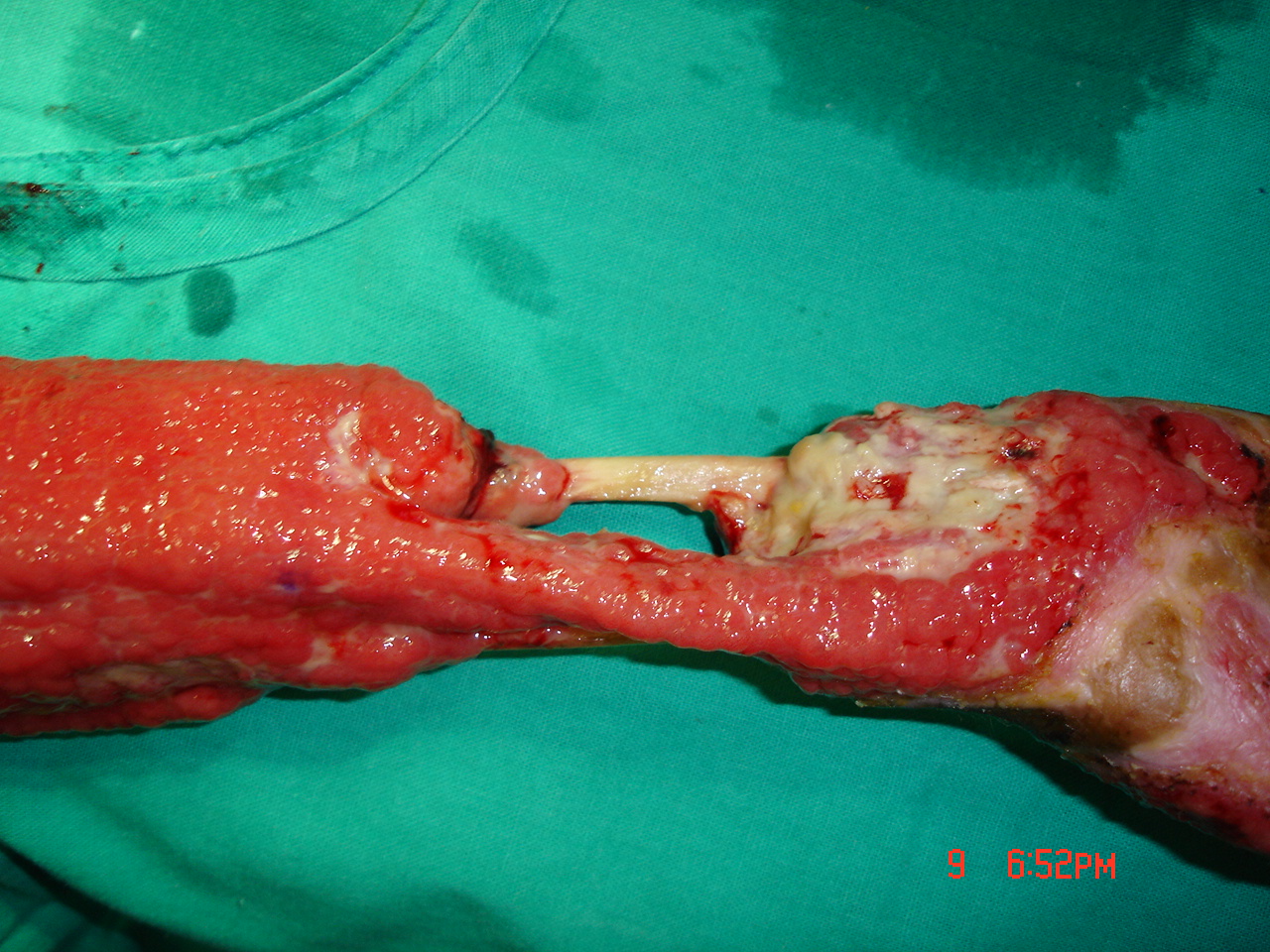
Right forearm (prone) showing exposed radius and ulnar bones
Photograph showing bi-pedicle abdominal flap for exposed radius and ulna

Post-operative photograph showing well accepted scalp flaps

Early post-operative photograph showing right upper limb

Photograph showing cosmetically acceptable right upper limb

Discussion
Although electric burn injuries (EBIs) are not frequent, they remain a serious problem [4]. Extensive damage to the deeper tissues (muscles, blood vessels and nerves, etc) may be present beneath the intact and unburned skin [1]. A thermal injury may also occur due to ignition of the clothing after the electric contact. Cardiac arrhythmias and ECG changes may be seen within the first few hours following EBIs [1]. The upper extremities remain the most frequently involved sites of injuries following EBIs. The causes of EBIs, in the order of frequency, are work related accidents, home accidents, high tension injuries and electrocution [6,7].
The management of the patients with EBIs consists of a management of the burn itself and its complications. A majority of the patients with EBIs also require surgical therapy in the form of distant pedicle flaps, local pedicle flaps, free flaps, micro – vascular reconstructions, skin grafting, and limb amputations [2–5,8]. Many a times, amputation of the limb is needed following a high-voltage electric injury to the limb and it is considered as one of the most devastating consequences of the electric injury [9]. Rehabilitation is an essential and integral part of the burn treatment. The aims of burn rehabilitation are to minimize the adverse effects which are caused by the injury, maintaining the range of the movement, minimizing the contracture development and scarring, maximising the functional ability and the psychological wellbeing, etc [10].
The present patient was a seven years old boy who sustained injuries over his head, thorax and right upper limb following a contact with a high – voltage electric current during playing. He was successfully managed with multiple surgeries, which included pedicle scalp/local flaps for the scalp wound, skin grafting for the chest wound, and a pedicle abdominal flap for preserving the forearm and the hand. His post-operative result was cosmetically acceptable to the patient and to his parents as well. In the present case, the most important and challenging fact was to save the child’s forearm and hand and that was successfully achieved with the help of a bipedicle abdominal flap.
[1]. Shrivastava P, Goel A, Pre-hospital care in burn injuryIndian J Plast Surg 2010 43:15-22. [Google Scholar]
[2]. Koul AR, Patil RK, Philip VK, Early use of microvascular free tissue transfer in the management of electrical injuriesBurns 2008 34:681-87. [Google Scholar]
[3]. Xie WG, Wang DY, Liu JF, Long ZH, Li J, Jiang MJ, Repair of electrical burns on hands with flapsZhonghua Shao Shang Za Zhi 2010 26:30-3. [Google Scholar]
[4]. Celik A, Ergün O, Ozok G, Pediatric electrical injuries: a review of 38 consecutive patientsJ Pediatr Surg 2004 39:1233-7. [Google Scholar]
[5]. Ofer N, Baumeister S, Megerle K, Germann G, Sauerbier M, Current concepts of microvascular reconstruction for limb salvage in electrical burn injuriesJ Plast Reconstr Aesthet Surg 2007 60:724-30. [Google Scholar]
[6]. Sheikhazadi A, Kiani M, Ghadyani MH, Electrocution-related mortality: a survey of 295 deaths in Tehran, Iran between 2002 and 2006Am J Forensic Med Pathol 2010 31:42-5. [Google Scholar]
[7]. Shen YM, Hu XH, Mi HR, Yu DN, Qin FJ, Chen H, Early treatment of high-voltage electric burn wound in the limbsZhonghua Shao Shang Za Zhi 2011 27:173-7. [Google Scholar]
[8]. Baumeister S, Köller M, Dragu A, Germann G, Sauerbier M, Principles of microvascular reconstruction in burn and electrical burn injuriesBurns 2005 31:92-8. [Google Scholar]
[9]. Hsueh YY, Chen CL, Pan SC, Analysis of factors influencing limb amputation in high-voltage electrically injured patientsBurns 2011 37:673-7. [Google Scholar]
[10]. Procter F, Rehabilitation of the burn patientIndian J Plast Surg 2010 43:101-13. [Google Scholar]