Introduction
Nocardia is a well known opportunistic pathogen. Recently, we isolated Nocardia from two patients, one who was admitted with breathlessness and the other who was suffering with lymphadenitis ( who was later found to be HIV positive).
Case History
Case I: A 70-years-old female patient was admitted with fever, breathlessness and left lower zone pneumonia, along with osteomalecia and hypertension. Though there was no complaint of cough, she had fever for a period of one month and a history of breathlessness for a period of 4 years. On chest examination, it was observed that her chest was bilaterally clear, No abnormalities were detected in the chest and the CVS. Her blood pressure was 100/60, her pulse rate was 72 per minute and her haemoglobin was 11.6. The total leucocyte count was 9200 and the erythrocyte sedimentation rate was 21.
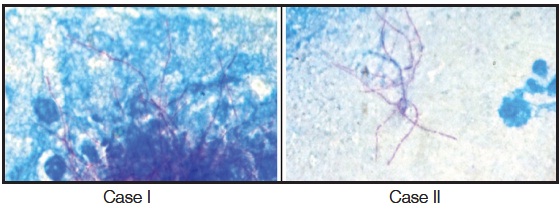
Her blood and sputum samples were sent to the microbiology laboratory for culture and microscopy. The blood culture was done in BHI broth, but no organism was isolated after 7 days of incubation. The sputum sample was stained by the Ziehl Neelsen Staining Method by using 20% sulphuric acid [Table/Fig-1]. Microscopy revealed pink coloured branching filaments. The staining procedure was repeated with 1% H2S04, which showed similar findings. Gram staining of the samples showed thin gram positive beaded and coccoid branching filaments, which were suggestive of Nocardia species. It also showed gram positive, thick, septate ,fungal hyphae with acute angle branching. The sputum sample was cultured on 5% sheep Blood agar, MacConkey’s agar, Nutrient agar and Sabouraud’s Dextrose Agar (SDA). The plates were incubated at 370C. One more plate of SDA was incubated at 250C. Golden yellow, circular and β haemolytic colonies were seen on blood agar after 24 hours of incubation, which were later identified as Staphylococcus aureus on the basis of gram staining and other confirmatory tests like catalase, coagulase and Mannitol fermentation. The antibiotic sensitivity testing of Staphylococcus aureus was done by the Kirby Bauer technique.
Nocardia seen under high power after ZN staining with 20% H2SO4
Further incubation of the blood agar plates at 37 degree Celsius showed white, rough, dry, irregularly folded, chalky colonies on the 4th day of incubation. The colonies showed the characteristic aerial hyphae, which indicated Nocardia. It was identified as the Nocardia asteroides complex, based on the gram staining and acid fast staining by using both 20% and 1% H2SO4 as decolourisers, Caesin hydrolysis, Xanthine hydrolysis, L – Tyrosine hydrolysis and the Antibiotic sensitivity profile which was assessed by using Tobramycin (Resistant), Erythromycin (Resistant) and Cefotaxime (Sensitive) [1].
The blood agar and the SDA plates also showed dry, cream coloured, circular colonies. Gram staining was done from both the SDA plates, and they showed septate hyphae. Lacto-phenol cotton blue mounts were made for the fungal growth. Based on the morphological details which were observed (the presence of arthroconidia and a negative urea hydrolysis), it was identified as Blastoschizomyces capitatus.
The patient was on an empirical treatment of levofloxacin (500 mg OD), and injection Acuclave (amoxyclav+ Potassium clavulinic acid) and she responded well to the drugs. Her condition improved and the symptom of breathlessness was reduced significantly at the time of her discharge.
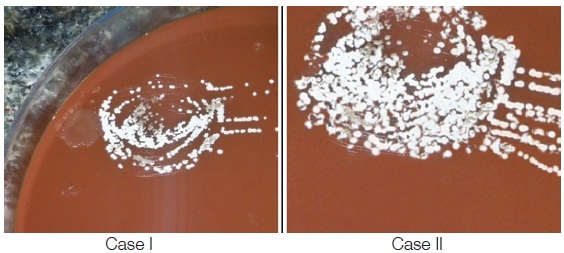
Case II: A 36-years-old male patient was admitted with the complaints of high fever, lymphadenitis, pain in the neck, swelling and pus discharge from the right supra-clavicular region. He was given an empirical treatment of Augmentin (625 mg). The pus was collected by needle aspiration and it was sent to the Microbiology laboratory for microscopy and culture sensitivity studies. It was subjected to gram staining and Ziehl Neelsen Staining (with 20% H2SO4). Both the slides revealed the presence of Nocardia. The Ziehl Neelsen Staining was repeated with 1% H2SO4, which showed similar results. The pus was cultured on blood agar and nutrient agar. After 3 days of incubation at 37 degree Celsius, the characteristic grey, dry, chalky wrinkled colonies appeared on blood agar [Table/Fig-2]. The organism was identified as Nocardia brasiliensis on the basis of its ability to hydrolyze Caesin and L – Tyrosine as the sole sources of carbon [2]. By the disk diffusion test, the isolate was found to be sensitive to gentamicin and amikacin and to be resistant to ceftazidime, ciprofloxacin and ampicillin. Its resistance to ciprofloxacin confirmed that the organism was Nocardia brasiliensis [3]. The blood sample of the patient was also sent for serological tests and he was diagnosed as HIV-1 positive. The patient was referred to a higher centre for further confirmation of HIV infection.
Nocardia colonies on blood agar
Discussion
Nocardia is gram-positive, catalase-positive, rod-shaped and filamentous bacteria. It is non motile and non-capsulated. It is acid fast with beaded branching filaments. It belongs to the suborder, Corynebacterineae, of the phylum, Actinobacteria. It was first isolated in the year 1888. More than 50 species of Nocardia have been recognized till now, on the basis of their phenotypics and molecular characters. Among these, around 22 species have been identified as potential pathogens, the most common one being the N. asteroides complex (N. asteroides sensu strictu, N. farcinica, N. nova and N. abscessus). The other important pathogenic species are N. brasiliensis, N. africana, N. brevicatena complex, N. carnea, N. paucivorans, N. pseudobrasiliensis, N. transvalensis, etc [4].
Nocardia is found worldwide in soil that is rich with organic matter. it is present as normal oral flora in healthy gingiva as well as in the periodontal pockets. Most of the Nocardia infections are acquired through the respiratory route or through trauma. Pulmonary nocardiasis constitutes upto 70% of the total incidences of Nocardiosis and this is attributed to the fact that the organism can be easily aerosolised. A majority of these cases are attributed to the N. asteroides complex. N.brasiliensis is also an established but a relatively uncommon pulmonary pathogen [4]. [Table/Fig-3] represents the common Nocardial species which are associated with human infections.
Nocardia species associated with human infection [12] (Saubolle and Sussland,2003)
| Commonly associated | Nocardia asteroides complex Nocardia brasiliensis |
|---|
| infrequently associated | Nocardia otitisdiscaviarum |
| Nocardia pseudobrasiliensis |
| Rarely associated | Nocardia abscessus |
| Nocardia africana |
| Nocardia brevicatena complex |
| Nocardia carnea |
| Nocardia paucivorans |
| Nocardia transvalensis |
| Nocardia veterana |
The N.brasiliensis infection is more commonly seen in the patients who are associated with agriculture. Its direct inoculation may lead to infections in the skin and the subcutaneous tissues, which may later spread to the regional lymph nodes [4]. Disseminated infections are seen in many cases. The organism enters into the blood stream through the lungs and it then reaches into and infects other organs. The CNS, retina, kidneys, joints, bone, and the heart are the common sites of disseminated Nocardiosis.
The rate of incidence for the Nocardial infection in AIDS and in immuno compromised patients is well over 100% in comparison to that in the normal population [5].
The organism can be detected in clinical samples by gram staining and by the modified Ziehl Neelsen Staining Method by using 1% sulphuric acid. Many studies have shown that gram staining is a more reliable method of staining Nocardia [6]. A number of special media are available for the cultivation of Nocardia, like Buffered charcoal yeast extract agar with antibiotics, Sabouraud’s Dextrose Agar (SDA) with chloramphenicol, Thayer–Martin agar with antibiotics, etc. But Nocardia can grow readily on the routine laboratory media like brain heart infusion agar, SDA and blood agar. The colonies may appear within 48 hours to 3 weeks (generally 3 to 5 days) [5]. The growth is seen best at 370C to 450C and in the presence of CO2. The colonies are dry, raised and chalky white in colour, but they can also be yellowish or pinkish.
Identification of the species can be done on the basis of a battery of biochemical tests and the sensitivity profile towards certain antibiotics. [Table/Fig-4] shows the biochemical tests for the species identification. The organisms which are identified as belonging to the N. asteroides complex can be further differentiated on the basis of their antibiotic sensitivities. N. nova is sensitive to both cefotaxime and erythromycin, whereas N. farcinica is resistant to both. N. asteroides is sensitive to cefotaxime but it is resistant to erythromycin.
Major biochemical reaction of Nocardia species
| Casein hydrolysis | L-tyrosine hydrolysis | Xanthine hydrolysis | Galactose | Glycerol | Trehalose | Adonitol | Esculin |
|---|
| N. asteroides complex | - | - | - | - | + | - | - | - |
| N. brasiliensis | + | + | - | + | + | + | - | + |
| N. otitidiscaviarum | - | + | - | - | + | + | - | + |
| N. nova | - | - | - | - | - | - | - | - |
| N. brevicatena | - | - | - | - | - | - | - | + |
| N. transvalensis | - | - | - | + | + | + | + | - |
| N. pseudobrasiliensis | + | + | - | + | + | + | - | + |
| N. farcinica | - | - | - | - | + | - | - | + |
Trimethoprim-sulfamethoxazole is the drug of choice. The drugs like are minocycline, amikacin, imipenem, and linezolid are effective for the treatment of Nocardiosis. The other effective drugs are ciprofloxacin, amoxyclav, the extended-spectrum cephalosporins, azithromycin, etc [6].
Nocardia is an infrequent pathogen which is found in both healthy and immunocompromised individuals. Though pulmonary Nocardiosis is mostly seen in immunocompromised patients, its incidence in immunocompetent persons has also been reported [7]. We had isolated the Nocardia asteroides complex from an immunocompetent elderly female who was suffering from pulmonary Nocardiosis, which is the most common manifestation of the Nocardial infection [3]. Pulmonary Nocardiosis can be divided into 2 groups, i.e the patients who are on corticosteroid therapy (with a mortality rate of 80-100%) and the patients with underlying untreated disease (with a mortality rate of 15-20%). This particular patient was an otherwise healthy lady with the complaints of chronic breathlessness and she was also suffering from fever for the past one month. She responded well to the antibiotics which were administered to her as an empirical treatment. She was discharged after one week of admission. She also had a concomitant infection which was caused by Blastoschizomyces capitatus, which is a rare infection. In India, cases of Blastoschizomyces capitatus were reported earlier by Sreeja et al., [8]. Mostly, the symptoms may resemble those of tuberculosis and hence, a differential diagnosis is important. Moreover, it is important to appreciate that Nocardia takes more time to grow and to form visible colonies as compared to other bacteria (> 48 – 72 hours). Hence, a longer incubation is required before discarding the culture plates as negative, for the isolation and identification of Nocardia.
The second case was of Nocardia brasiliensis in a HIV positive patient with a swelling in the right supraclavicular region. The incidence of Nocardia brasiliensis is only 7 – 10% as compared to Nocardia asteroides, which is seen in 90% of the cases of the Nocardia infection. But when it comes to the cutaneous infections, the incidence rate of Nocardia brasiliensis is much higher than that of any other Nocardia species [9]. There are also some reported cases of Nocardia brasiliensis which had caused life threatening pulmonary infections.
The symptoms and the radiological findings of pulmonary Nocardiosis and tuberculosis are more or less similar. One of the most reliable and widely used techniques for the diagnosis of tuberculosis is the Ziehl Neelsen Staining with the use of 20% H2SO4 as a decolouriser. But in this test, most of the Nocardial infections go unreported, since Nocardia generally appears as acid fast only when it is decolorized with 1% H2SO4. Interestingly, in these two cases, both the Nocardial strains were acid fast against 20 % H2SO4. Earlier Rawat et al., in India had reported 20% acid fast Nocardia [10]. These findings indicated the need of a more detailed study on the staining character of the Nocardia species.
[1]. Sorrell TC, Iredel JR, Mitchell DH, Nocardia speciesIn: Principles and Practice of Infectious Diseases2006th edPhiladelphiaChurchill Livingstone:2637-45.Mandell GL, Bennett JE, Dolin R, editors [Google Scholar]
[2]. Koneman EW, Allen SD, Janda WM, Schreckenberger Winn WC Jr, The Aerobic Gram-Positive BacilliIn: Color Atlas and Textbook of Diagnostic Microbiology 1997 5th edPhiladelphiaLippincott:651-708. [Google Scholar]
[3]. Wallace RJ, Brown BA, Blacklock Z, Ulrich R, Jost K, Brown JM, New Nocardia taxon among isolates of Nocardia brasiliensis associated with invasive diseaseJ Clin Microbiol 1995 33:1528-33. [Google Scholar]
[4]. Vohra P, Sharma M, Yadav A, Chaudhary U, Nocardiosis: A review of clinico-microbiological featuresInt. J. Life Sc. Bt Pharm. Res 2013 2:20-29. [Google Scholar]
[5]. Ambrosioni J, Lew D, Garbino J, Nocardiosis: Updated Clinical ReviewInfection 2010 38(2):89-97. [Google Scholar]
[6]. Saubolle MA, Sussland D, Nocardiosis: Review of Clinical and Laboratory ExperienceJ. Clin. Microbiol 2003 41(10):4497-501. [Google Scholar]
[7]. Amatya R, Koirala R, Khanal B, Dhakal SS, Nocardia brasiliensis primary pulmonary Nocardiosis with subcutaneous involvement in an immunocompetent patientIndian J Med Microbiol 2011 29:68-70. [Google Scholar]
[8]. Sreeja S, Banashankari GS, Bhavana MV, Gayathri Devi DR, Blastoschizomyces capitatus pneumonia: A rare caseIndian J Pathol & Microbiol 2011 4:846-47. [Google Scholar]
[9]. Satterwhite TK, Wallace RJ Jr, Primary cutaneous NocardiosisJAMA 1979 242(4):333-36. [Google Scholar]
[10]. Rawat V, Umesh Thapliyal N, Punera DC, Primary pulmonary infection caused by 20% acid fast Nocardia brasiliensisIndian J Med Microbiol 2011 29:446-47. [Google Scholar]