Bilateral Aberrant Renal Arteries with Abnormal Left Renal Vein: A Case Report
N B S Parimala1
1 Assistant Professor, Department of Anatomy, Dr Pinnamaneni Siddhartha Institute of Medical Sciences & Research Foundation, Chinnaoutpalli, Gannavaram Mandal, Krishna District, AP – 521286 India.
Name, Address, E-Mail Id of The Corresponding Author: Dr N B S Parimala, Flat No.3, fourth floor, Alekhya apartments, Siddhartha nagar, Vijayawada, Krishna District, AP – 521286, India.
Phone: 9440791896 Email: nbsparimala@gmail.com
Renal arteries are a pair of lateral branches which arise from abdominal aorta, just below the origin of the superior mesenteric artery (sma), at L2 level. The right one is longer, on account of position of aorta and left is a little higher in its origin. Variations in renal arteries are highly common and such variations may differ in number, mode of origin, branching, course and termination.
Extra renal arteries (ERA) are broadly divided into two types- The aberrant (polar) ones are those which supply the kidney (poles) without passing through hilum, whereas the accessory (hilar) ones are those which supply the kidney after passing through hilum. The renal veins are of large size, which are located anterior to arteries and they open into inferior vena cava at right angles. The left is thrice in length than right one and it passes in front of abdominal aorta to join inferior vena cava (IVC). In view of constantly increasing renal transplantations and kidney retrieval surgeries, the variations in renal vasculature are valuable.
Anomalies of renal veins are rarely encountered. Abnormal renal vessels are of interest to the medical and surgical personnel, because of the wide spectrum of diseases which are associated with kidney, like hydronephrosis, left renal vein hypertension, retro peritoneal tumours and surgeries, particularly renal transplantations.
Renal artery, Left renal vein
Case Report
During a routine dissection which was held for Ist M.BB.S students (batch 2011-2012), in an elderly male cadaver which was aged 60 years, bilateral aberrant renal arteries and a retro aortic left renal vein were found.
It was observed that left kidney was supplied by two renal arteries which took their origin from abdominal aorta at L2 level, one below the other. The first one was an aberrant bipolar artery and it bifurcated into two branches, just before reaching upper pole of left kidney, to supply both upper and lower poles. The lower polar branch from above said artery superficially crossed the left renal vein to reach the lower pole. The second left renal artery took origin just below the 1st branch and it was a normal hilar branch [Table/Fig-1].
Bilateral aberrant renal arteries and retro aortic left renal vein
1. Abdominal aorta
2. Upper Left renal artery – Aberrant bipolar artery
3. Lower Left renal artery – hilar
4. Upper Right renal artery – hilar
5. Lower Right renal artery – Aberrant lower polar artery
6. Left renal vein with retro aortic course
7. Right renal vein
8. Inferior vena cava
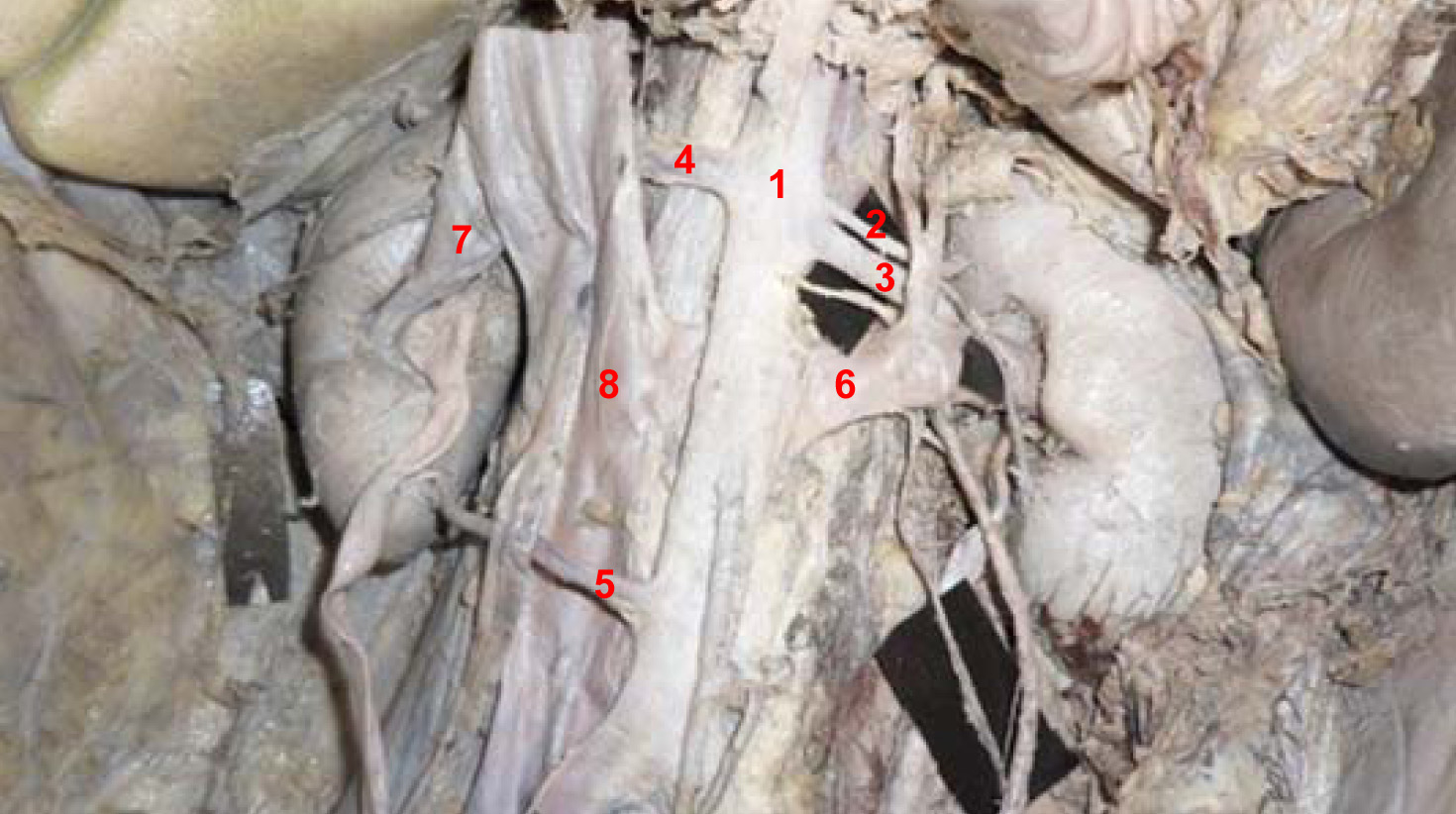
On the right side also, two renal arteries with different levels of origin from aorta were seen; the first one was a hilar branch at the L2 level (below sma origin) with an early division behind IVC into two branches, after giving a branch to right supra renal gland which passed obliquely downwards anterior and posterior to right ureter. The anterior branch also gave slender branches to upper pole and peritoneum of that side. The second right renal artery was a polar branch at L3 level (below ima origin) and it had a retroureteric course for reaching lower pole.
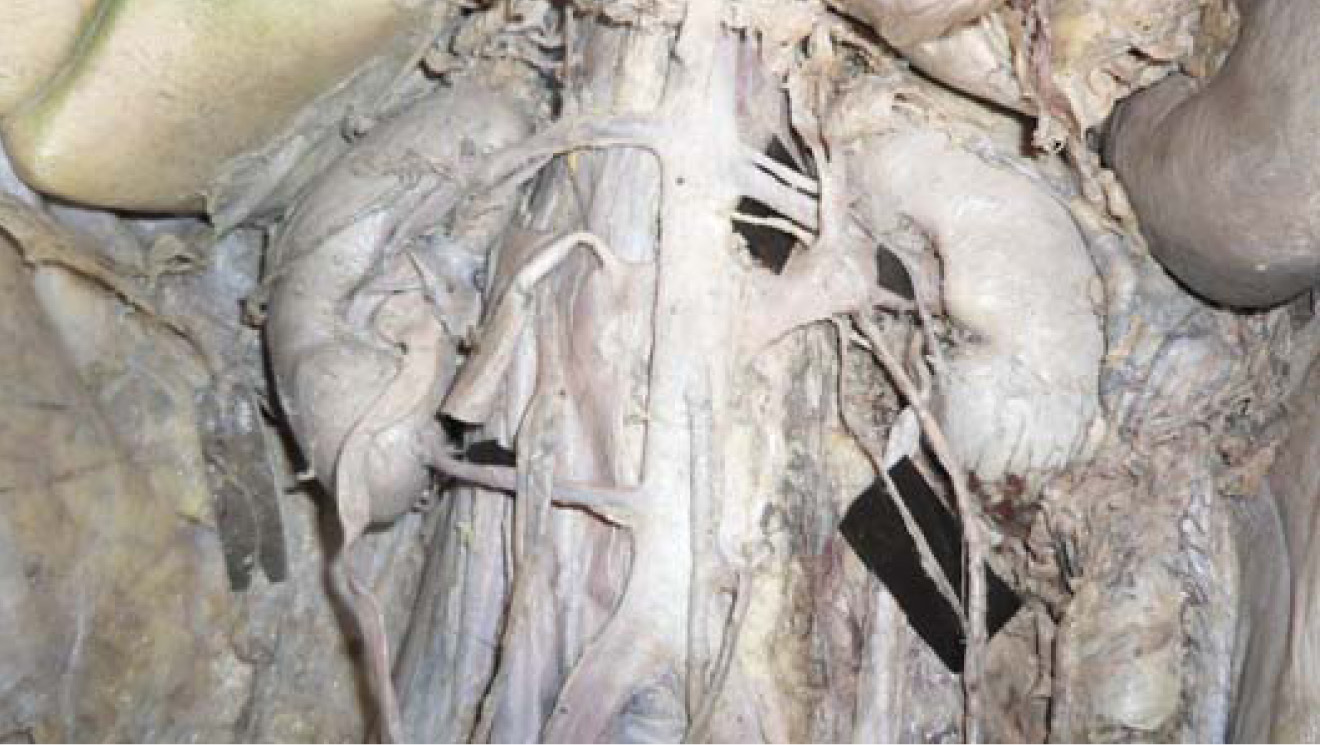
A significant variation was observed in the course of left renal vein. In the present case, it passed behind the aorta to join inferior vena cava and so, it was called as retro aortic left renal vein (RALRV) [Table/Fig-2]. In addition, left renal vein was crossed superficially by lower polar branch of aberrant left renal artery, near the hilum of left kidney. Right renal vein was normal in its course. No other associated anomalies were found.
Showing the course of Upper Right renal artery behind inferior vena cava
Discussion
The mesonephric arteries extended from the sixth cervical to the third lumbar segments. The more cranial of these vessels disappeared before those at the caudal end had reached their maximal development. In the upper lumbar region, the mesonephric arteries formed a network, the rete arteriosum urogenitale, from which the reproductive gland, the mesonephros and later, the metanephros, were supplied with arterial segments. It was inferred that early division of renal artery was the result of a variation in the degeneration of the rete arteriosum. Accessory renal arteries which arose from the aorta were persistent mesonephric arteries. Aberrant renal arteries were in fact normal segmental arteries with a proximal origin, which accounted for multiple or supernumery arteries of renal pedicle [1].
Aberrant renal arteries were observed twice as often as accessory renal arteries. The frequency rate of ERA was the same on the right and left sides, and in 12% of the general population, ERA is bilateral. It has been reported that ERA are detected less in angiography studies than in anatomic dissection studies. In several angiographic studies, ERA frequency rate was between 20% and 27%. This rate was 24% in an angiographic study which was conducted on 855 patients by Ugur Ozkan et al., [2]. The reason why ERA are detected with a lesser frequency in angiographic series, is that thin arteries which originate directly from the aorta cannot be observed in angiography, and/or arteries that enter parenchyma directly without passing the renal hilus are frequently confused with adrenal or capsular arteries [2].
Brodie et al., in an anatomical study, reported six cases with a retro ureteric passage of aberrant renal artery [3]. In a considerable number of cases, arteries that pass behind or in front of renal pelvis were attributed to cause uretero pelvic obstructions.
Aberrant right superior polar artery from abdominal aorta at lower border of L1 was reported by Ramesh et al., [4]. The present observation of an aberrant bipolar artery has never been reported before.
The development of the renal veins is a part of the complex developmental process of the IVC and errors in such a process are mainly responsible for the variations. The retro aortic left renal vein (RLRV) results from persistence of dorsal limb instead of ventral limb in circum aortic collar of veins.
Left renal vein abnormalities were categorised into four types. The present observation of a left renal vein with a retro aortic course comes under type 1, in which ventral pre aortic limb of left renal vein is obliterated, but the dorsal retro aortic limb persists and joins inferior vena cava in orthotopic position [5]. The incidence of this type of anomaly is comparatively rare. In a CT study which was done by Trigaux et al., which included 1014 cases, such a vein was seen in 3.7% cases [6]. Among a series of 1008 kidneys which were studied by Satyapal et al; only 0.5% specimens had such an anomaly [7]. In another radiological study which was conducted by B Yagci et al., out of 783 patients, only 22 had retro aortic left renal veins. RLRV is a significant variation and it is commonly asymptomatic, but its compression can cause haematuria, proteinuria, gonadal varices, flank pain or a combination of any of these symptoms [8].
Conclusion
During renal surgeries, these kinds of anatomical variations in renal vessels can influence the technical feasibility of the operations. A failure in recognizing these anomalies may lead to a severe haemorrhage and it may result in complications and graft loss. Hence, a careful pre operative evaluation is essential in all cases, for a safe out come. Particularly, in view of constantly increasing renal transplantations and kidney retrieval surgeries, the variations in renal vasculature are valuable.
[1]. Graves FT, The aberrant renal arteryJ Anat 1956 90:553-58. [Google Scholar]
[2]. Ozkan Ugur, Ozkurt Levent, Tercan Fahri, Osman Kızılkılıç, Koç Zafer, Nihal Koca Renal artery origins and variations: angiographic evaluation of 855 consecutive patientsDiagn Interv Radiol 2006 12:183-86. [Google Scholar]
[3]. Bordei P, Sapte E, Iliescu D, Double renal arteries originating from the aortaSurg Radiol Anat 2004 Dec 26(6):474-79. [Google Scholar]
[4]. Rao T Ramesh, Rachana Aberrant renal arteries and its clinical significance: A case reportInternational Journal of Anatomical Variations 2011 4:37-39. [Google Scholar]
[5]. Mayo J, Gray R, St Louis E, Grosman H, McLoughlin M, Wise D, Anomalies of the inferior vena cavaAJR Am J Roentgenol 1983 140:339-45. [Google Scholar]
[6]. Trigaux JP, Vandroogenbroek S, De Wispelaere JF, Lacrosse M, Jamart J, Congenital anomalies of the inferior vena cava and left renal vein: evaluation with spiral CTJ Vasc Interv Radiol 1998 9:339-45. [Google Scholar]
[7]. Satyapal KS, Kalideen JM, Haffejee AA, Singh B, Robbs JV, Left renal vein variationsSurg Radiol Anat 1999 21:77-81. [Google Scholar]
[8]. Yagci B, Tavasli B, Karabulut N, Kiroglu Y, Clinical significance and renal hemodynamics of incidentally detected retro aortic left renal vein: assessment with venous Doppler sonographyBritish Journal of Radiology 2008 81:187-91. [Google Scholar]