Colletotrichum keratitis: A Rare but Definite Clinical Entity
Shanmuga Vadivoo Natarajan1, N. Sasi Rekha2, Rewa D. Sharda3, Niranjana Mahalingam4
1 Assistant Professor, Department of Microbiology, Annapoorana Medical College & Hospital, Salem, Tamil Nadu, India.
2 Senior Consultant & HOD, Department of Ophthalmology, Sri Sathya Sai Institute of Higher Medical Sciences (SSSIHMS-PG), Puttaparthy, Andra Pradesh, India.
3 Technical Assistant, Department of Microbiology, Sri Sathya Sai Institute of Higher Medical Sciences (SSSIHMS-PG), Puttaparthy, Andra Pradesh, India.
4 Technician, Department of Microbiology, Sri Sathya Sai Institute of Higher Medical Sciences (SSSIHMS-PG), Puttaparthy, Andra Pradesh, India.
Name, Address, E-Mail Id of The Corresponding Author: Dr Shanmuga Vadivoo Natarajan, Assistant Professor, Department of Microbiology, Annapoorana Medical College & Hospital, Periyaseeragapaadi, Salem-636 308, Tamil Nadu, India.
Phone: 07598890927
E-mail: shanmugavadivoon@gmail.com
Colletotrichum spp. is an emerging pathogen which causes a variety of human infections. Only a few cases of Colletotrichum keratitis have been reported from India. We are reporting three cases of keratitis which were caused by three different species of Colletotrichum. Two of the three patients had a history of trauma and of a previous treatment with topical antibiotics. A direct microscopic examination of the corneas of all the three patients revealed fungal elements and Colletotrichum spp. grew in the culture. Two patients responded to topical anti - fungal therapy and the ulcer regressed, while the third patient failed to respond .The third patient was referred to a higher specialty centre for Keratoplasty.
Colletotrichum keratitis, Case reports, India
Introduction
Mycotic keratitis has emerged to be a major ophthalmic problem and it is being increasingly reported worldwide. Fusarium is the most commonly reported aetiology, and Colletotrichum spp is now an emerging fungal pathogen which causes keratitis. About twenty such reports of the Colletotrichum infection have been recorded in the medical literature and only a few have been recorded from India. Seven cases were reported by Kaliamurthy et al., [1] one report was made by Joseph et al., [2], one was made in 2005 by Menderitta et al., [3] and another one was made in 2010 [4] by Prakash et al. We are reporting three cases of fungal keratitis which were caused by Colletotrichum spp, which emphasized the significance of an accurate identification and an appropriate initiation of the treatment for a specified period, which helped in the resolution of the keratitis.
Case -1
A 21-years old male attended the OPD with a history of dust falling in his left eye, a month earlier. He had the complaints of pain and watering in both the eyes and he had used topical antibiotics (names not known). On slit lamp examination, the left eye showed a central corneal ulcer with a feathery irregular margin. Stromal infiltration and vascularisation were not seen. The anterior chamber had a thick organised hypopyon. The initial visual acuity of his affected eye was 3/60. A corneal scraping of the ulcer was sent for microbiological investigations. The patient was initiated with oral ciprofloxacin 500 mg BD for a week and also other symptomatic drugs like oral Diamox (250 mg Qid) and 5% sodium chloride eye drops Qid were given. The topical prescription of Natamycin (5%) and ciprofloxacin (0.3%) eye drops was made when the positive direct microscopic report was received. The topical application was prescribed fourth hourly and it was reviewed every day for 10 days. Colletotricum dematium was isolated from this patient. The patient did not respond to the treatment because the ulcer was still persisting, with no improvement in the vision. The patient was referred to a specialty centre for a Total Penetrating Keratoplasty.
Case -2
This was a 45-year old female with a history of an injury which was caused by stone pieces on the right eye, one week earlier, and she had complaints of pain and watering in both the eyes. The patient was treated with topical antibiotics elsewhere, the names of which are not known. On slit lamp examination, it was seen that there was a small central corneal ulcer with 2mm hypopyon of the right eye. The initial visual acuity of her affected eye was 6/60. A corneal scraping of the ulcer was sent for microbiological investigations. Colletotrichum crassipes was isolated from this patient. The patient was initiated with symptomatic treatment and oral antibiotics, as has been mentioned for Case-1. A topical application with Natamycin (5%) and ciprofloxacin (0.3%) eye drops fourth hourly also was prescribed for two weeks. When the patient was examined at the end of two weeks, it was seen that the ulcer had started to heal, but the patient’s vision did not improve. The patient was advised to continue the same treatment for another two weeks. The patient’s vision improved to a 6/21 visual acuity and the ulcer had healed by about 50%. The topical application of both the eye drops was tapered down to eighth hourly for another three weeks. When the patient was examined three weeks later, there was complete resolution of the keratitis, with an approximate final visual acuity of 6/12.
Case -3
A 45-years old female with no history of trauma, came with the complaints of pain and watering in both the eyes since 10 days. She had not received any treatment earlier. On slit lamp examination, it was seen that there was a central corneal ulcer, which was seen with the Hypopyon. The initial visual acuity of the affected right eye was 6/18. Colletotrichum coccodes was isolated from this patient. The corneal ulcer started to regress with the disappearance of the hypopyon upon treatment with Natamycin and Ciprofloxacin eye drops fourth hourly, for a week. The visual acuity improved to 6/12. The patient was advised to continue the Natamycin and Ciprofloxacin eye drops for another 15 days. She failed to present herself for further follow up.
Microbiological Investigation
Corneal scrapings from these three patients were submitted for a routine direct microscopic examination and for the culture of bacteria and fungi. The corneal scrapings were examined in 10% KOH, (Himedia laboratories-Mumbai-India), Calcoflour white mount (Prepared in – house with reagents – Evans blue and Fluorescent brightener – from SIGMA chemicals co St. louis – USA), Lactophenol Cotton Blue (LCB) (Himedia laboratories – Mumbai – India) mount and on Gram staining (Himedia laboratories-Mumbai-India). The scrapings were also inoculated onto sheep blood agar (Readymade media from Delta biological – Bangalore – India), chocolate agar (Readymade media Delta biological, Bangalore, India), and Sabouraud’s dextrose agar (Prepared with Dehydrated media from Himedia laboratories – Mumbai, India). The growth of the same fungus on two or more media (or) its growth in at least one medium, with direct microscopy revealing the presence of fungal hyphae in the smear, was considered as indicative of a diagnosis of mycotic keratitis. [Table/Fig-1] gives the results of the microbiological work up of all the three patients.
Results of Microbiological investigation: *LCB mount, 10%KOH mount Calcoflour white mount and grams stain **Sheep blood agar,Chocolate agar andSabourauds dextrose agar (SDA) ***This species of colletotrichum was identified at Department of Microbiology, institute of Ophthalmology, Joseph eye hospital, Trichirapally, Tamilnadu. *****These two species were identified on site based on microscopic morphology following slide culture technic [5]
| Direct Microscopy* | Culture Growth Description** | Microscopic description of culture growth | Fungus Identified as |
|---|
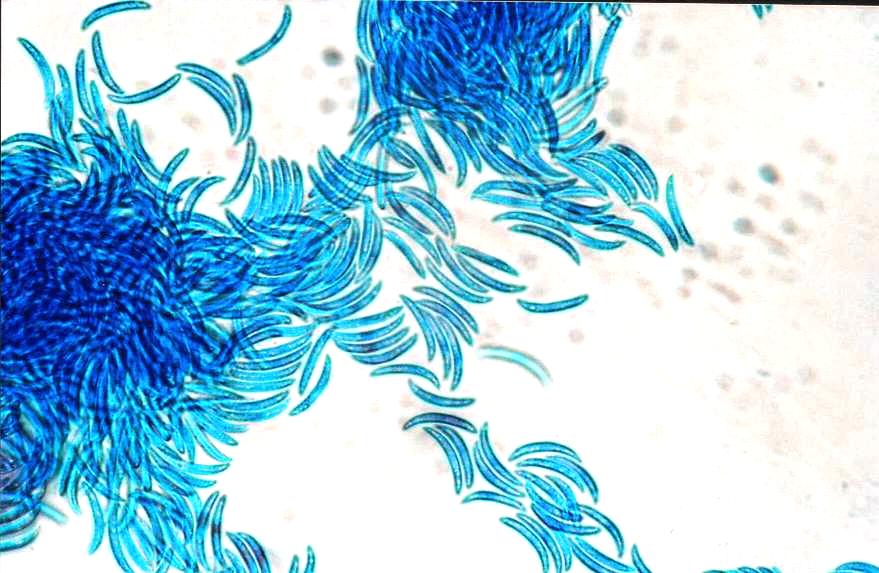
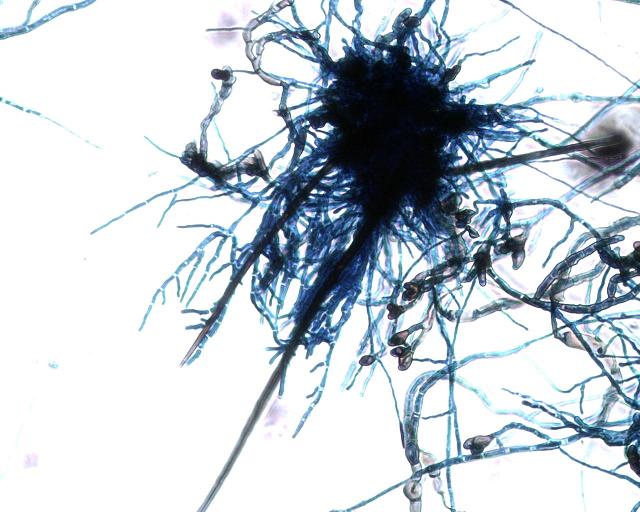
| Case-1 | Branching septate fungal elements seen on all four microscopic methods. | Three culture media used showed a rapidly growing white cottony fungus within 48 hours, which later on turned into mouse gray color colonies [Table/Fig-1]. Reverse of SDA had black color pigmentation [Table/Fig-2]. | LCB mounts of 48 hours old slide culture mounts showed) Many branching, septate hyaline & phaeoid fungal filaments. Many sickle shaped macro conidia without septation. [Table/Fig-3A]. Many pear shaped appressorias which had entire (smooth) margins [Table/Fig-3B]. Lacto phenol blue mount 10 days old of slide culture show the above two findings plus Brown color setae. [Table/Fig-3C & 3D]. | Colletotricum dematium*** |
| Case-2 | Branching septate fungal elements seen on all four microscopic methods. | Three culture media used showed a rapidly growing white cottony fungus within 48 hours, which later on turned into mouse gray color colonies. Reverse of SDA had black color pigmentation. | LCB mounts of 48 hour old slide culture mounts showed. Many branching, septate hyaline & phaeoid fungal filaments. Many cylindrical shaped macroconidia without septation [Table/Fig-4A, 4B, & Fig-4C]. Many brown color appressorias which were crenated or deeply lobed [Table/Fig-4D, 4E & 4C]. Absence of sclerotia and setae. | Colletotrichum crassipes**** |
| Case-3 | Branching septate fungal elements seen on all four microscopic methods. | Three culture media used showed a rapidly growing white cottony fungus within 48 hours, which later on turned into mouse gray color colonies. Reverse of SDA had black color pigmentation. | LCB mounts of 48 hour old slide culture mounts showed. Many branching ,septate hyaline & phaeoid fungal filaments. Many cylindrical shaped macroconidia without septation [Table/Fig-5A & 5B]. Many brown color appressorias which had entire margins [Table/Fig-5A & 5B]. Absence of sclerotia and setae in 10 day old culture. | Colletotrichum coccodes**** |
Mousy Gray to black colored cottony colonies of Colletotrichum spp. after 72 hrs on Sabouraudes Dextrose Agar plate.

Diffuse black pigmentation seen on the reverse side of SDA plate having Colletotrichum growth.

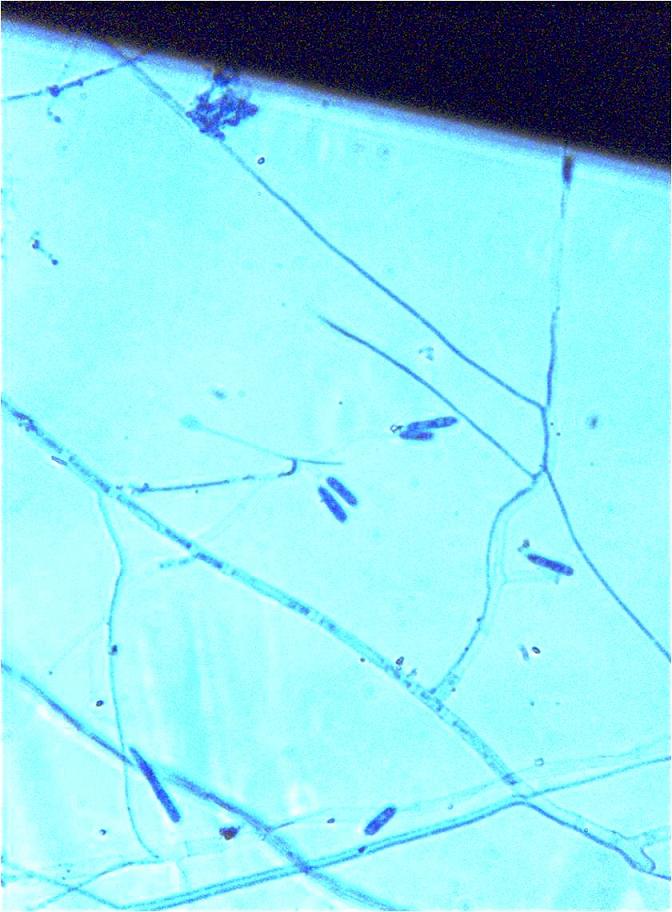
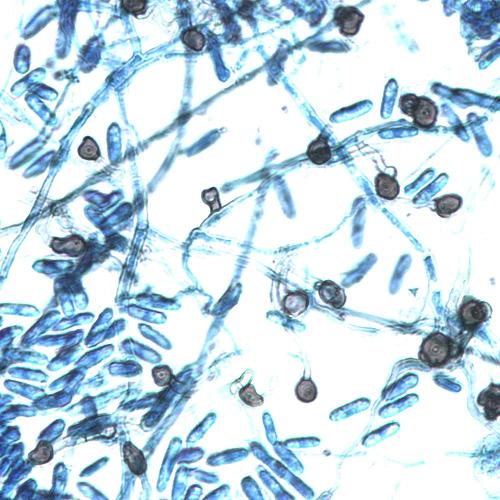
x400 view of slide culture mounts of Colletotrichum dematium showing Sickle shaped macro conidia without any septation
x 400 view of slide culture mounts of Colletotrichum dematium showing many brown color pear shaped appressorias with smooth margins

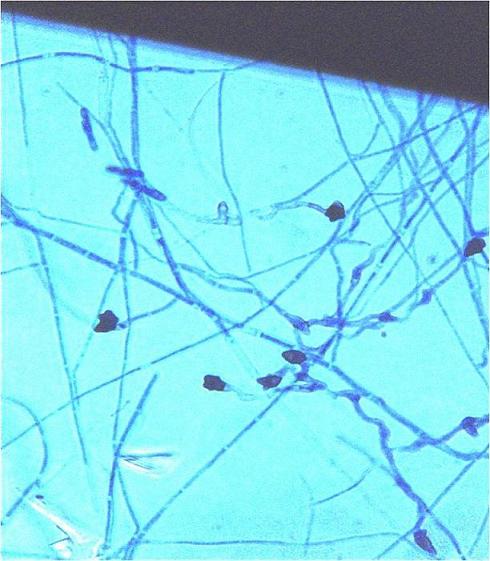
x200 view of slide culture mounts of Colletotrichum dematium showing sclerotia with brown color setae
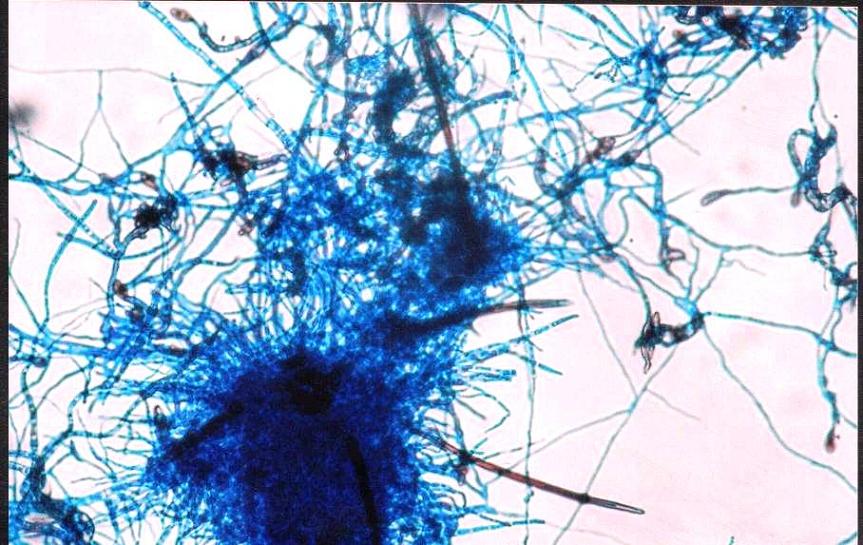
x 200 view of slide culture mounts of Colletotrichum dematium showing sclerotia with brown color setae. Pear shaped appressorias are also seen
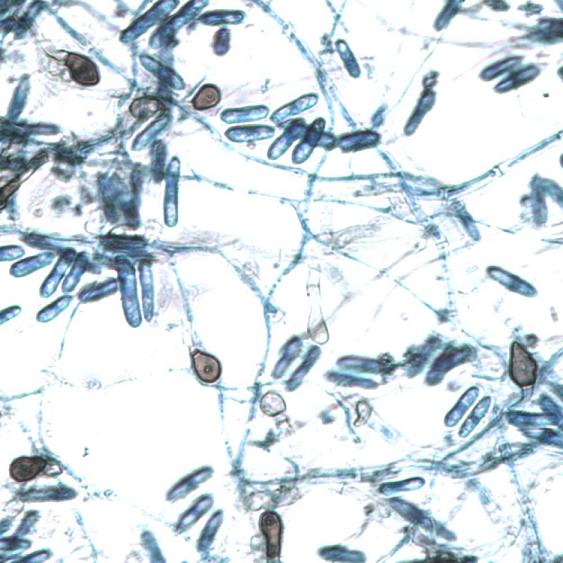
x 1000view of slide culture mounts of Colletotrichum crassipes showing cylindrical shaped macroconidia without septation
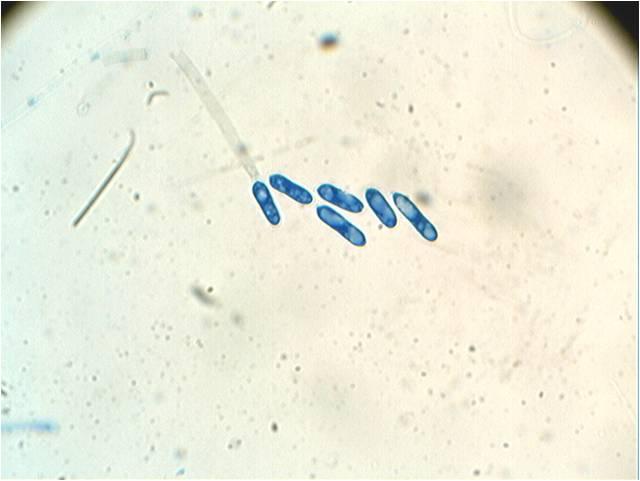
x 100 view of slide culture mounts of Colletotrichum crassipes showing cylindrical shaped macroconidia without septation
x 100 view of slide culture mounts of Colletotrichum crassipes showing many brown color crenated (or) deeply lobed appressorias and cylindrical shaped macroconodia
x 1000 view of slide culture mounts of Colletotrichum crassipes showing many brown color crenated (or) deeply lobed appressorias
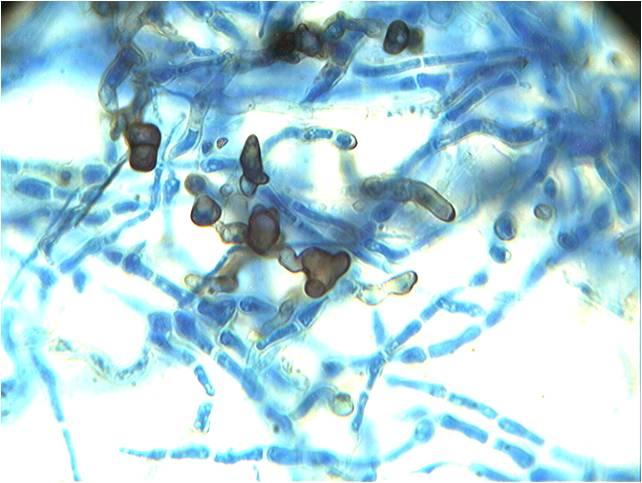
x 400 view of slide culture mounts of Colletotrichum crassipes showing many brown color crenated (or) deeply lobed appressorias
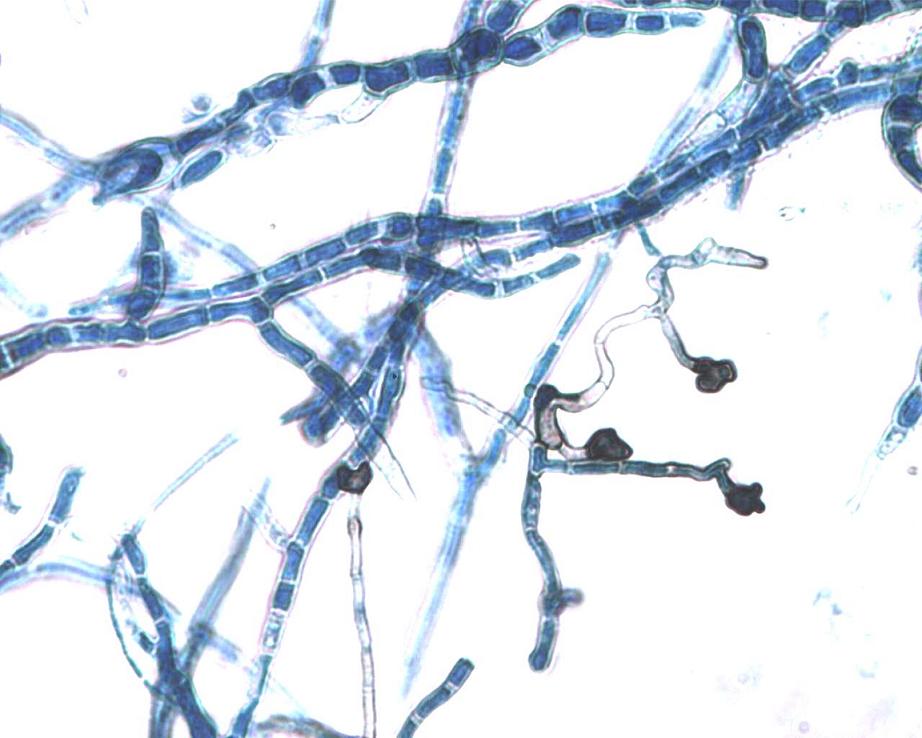
x 400 view of slide culture mounts of Colletotrichum coccodes showing many cylindrical shaped macroconodia without septation
x 400 view of slide culture mounts of Colletotrichum coccodes showing many brown color appresorias which had entire margins.
Discussion
The genus, Colletotrichum, one of the most important plant pathogens, has a worldwide distribution, but is found mainly in the tropical and the subtropical regions [6]. The five species of Colletotrichum which have been reported to be associated with human infections are Colletotrichumcoccodes, C. graminicola [4,7] C. crassipes [8], C.dematium, and C.gloeosporioides [9,10]. The predominant type of infection is keratitis, following a traumatic implantation [9,10], but subcutaneous and systemic infections among the immunosuppressed patients have also been reported recently.
A Pubmed search and a literature search revealed eight cases of Colletotrichum keratitis which were reported from south India [1,2] and two cases which were reported from other parts of India [3,4]. The reports from other parts of the world [7,9,10] showed eye and subcutaneous infections also.
The key morphological features which identify the genus are its acervular conidiomata, often with setae (which are dark-pigmented, unbranched, thick-walled, sterile hyphae which are usually pointed at the tip), and the presence of appressoria (thick-walled swellings at the end of a hypha or a germ tube, which are useful for attaching the fungus to the host surface before the penetration of the tissue) [5]. The falcate (or) cylindrical conidia can be misidentified as Fusarium spp. One has to carefully look for the presence or absence of the septation within the conidia and the presence or absence of the appressorias, to distinguish the Colletotrichum spp. from the Fusarium spp.
Two of our patients had sustained antecedent ocular trauma, which was the probable cause of the keratitis, which was in accordance with the literature and both of them had received prior antibacterial therapy. The third patient did not have any previous history of a trauma or treatment. There were no obvious risk factors like hypertension or diabetes in all the three patients. The bacterial cultures were negative for all the three clinical samples. An in vitro anti – fungal susceptibility testing could not be performed for the three isolates of the Colletotrichum spp.
Literature evidence has indicated that an early accurate identifi-cation with an immediate initiation of the appropriate anti – fungal therapy and a continued treatment for a specified period, helps in resolving Colletotrichum keratitis [1]. Two of our patients had a successful treatment out- come following an appropriate and an early initiation of the anti – fungal therapy after making a correct diagnosis. One patient had complete resolution of the keratitis with appreciable visual recovery and the other patient had started to show a better clinical response, but a further assessment was not possible, because the patient did not return for follow up. The unsuccessful treatment outcome of the third patient may possibly be due to the extensive damage which had been caused to his cornea due to the fungal aetiology.
A meticulous microbiological examination is essential for the identification of the Colletotrichum spp., as this will help in the complete resolution of the corneal ulcer after an early initiation of the appropriate anti – fungal therapy.
[1]. Kaliamurthy J, Kalavathy CM, Ramalingam MD, Prasanth DA, Jesudasan CA, Keratitis due to a Coelomycetous Fungus: Case Reports and Review of the LiteratureCornea 2004 23:3-12. [Google Scholar]
[2]. Joseph J, Fernandez M, Sharma S, Colletotrichum dematium KeratitisJ Postgrad Med 2004 50:309-10. [Google Scholar]
[3]. Mendiratta DK, Thamke D, Shukla AK, Narang P, Keratitis due to Colletotrichum dematium – a case reportInd J Med Microbiol 2005 23:56-58. [Google Scholar]
[4]. Yegneswaran Prakash P, Pai Vijaya, Bairy Indira, Bhandary Sulatha, Colletotrichum graminicola keratitis. First case report from IndiaIndian J Ophthalmol 2010 58(5):415-17. [Google Scholar]
[5]. Cano J, Guarro J, Gené J, Molecular and Morphological Identification of Colletotrichum Species of Clinical InterestJ Clin Microbiol 2004 Jun 42(6):2450-54. [Google Scholar]
[6]. Bailey JA, Jegger MJ, Colletotrichum: biology, pathology and control 1992 Wallingford, United KingdomCAB International [Google Scholar]
[7]. De Hoog GS, Guarro J, Gene J, Figueras Atlas of clinical fungi: 1995 2nd edUtrecht, The NetherlandsCentraalbureau voor Schimmelcultures:306-10. [Google Scholar]
[8]. Castro Phaeohyphomycotic cyst caused by Colletotrichum crassipesJ Clin Microbiol 2001 Jun 39(6):2321-24. [Google Scholar]
[9]. Fernandez V, Dursun D, Miller D, Alfonso EC, Colletotrichum keratitisAm J Ophthalmol 2002 Sep 134(3):435-38. [Google Scholar]
[10]. Yamamoto N, Matsumoto T, Ishibashi Y, Fungal keratitis caused by Colletotrichum gloeosporioidesCornea 2001 Nov 20(8):902-03. [Google Scholar]