Median Raphe Cysts of the Prepucial Skin, with Triple Histological Linings: A Case Report and Review of the Literature
Anandhi Amaranathan1, Sankappa P. Sinhasan2, Simon David Dasiah3
1 Assistant Professor, Department of Surgery, Indira Gandhi Medical College & Research Institute (IGMC & RI), Pondicherry–605009, India.
2 Associate Professor, Department of Pathology, Indira Gandhi Medical College & Research Institute (IGMC & RI), Pondicherry–605009, India.
3 Head of the Department, Department of Surgery, Indira Gandhi Medical College & Research Institute (IGMC & RI), Pondicherry–605 009, India.
Name, Address, E-Mail Id of The Corresponding Author: Dr Anandhi Amaranathan, 12, New Street, Shanthi nagar, Lawspet, Pondicherry–605008, India.
Phone: +91 9487781661
E-mail: anandhiramesh76@yahoo.in
A median raphe cyst is an uncommon entity. An extensive literature search has revealed only less than 200 reported cases. Among these, only less than 10 have been reported from the Indian subcontinent. Usually, it is located in the midline, anywhere between the urethral meatus and the anus. We are presenting a case of a prepucial median raphe cyst, which occurred at a very uncommon location, which presented with symptoms, which is also a rare scenario. This case has been presented for its rare location, uncommon clinical presentation and an interesting triple lining presentation in histology.
Median raphe cyst, Penile cyst, Prepucial cyst
Introduction
A median raphe cyst is an uncommon congenital cyst which presents itself anywhere between the tip of the penis and the anus, along the midline and it is usually asymptomatic. When it presents close to the meatus, it is also mentioned as a ‘parameatal cyst’ [1]. So, the commonly reported sites of occurrence are the shaft of the penis and the glans penis. We are presenting a case of a prepucial median raphe cyst which presented with symptoms in a young adult of Indian origin.
Case Report
A 27 years old Indian male came to the surgery outpatients clinic with the complaint of a swelling in the foreskin. It was present from his childhood and it had gradually increased in size. All these years, the swelling was asymptomatic, but he developed pain and discomfort during sexual intercourse. There was no other relevant clinical history.
On clinical examination, a 2 x 2 cm, smooth, globular swelling was found to be present in the prepuce, on the ventral side [Table/Fig-1]. It was not tender, the skin over the swelling was normal and it was not attached to the glans penis or to the body of the penis. Considering the size, site and the nature of the swelling, we decided to do circumcision and an excision biopsy of the lesion was done, with only the basic haematological investigations. The post operative follow up of 18 months revealed no recurrence.
Pre-operative photograph showing globular swelling present over the prepucial skin on the ventral side of penis

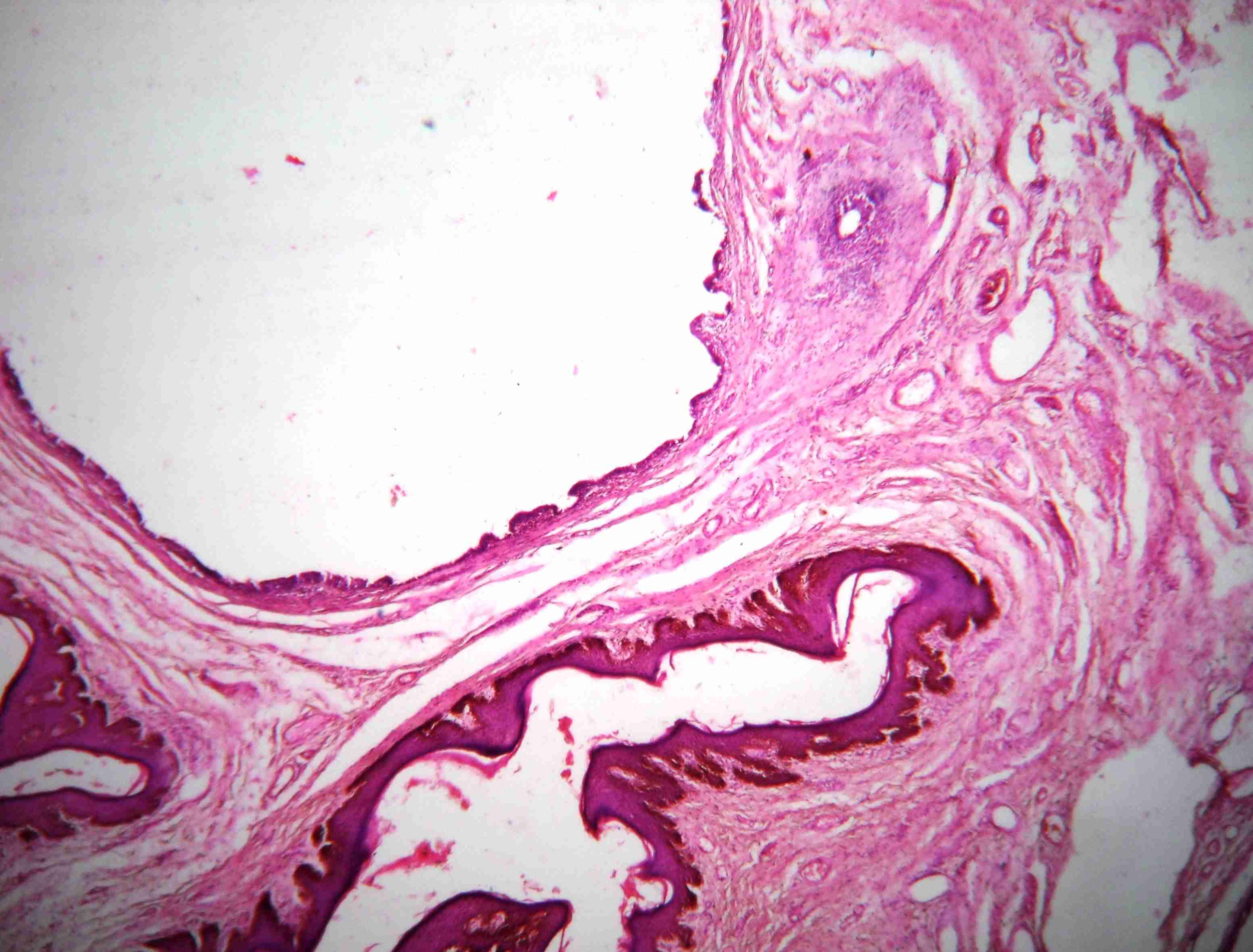
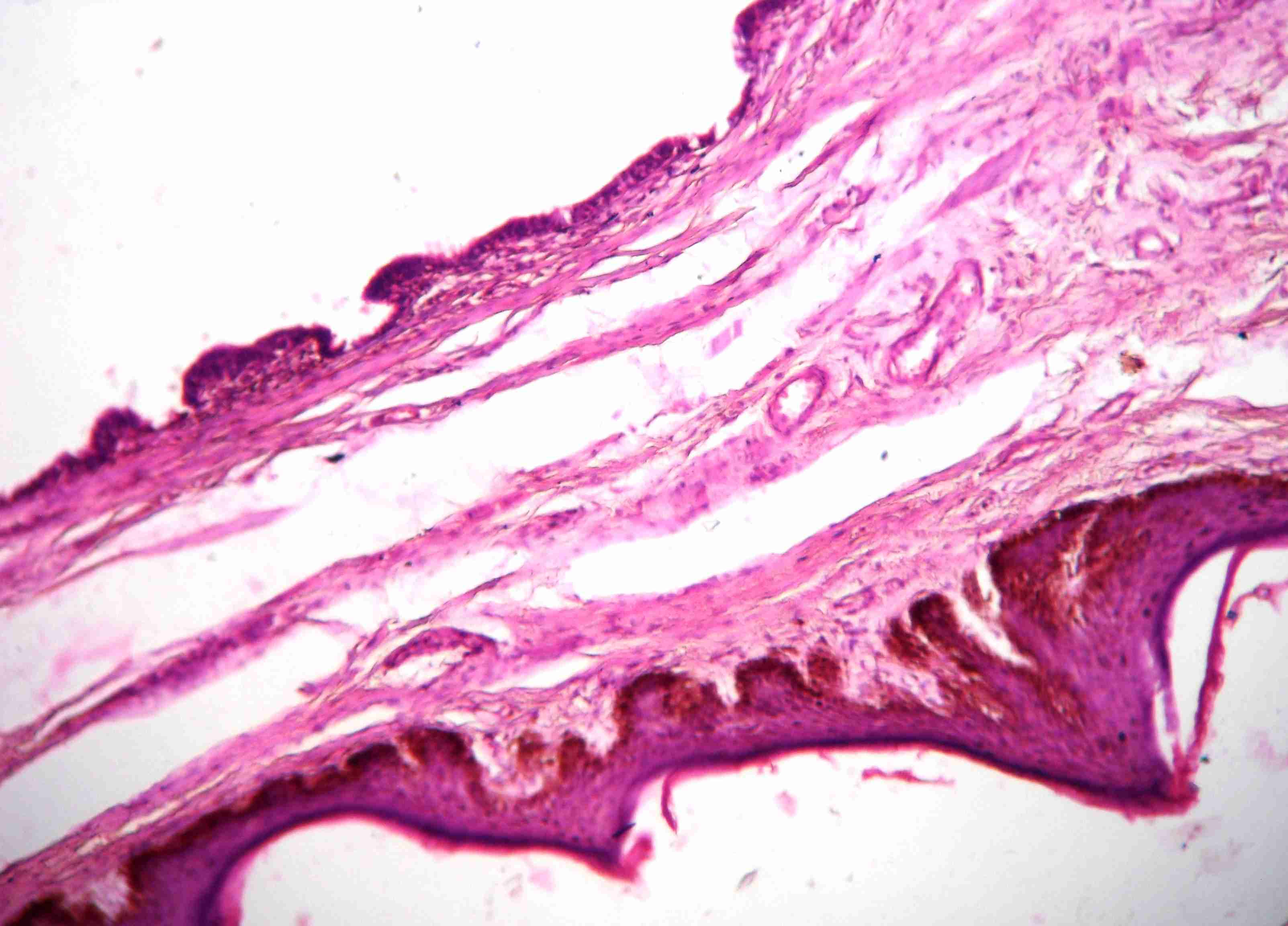
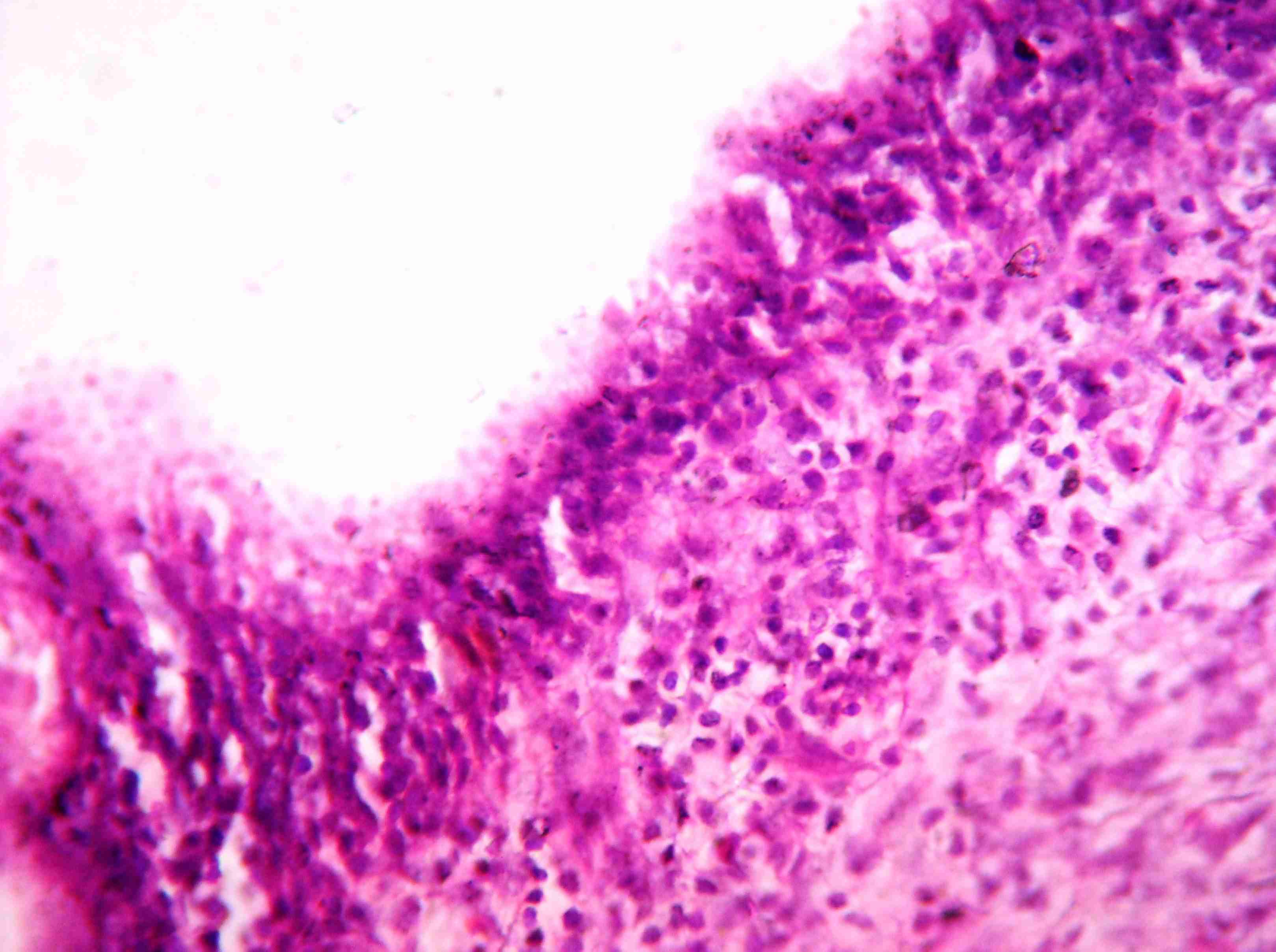
Grossly, the specimen measured 2 x 2 x 1.5 cm, it was soft to spongy in consistency and it was covered with skin at one surface. The cut section showed an irregular cyst which had collapsed and its inner surface was smooth. Multiple sections were taken randomly and their histopathological examinations revealed skin which was covered by cystic lesions [Table/Fig-2], with the subcutaneous tissue showing a fibro muscular stromal connective tissue and sparse aggregates of chronic inflammatory cell infiltrates. The cyst showed variable lining, with the stratified cuboidal to flat to the transitional type of epithelium. The focal areas also revealed cilia over the stratified cuboidal epithelium [Table/Fig-3]. A focal area also showed an apocrine snouting over the stratified cuboidal lining, with dense lymphocyte and plasma cell infiltrates in the sub-epithelial tissue [Table/Fig-4]. Considering the site and the histological features, a diagnosis of a median raphe cyst of the prepucial skin of the penis was issued.
Histopathology showing a cystic lesion covered with skin and areas of sub-cutaneous tissue showing fibromuscular stromal connective tissue. Cyst lining varied from areas to area (H&E, 4X)
Cyst lined with stratified cuboidal to flat to transitional type of epithelium with focal areas showing fine cilia (H&E, 10X)
A focal area showing apocrine snouting over the stratified cuboidal lining with dense lymphocyte and plasma cell infiltrate in the sub-epithelial tissue (H&E, 40X)
Discussion
Median raphe cysts (MRCs) are uncommon benign congenital lesions that can develop at any site along the midline of the ventral side of the male genital area, from the urethral meatus to the anus and the perineum (i.e.) along the median raphe of the male external genitalia [2].
The pathogenesis of this disease has not been well understood by the physicians. This is reflected in various theories which have been put forth for the development of this median raphe cyst, which are given below. The urethra forms as a result of the fusion of the urethral folds and the envelopment of the urethral groove during development. The first theory states that, ‘tissue trapping’ could occur at this time or at a later stage, either due to a defective fusion of the urethral folds or an anomalous outgrowth of the epithelium, which becomes sequestrated and independent after the primary closure of the median raphe [1–3]. Another theory proposes that the median raphe cysts could also be caused by the anomalous developmental rest of the periurethral glands of Littre [4]. This theory explains the presence of intraepithelial mucus cells and glandular structures in some cases. Some authors suggested that it may develop from the blockage of the paraurethral ducts [5].
According to the first theory, depending on the nature of the tissue which is trapped, the lining of the cyst may vary [2]. Four different types have been recognised so for. They are (1) pseudo stratified columnar epithelium (if the proximal urethral cells are trapped), (2) squamous cell epithelium (if the distal urethral cells are trapped), (3) glandular epithelium (if the periurethral glands are trapped) and (4) the mixed type [6]. Some authors says that the mixed type is the second most common type [6], and others says that itis the least common variety [7]. Ciliated cells in the median raphe cysts are a rare finding, with only five cases having been reported in the English literature. The pathogenesis is probably a metaplastic change which is secondary to a local irritation [8]. Our case belonged to the mixed type epithelium group, as it contained all the three elements, along with the ciliated cells.
In the earlier studies, some cases were reported under varied terms which included ‘mucoid cysts’, ‘genitoperineal cysts’, ‘parameatal cysts’, ‘hydrocystomas’, ‘apocrine cystadenomas’ [1] and ‘urethroid cysts’ [9]. If the luminal cells presented with a decapitation secretion, then the case was interpreted as an apocrine cystadenoma or a hydrocystoma.
In most of the patients, the cysts, which are asymptomatic or unrecognised during childhood, may progress slowly and become symptomatic during adolescence or adulthood [6]. Only one case of a spontaneous onset after an intense sexual intercourse has been documented [10]. Most of the cases of MRCs are asymptomatic because of the proximal locations of the cysts in the genitalia and their small sizes (usually less than 2 cm). The more distal the location of the cysts, the bigger the size of the cysts, greater will be the manifestation of the symptoms, such as pain (may be due to infection or trauma), difficulty during micturition, haematuria, haematospermia and difficulty in having sexual intercourse [6, 10]. Our patient who had a prepucial cyst approached the surgeon with the complaint of a difficulty in having sexual intercourse and for cosmetic reasons.
The most common location of such cysts is the penile shaft and the parameatal position. They have been rarely reported in the glans penis and the scrotum. Very rarely, prepucial median raphe cysts have been reported [6]. Although they are referred to as ‘median raphe cysts’, they can also present as cordlike or canaliform indurations on the median raphe, which are very rare [11]. The clinical differential diagnosis that should be kept in mind are glomus tumour, dermoid cyst, pilonidal cyst, epidermal inclusion cyst, urethral diverticulum, and steatocystoma [2].
Treatment should be considered for the symptomatic lesions and for cosmetic purposes. The treatment options include a wide local excision and aspiration, if the patient is not willing to undergo surgery. The latter may be associated with recurrence [6]. Thus, a simple aspiration alone is not recommended as a treatment for the median raphe cysts. Further, marsupialisation or deroofing are performed in the cases of deeply located large cysts, which can result in gaping sinuses, which are cosmetically unsatisfactory, and these procedures should be avoided [5]. Usually, no surgical complications are reported, except a few, like a urethrocutaneous fistula formation [6]. So, a complete local excision is the preferred treatment of choice.
In the present case, the indications for the treatment were, a difficulty in having sexual intercourse and a cosmetic disfigurement.
[1]. Otsuka T, Ueda Y, Terauchi M, Kinoshita Y, ‘Median raphe (parameatal) cysts of the penis’ inThe Journal of Urology [Internet] June, 1998 159(6):1918-20.cited in 24 Mar, 2013 Available at: http://www.ncbi.nlm.nih.gov/pubmed/9598487 [Google Scholar]
[2]. Nagore E, Sanchez-Motilla JM, Febrer MI, Aliaga A, Median raphe cysts of the penis: a report of five casesPediatric Dermatology [Internet]15(3):191-3.Available from: http://www.ncbi.nlm.nih.gov/pubmed/9655313 cited 24 Mar, 2013 [Google Scholar]
[3]. Krauel L, Tarrado X, Garcia-Aparicio L, Lerena J, Sunol M, Rodo J, Median raphe cysts of the perineum in childrenUrology [Internet] May, 2008 71(5):830-1.Available from: http://www.ncbi.nlm.nih.gov/pubmed/18313117 cited in 24 Mar, 2013 [Google Scholar]
[4]. Dini M, Baroni G, Colafranceschi M, Median raphe cyst of the penis: a report of two cases with immunohistochemical investigationThe American Journal of Dermatopathology [Internet] Aug, 2001 23(4):320-4.cited in 21 Mar 2013 Available from: http://www.ncbi.nlm.nih.gov/pubmed/11481524 [Google Scholar]
[5]. Shiraki IW, Parametal cysts of the glans penis: a report of 9 casesThe Journal of Urology [Internet] Oct, 1975 114(4):544-8.cited in 24 Mar, 2013 Available from: http://www.ncbi.nlm.nih.gov/pubmed/1235377 [Google Scholar]
[6]. Shao I-H, Chen T-D, Shao H-T, Chen H-W, Male median raphe cysts: serial retrospective analysis and histopathological classificationDiagnostic Pathology [Internet] Jan 2012 7:121cited in 19 Mar 2013 Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3487840&tool=pmcentrez&rendertype=abstract [Google Scholar]
[7]. Singh S, Baboo ML, Pathak IC, Cystic lymphangioma in children: report of 32 cases including lesions atrrare sitesSurgery [Internet] Jun, 1971 69(6):947-51.cited in 17 Mar, 2013 Available from: http://www.ncbi.nlm.nih.gov/pubmed/5578458 [Google Scholar]
[8]. Koga K, Yoshida Y, Koga M, Takeshita M, Nakayama J, Median raphe cyst with ciliated cells of the penisActa Dermato-Venereologica [Internet] Jan, 2007 87(6):542-3.cited in 19 Mar, 2013 Available from: http://www.ncbi.nlm.nih.gov/pubmed/17989897 [Google Scholar]
[9]. Paslin D, Urethroid cystArchives of Dermatology [Internet] Jan, 1983 119(1):89-90.cited in 24 Mar, 2013 Available from: http://www.ncbi.nlm.nih.gov/pubmed/6849573 [Google Scholar]
[10]. Giannakopoulos S, Makris NE, Kalaitzis C, Papatsoris AG, Pantazis T, Touloupidis S, Two unusual cases of median raphe penile cystsEuropean Journal of Dermatology: EJD [Internet]17(4):342-3.cited in 19 Mar, 2013, Available from: http://www.ncbi.nlm.nih.gov/pubmed/17540650 [Google Scholar]
[11]. Verma SB, Canal-like median raphe cysts: an unusual presentation of an unusual conditionClinical and Experimental Dermatology [Internet] Dec, 2009 34(8):e857-8.cited in 24 Mar, 2013 Available from: http://www.ncbi.nlm.nih.gov/pubmed/19817756 [Google Scholar]