According to the World Health Organization (WHO) report, India has 31.7 million diabetic subjects, and the number is expected to increase to an alarming 79.4 million by 2030 [1]. These clinical differences and the increasing prevalence of diabetes mellitus (DM) in India [2] emphasise need for epidemiologic studies on diabetes-related complications among type 2 diabetic population. Diabetic retinopathy (DR) is one of the complications of diabetes, which affects the microvasculature of retina. It is the leading cause of a visual impairment. It is shown to cause visual impairment in more than 86% type 1 diabetic patients and in 33% type 2 diabetic patients [3,4]. In epidemiological studies which have been done in the past, it has been seen that nearly all type 1 patients and 75% type 2 patients develop DR within 15 to 20 years of being diagnosed as having DM [5].
Prevalence of DR in India varies from study to study. Raman et al., found a prevalence of 18% in diabetic population, whereas Agrawal RP et al., found a prevalence of 28.9% in type 2 diabetic population [6,7]. Although various population and hospital based studies have been conducted in northern [7] and southern [8] parts of India to estimate the prevalence of DR in type 2 diabetic population, there is a paucity in the literature regarding the prevalence of DR in western India. With above context, a hospital-based, cross-sectional study was designed to find out prevalence of DR and effect of duration of diabetes on severity of DR in western Indian, type 2 diabetic population.
Material and Methods
This study was conducted in a medical college and a hospital in western India, during October 2007 to September 2009. A total number of 168 patients who visited the diabetic clinic and were diagnosed for type 2 DM were selected for the study. Diagnosis of diabetes was made in each case by doing a standard oral GTT with a 75gm glucose load by using the recommendations of ADA (American Diabetic Association) for type 2 DM [9].
Inclusion criteria: Patients who were diagnosed with NIDDM (non-insulin dependent diabetes mellitus), who gave their consents for participation in the study.
Exclusion criteria: Patients with mature cataracts and hazy media, whose fundi could not be examined. Patients with a history of exposure to radiation, hypertensive retinopathy without DM, sickle cell disease and pheochromocytoma were also excluded, as these conditions could mimic fundus features with diabetic retinopathy. A history of hypertension was taken and a blood pressure measurement was carried out. All the patients who were selected for study underwent detailed opthalmoscopic examinations. They were performed by same examiner under constant environmental conditions and on same machine to avoid errors in the data collection. An approval was obtained from institutional ethics committee. Informed consents were taken from all the subjects and the study was carried out in accordance with the World Medical Association – Declaration of Helsinki.
After taking a detailed history, a routine ophthalmological examination was done. The pupils of both eyes were dilated by using a mydiatric agent (1% Tropicamide eye drops). Distant direct opthalmoscopy, direct opthalmoscopy and binocular indirect opthalmoscopy were done. Binocular indirect ophthalmoscopy was done with a 20 D lens with the patient in supine position. Findings were noted and patients were categorized according to findings; whether diabetic retinopathy was present or absent. If present, retinopathy was classified according to early treatment of diabetic retinopathy study (ETDRS) classification [5, 10]. Presence of diabetic macular oedema was noted. If present, it was further classified into clinically significant (CSME) or non-significant.
Statistical Analysis
Data was analysed by using epi-info statistical software. Mean, standard deviation, range and percentage were calculated. Prevalence of DR was calculated as the ratio of the number of participants with DR in one or both eyes to the total number of diabetic patients who were evaluated. All confidence intervals were presented at 95% and all analyses were conducted at a <0.05 significance level. Chi – square test and Fisher – Exact test (2-tailed) were used to find out statistically significance differences, wherever they were applicable.
Results
[Table/Fig-1] shows age, gender and duration of diabetes in 168 patients who were studied. Ninety four were male patients with a mean age of 52.26±10.31 years (age range 35-70 years) and 74 were female patients with a mean age of 53.97±11.02 years (age range 30-72 years). Duration of diabetes was longer in female participants as compared to that in males.
Demographic profile of diabetic population under study (Values in parenthesis indicate age range, * Standard Deviation)
| No. of Participants (N=168) | Age in years (Mean±SD*) | Duration of diabetes in years (Mean±SD*) |
|---|
| Male (N=94) | 52.26±10.31 (35-70) | 13.71± 7.51 |
| Female N=74 | 53.97±11.02 (30-72) | 15.78± 9.23 |
[Table/Fig-2] shows the prevalence of diabetic retinopathy (DR). Out of 168 diabetic patients who were studied, 57 patients (33.92%) had diabetic retinopathy. Out of 57 patients with DR, 43 patients (25.59%) had NPDR and 14 patients (8.33%) had PDR.
Prevalence of DR (Total, NPDR and PDR)
| Total no. of patients (pts) | Percentage of pts with *DR (Total) | Percentage of pts with #NPDR | Percentage of pts with †PDR |
|---|
| 168 | 33.92 (57) | 25.59(43) | 8.33(14) |
(Values in parenthesis indicate number of patients, *Diabetic retinopathy, #Non-proliferative diabetic retinopathy, †Proliferative diabetic retinopathy)
Vision ranged from 20/20 to Fc close to face in different patients, vision was poor in patients with diabetic retinopathy, and it deteriorated as grade of diabetic retinopathy advanced [Table/Fig- 3].
Vision (mode value) in patients without DR, with NPDR, with PDR
| Best Corrected visual acuity (Mode Value) |
|---|
| Patients without DR | 20/20 |
| Patients with NPDR | 20/40 |
| Patients with PDR | 20/200 |
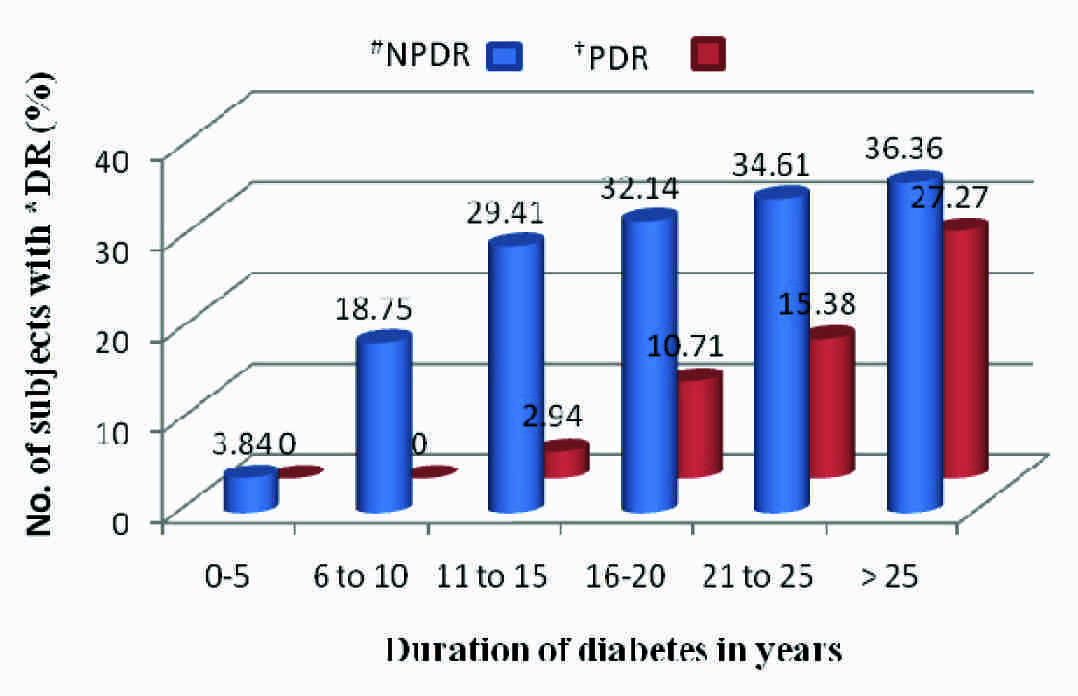
[Table/Fig-4] shows severity of DR in groups of patients who were classified according to duration of diabetes (Diabetic age). Comparison between different groups showed a p value of < 0.05 on Chi square test. Statistically significant differences (p values of <0.05) were observed between prevalences of NPDR and PDR in each group.
Severity of retinopathy in relation to age of type 2 diabetes mellitus patients *diabetic retinopathy; #non-proliferative DR; †proliferative DR
[Table/Fig-5] shows the prevalence of various stages of NPDR (mild, moderate, severe and very severe) and PDR (early and high risk) with duration of DM. Severities of NPDR and PDR were found to increase with an increased duration of DM.
Prevalence of various stages of NPDR and PDR with duration of diabetes.
| Duration of *DM in years | No. of patients (pts) | % of pts with Mild #NPDR | % of pts with Moderate NPDR | % of pts with Severe NPDR | % of pts with very Severe NPDR | % of pts with Early †PDR | % of pts with high risk PDR |
|---|
| 0-5 | 26 | 3.84 (1) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| 6-10 | 32 | 9.37 (3) | 3.12 (1) | 3.12 (1) | 3.12 (1) | 0 (0) | 0 (0) |
| 11-15 | 34 | 2.94 (1) | 5.88 (2) | 8.82 (3) | 11.76 (4) | 2.94 (1) | 0 (0) |
| 16-20 | 28 | 0 (0) | 3.57 (1) | 10.71(3) | 17.85 (5) | 7.14 (2) | 3.57 (1) |
| 21-25 | 26 | 0 (0) | 0 (0) | 7.69 (2) | 26.92 (7) | 7.69 (2) | 7.69 (2) |
| > 25 | 22 | 0 (0) | 0 (0) | 0 (0) | 36.36 (8) | 9.09 (2) | 18.18 (4) |
(Values in parenthesis indicate number of patients. *diabetes mellitus, #Non-proliferative diabetic retinopathy, †Proliferative diabetic retinopathy.)
Out of 168 patients, 11 patients (6.5%) developed CSME (clinically significant macular oedema). Prevalence of CSME increased with increasing diabetic age [Table/Fig-6].
Prevalence of CSME with duration of diabetes
| Duration of NIDDM* in year’s | Total no of patients | % of patient with CSME |
|---|
| 0-5 | 26 | 0(0) |
| 6-10 | 32 | 0(0) |
| 11-15 | 34 | 2.94(1) |
| 16-20 | 28 | 7.14(2) |
| 21-25 | 26 | 15.38(4) |
| >25 | 22 | 22.73(5) |
(Values in parenthesis indicate number of patients. *non – insulin dependent diabetes mellitus)
A significant difference (p value<0.05) was observed between prevalence of CSME in each group.
[Table/Fig-7] shows that with associated hypertension, prevalence of DR increased. A statistically significant difference was observed between two groups.
Prevalence of diabetic retinopathy in NIDDM cases with Hypertension
| Category of NIDDM patients | Total no of patients | Percentage of patients with retinopathy | P value (Fisher Exact test) |
|---|
| NIDDM with Associated hypertension (HT) | 32 | 46.88(15) | (P value <0.05) |
| NIDDM without associated HT | 136 | 30.88(42) |
(Values in parenthesis indicate number of patients. *non – insulin dependent diabetes mellitus)
Discussion
Diabetic retinopathy (DR) is a well known complication of diabetes mellitus (DM). Prevalence of DR differs in type 1 and type 2 DM. A registry for prevalence of type 1 cases has recently been set up in India. Hence, we have paucity of data on prevalence of DR in type 1 cases. Different population and hospital based studies which were done to establish prevalence of DR in diabetic populations, have been summarized in [Table/Fig-8].
Prevalence of DR in different populations in India
| Study and authors | Year | Region/area & type of population studied | Total No. of cases | % DR, % NPDR and % PDR |
|---|
| Present study | 2009 | Urban & Rural Western India Type 2 DM | 168 | 33.92 25.59, 8.33 |
| Rema M et al., [11] | 1996 | Urban & rural South India Type 2 DM | 6792 | 34.1, 30.8, 3.4 |
| Agrawal R P et al., [7] | 2000 | Urban & rural North India Type 2 DM | 4067 | 28.9, 23.06, 5.9 |
| Narendran V et al., [12] | 2002 | Urban & rural South India Type 1 & type 2 DM | 260 | 26.2, 24.6, 1.6 |
| Rema M et al., CURES Eye Study, I [8] | 2005 | Urban South India Type 2 DM | 1382 | 17.6, 16.6, 0.9 |
| Mahesh G et al[13] | 2005 | Urban & rural South India Type1 & type 2 DM | 323 | 20.12, 10.84, ------ |
There was an increase in prevalence of diabetes in Indian urban population due to life style changes which pertained to changes in socioeconomic status [14]. Several studies from the world and India have also tried to find out prevalence of different complications of DM. [Table/Fig-8] has compared the prevalence of diabetic retinopathy, including its stages NPDR and PDR, in different populations from south, north and western India.
The present hospital – based, cross-sectional study showed that the prevalence of diabetic retinopathy (DR) was 33.92% (NPDR- 25.59%, PDR - 8.33%) in type 2 DM patients of western India. Overall, prevalence of DR in hospital based studies [7,11], including present study was higher as compared to those in population based epidemiological studies [8,12,13]. This observation may be attributed to the fact that there was a referral bias among the diabetic patients who were reported to tertiary care centres. Hence, with larger number of diabetics with higher diabetic ages reporting to the diabetic clinic, it is more likely that prevalence of complications may also be larger. In a recent, population based, cross – sectional study which was done at Chennai on urban diabetic population an 18% prevalence of DR was observed [6]. It further strengthens referral biased differences in hospital and population based studies.
Overall, prevalence which was observed in present study was similar to that which was observed by Rema et al., and Agrawal RP et al., in spite of the fact that in present study, sample size is smallest among all studies. Prevalences of NPDR and PDR matched well with those which were observed by Agrawal RP et al., only. Although NPDR was more prevalent as compared to PDR in all the studies, the observation that more PDR cases were observed in the present study and Agrawal RP et al., study, needs special attention. Both these studies share a close geographical cohort in western and northern India. Possibility of existence of differences in prevalence of DR in ethnic groups was suspected in Asian Young Diabetes Research (ASDIAB) study [15]. Although it is premature to say that such differences may exist among Indian populations of different geographical origins, this possibility may be explored by doing larger population based studies across the nation.
We observed an increase in severity of DR as age of diabetics advanced. This further strengthened the fact that duration of diabetes was single most common predictor which affected severity of DR [6]. According to our findings, DR may appear as early as 0-5 years of having diabetes and more than 90% of patients develop DR after 25 years of having the disease. PDR was seen after 11 years of having diabetes and after 25 years of having it, 100% cases were in severe stages of DR. Prevalence of CSME increased with increasing age of diabetics. Similar observations were evident in studies which were done in the past [16–18]. Associated hypertension is a known risk factor for development of diabetic retinopathy [19]. Our study supported this fact.
Limitations and Strengths of Our Study
Smaller sample sizes, referral biases and cross sectional studies are major limitations due to which results are difficult to extrapolate in larger populations. Its strength lies in the fact that this was a first study of its kind which assessed the prevalence of DR in western Indian population by using retinal photographs and standard grading (ETDRS) technique.
Conclusion
The prevalence of diabetic retinopathy was 33.92% in Type 2 DM patients of western India. PDR was evident only after 11 years of having diabetes. 100% cases developed severe DR after 25 years of having diabetes. Thus, it can be concluded that age of diabetes and severity of DR goes hand in hand. The duration of diabetes is the strongest predictor for diabetic retinopathy. Associated hypertension is a risk factor for development of DR.
(Values in parenthesis indicate number of patients, *Diabetic retinopathy, #Non-proliferative diabetic retinopathy, †Proliferative diabetic retinopathy)
(Values in parenthesis indicate number of patients. *diabetes mellitus, #Non-proliferative diabetic retinopathy, †Proliferative diabetic retinopathy.)
(Values in parenthesis indicate number of patients. *non – insulin dependent diabetes mellitus)
(Values in parenthesis indicate number of patients. *non – insulin dependent diabetes mellitus)