A Multivessel Umbilical Cord with a Single Umbilical Artery
Subrat Panda1, Vandana Jha2, Yookarin Khonglah3, Biswajit Dey4
1 Associate Professor, Department of Obstetrics and Gynaecology, NEIGRIHMS, Shillong, India.
2 Junior Resident, Department of Obstetrics and Gynaecology, NEIGRIHMS, Shillong, India.
3 Associate Professor, Department of Pathology, NEIGRIHMS, Shillong, India.
4 Junior Resident, Department of Pathology, NEIGRIHMS, Shillong, India.
Name, Address, E-Mail Id of The Corresponding Author: Dr Biswajit Dey, RMO Hostel, NEIGRIHMS, Mawdiangdiang 793018, Shillong, Meghalaya, India.
Phone: +919911310290
E-mail: drbish25@rediffmail.com
Umbilical cord abnormalities are known to be associated with congenital anomalies, chromosomal abnormalities and potential complications during pregnancy.
We are reporting a case of a multivessel umbilical cord which comprised two umbilical veins alongwith a single umbilical artery.
Multivessel umbilical cord, Single umbilical artery, Congenital anomalies
Introduction
The most common abnormality of the umbilical cord is a single umbilical artery, which occurs in 0.5% to 2.5% of the pregnancies [1]. A single umbilical artery has been associated with multiple congenital anomalies [2]. Another abnormality of the umbilical cord is a multivessel cord, which contains more than two arteries or more than one vein. A multivessel cord is rare and it also has been associated with congenital anomalies and conjoined twins [3]. Thus, most of these cases end up in perinatal and postnatal foetal loss. However, this rarely reported vascular pathology may not always be associated with congenital malformations, but such cases require a comprehensive antenatal workup, to permit a better perinatal outcome [4,5].
Case Report
A 37 years old female came to our antenatal clinic for a routine check up in her second pregnancy, at eight months of gestation, for the first time. She gave an uneventful history of the first and second trimester. She had a history of spontaneous abortion at three months of gestation, in her previous pregnancy.
Her vital parameters and general examination findings were normal. On obstetrical examination, her symphysio – fundal height was found to correspond to 28 weeks of gestation and thus a clinical diagnosis of an intra – uterine growth restriction was made. Her routine antenatal haemogram and urine tests were normal. Her obstetrical ultrasonography showed a single live intrauterine foetus of 31 weeks with intrauterine growth retardation and severe oligohydramnios, with an amniotic fluid index of 3.2 and the largest vertical pocket of less than 2 cm. Her anomaly scan was normal, except that it showed a single umbilical artery with a persistent right vein. Her TORCH screening was negative. An admission was advised in view of her of obstetrical risk factor, for further evaluation and management, which the patient refused.
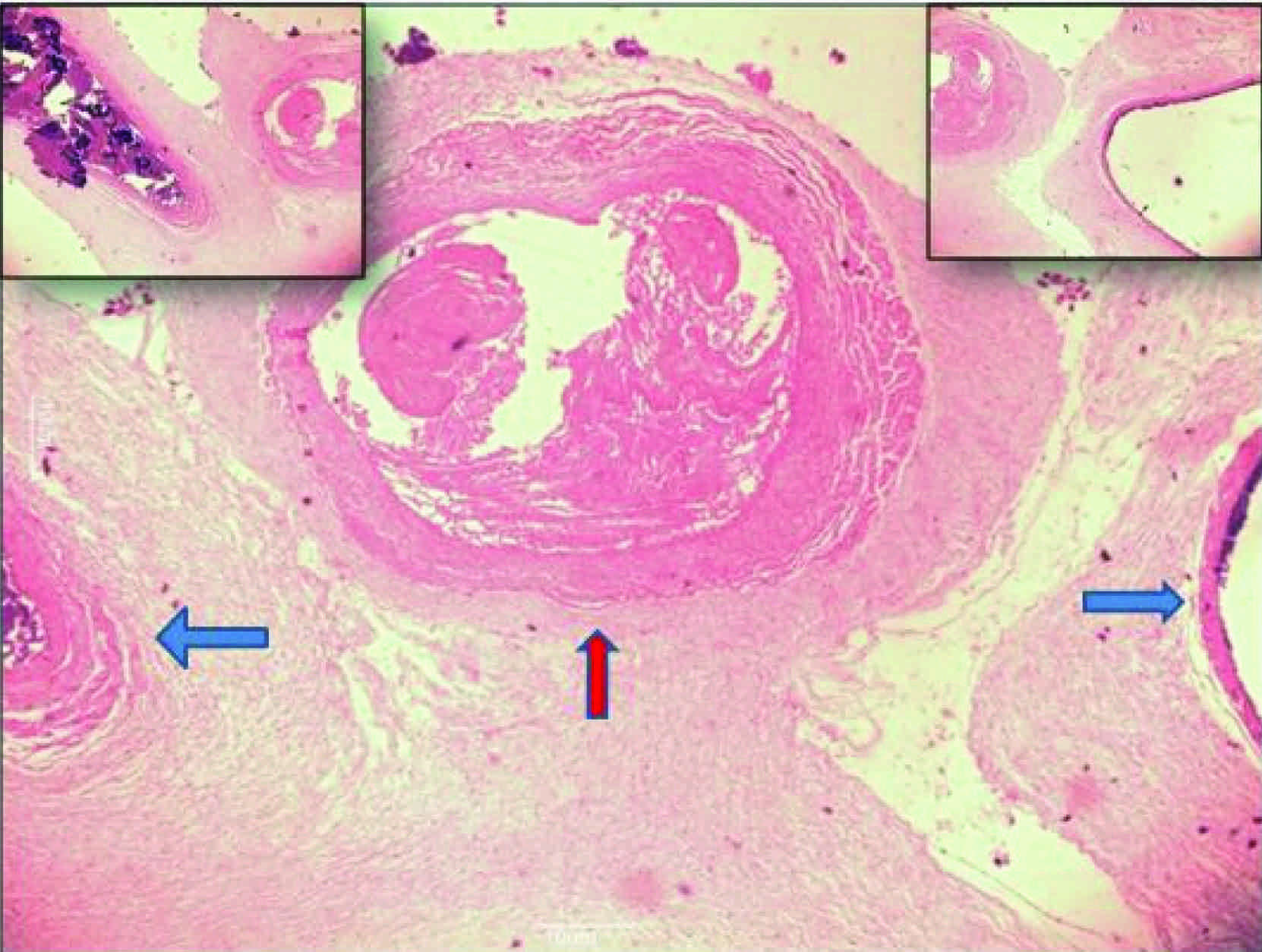
After two weeks, she again visited the antenatal clinic with loss of foetal movements for one day. On clinical and ultrasonographic examination, an intrauterine foetal demise was confirmed. Labour was induced with intra – vaginal misoprostol in view of the intrauterine foetal demise. A dead female baby which weighed 1.4 kg was delivered. No signs of maceration or no apparent congenital anomalies were seen. The placenta, alongwith the umbilical cord, was sent for a pathological examination. On histopathological examination, the umbilical cord showed a single umbilical artery and both the left and right persistent umbilical veins [Table/Fig-1]. The autopsy of the dead foetus was not done, as the patient refused the same due to religious reasons.
Haematoxylin and eosin stained section (10x magnification) of umbilical cord showing one umbilical artery (Red Arrow) and two umbilical veins (Blue Arrows). Insets show the umbilical veins on either side of the artery (4x magnification)
An umbilical cord contains two arteries and one vein. In the present case, the infant had one umbilical artery and two umbilical veins. A single umbilical artery is believed to be caused either due to the atrophy of a previously normal artery or due to agenesis of one of the umbilical arteries. The presence of two veins in the umbilical cord could be attributed to the persistence of both the normal left umbilical vein and the caudal part of the right umbilical vein.
A multi – vessel umbilical cord, as well as a single umbilical artery, are associated with a high incidence of congenital anomalies, which include cardiovascular abnormalities, gastrointestinal defects, oesophageal atresia, a variety of renal defects and multiple anomaly syndromes, and poor perinatal and post – natal outcomes [2,3]. Thus, a multivessel umbilical cord abnormality with a single umbilical artery detection in the antenatal period is a forewarning sign of the adverse perinatal outcome and it should prompt a comprehensive antenatal examination, to rule out other congenital anomalies.
[1]. Callen PW, Ultrasonography in Obstetrics and Gynecology 2000 4th edPhiladelphia, PennW.B. Saunders Company [Google Scholar]
[2]. Volpe G, Volpe P, Boscia FM, Volpe N, Buonadonna AL, Gentile M, ‘Isolated’ single umbilical artery: incidence, cytogenetic abnormalities, malformation and perinatal outcomeMinerva Ginecol 2005 57:189-98. [Google Scholar]
[3]. Painter D, Russell P, Four – vessel umbilical cord associated with multiple congenital anomaliesObstet Gynecol 1977 50:505-507. [Google Scholar]
[4]. Pérez-Cosio C, Sheiner E, Abramowicz J S, Four-vessel umbilical cord: not always a dire prognosisJ Ultrasound Med 2008 27:1389-1391. [Google Scholar]
[5]. Schimmel MS, Eidelman AI, Supernumerary umbilical vein resulting in a four-vessel umbilical cordAm J Perinatol 1998 15:299-301. [Google Scholar]