It has been documented that the elderly are prone to psychological problems, among which depression is the commonest. In fact, the elderly in India face a multitude of psychological, social and physical health problems. As the age advances, there is increased morbidity and functional loss, the presence of a variety of depressive factors and the occurrence of varying life events like the death of the spouse, retirement and interpersonal difficulties with family members, poverty and loneliness. These situations greatly impact the psychological statuses of the elderly, making them prone to depression.
The depression among the elderly manifests as a major or a minor depression which is characterized by a collection of depressive symptoms [1]. Ten percent of the people who are older than 65 years have depressive symptoms and one percent have major depressive disorders [2]. Many studies have indicated a severe under-recognition and under-treatment of depression in the elderly, even in the developed counties [3–5].
The depression in the elderly should never be considered as a natural consequence of ageing. It usually has an atypical presentation. It can manifest as a symptom eg: as a reaction to stress: as a syndrome ex: secondary to hypertension or Parkinson’s disease; and as an illness e.g. endogenous depression [6]. Depression as a major risk factor for suicide among the elderly, also has been reported.
In India, most of the elderly live in the rural areas and the access to the health care facilities is meagre. The depressive symptoms are likely to be dismissed as “normal” by the older persons, their family members and even by health care providers. Given the relative ease with which the depressive illness can be diagnosed and treated, there is enormous potential for alleviating this largely neglected public health burden among the elderly [7]. Community studies from India on the depression among the elderly are sparse. Taking into consideration the above factors, this study was conducted in a rural area with the following objectives:
Material and Methods
A cross – sectional, descriptive study was carried out in 9 villages which were selected randomly. These areas were covered by the field practising areas of the Chandragiri Rural Health Centre of S.V. Medical College in Chittoor district of Andhra Pradesh, India. The study period was from April 2009 to September 2009.
Sample Size
The sample size for the present study was calculated by using the following formula at a 95% confidence interval, with an allowable error of 10%:
N= 4 pq / L2 Where
N= a minimum sample size required.
p = the expected prevalence rate (%) of depression among the geriatric age group.
q = 100 – p (%).
L = The margin of the sampling error allowed (%)/Allowable sampling error.
Various earlier Indian studies have revealed that the prevalence of depression among the old age people ranged from 6% to 58%. Hence, a prevalence of 55% was assumed for the purpose of computing the size of the sample which was required for the present study.
Thus, the sample size for the present study was determined as follows:
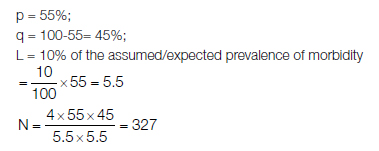
Thus, the sample size of a 400 strong population of age 60 years and above was found to be sufficient for this study.
The sample sizes of 400 elderly subjects who were aged 60 years and above, of both the sexes (equal numbers), were contacted through house-to-house visits in the study villages for the data collection. In each household, the head of the family or another responsible adult was contacted and the nature and the purpose of the study was explained to him/her. When more than two persons of age 60 years and above were present in the same house, two persons of the opposite sex i.e. one from either sex were selected as the study subjects and between the persons of the same sex group, the elder person was given preference and was selected as the study subject. Thus, a maximum of two persons were taken from one house as the study subjects. If the particular elderly person was not present at the time of the survey, the house was revisited. The elderly persons who were not available in spite of repeated visits to their houses and those who did not gave their consents for participation in the study were not taken up for the study. The information regarding their ages was crosschecked by asking their children’s age(s), with respect to some major events and by verifications by using records like the ration card, etc. The identified 400 older subjects was interviewed in their local languages and they were examined by using a pre-tested, pre-structured, study questionnaire. The questionnaire was divided into two parts. The first part comprised of the socio-demographic information which covered a diverse set of parameters such as age, sex, marital status, education, socio-economic status, living conditions, economic dependency and the dependency for the activities of daily living.
Definition of the variables which were used in the study
The socio-economic status of the study subjects[Table/Fig-1],[8].
The socio-economic status of the study subjects.
| Social status | Score |
|---|
| Upper high | > 76 |
| High | 61–75 |
| Upper middle | 46–60 |
| Lower middle | 31–45 |
| Poor | 16 – 30 |
| Very poor or below poverty line | < 15 |
Economic dependency
The subjects were categorized into three types. Economically independent, economically partially dependent and economically totally dependent.
The subjects were considered to be ‘economically independent’ if they were leading economically productive lives or if they were getting any pension (in case of retired employees or their widowed spouses).
The subjects were considered to be economically ‘partially dependent’ if they were having a small income like an old age pension and were depending on their family members for their livelihood. But in case of the subjects who were living alone, even getting the small amount like the ‘old age pension’ was considered to be ‘an economical independency’.
The subjects were considered to be economically ‘totally dependent’ if they were not getting any income and were totally dependent on the family members for their livelihood.
The Activities of Daily Living (ADL)
With respect to the activities of daily living, the subjects were divided into three categories i.e. independent for the activities of daily living, partially dependent for the activities of daily living and totally dependent for the activities of daily living.
A subject was considered to be ‘independent’ for the activities of daily living if he/she was able to conduct the activities of daily living like brushing, bathing, rising from the bed, going to the bathroom, dressing and undressing on his/her own without requiring any sort of help from others.
A subject was considered to be ‘partially dependent’ for the activities of daily living if he/she needed some help from others
A subject was considered to be ‘totally dependent’ for the activities of daily living if he/she was totally dependent on others.
The second part comprised of a scale which was known as the “Yesavage’s Geriatric Depression Scale (GDS) –Shorter version,” which was used for measuring the depression in the elderly [9].
The Geriatric Depression Scale which was used was specifically developed for the older population. Originally, it is a 30 question scale, but a shorter version is more suitable for the general practice and hence, Yesavage’s Geriatric Depression Scale (GDS) – Shorter version was used to detect whether the study subject was having depression or not. It is a screening tool and not a diagnostic one, which has a sensitivity of 92% and a specificity of 89% in a community sample. The validity and the reliability of the tool have been supported both in the clinical practice and in research. So, the researcher selected this scale for estimating the prevalence rate of depression among the elderly. The shorter version of the scale consists of 15 questions that are simple and clear. The participants were asked to respond to 15 questions by answering ‘yes’ or ‘no’ in reference to how they felt on the day on which the questionnaire was administered. Each negative answer would carry 1 point and thus, the more the scores were, the more were the chances of having depression. A score of > 5 was suggestive of depression. The maximum score that one could get was 15, which would indicate severe depression. Based on their scores, the study subjects were categorised as follows[Table/Fig-2]:
Based on their scores, the study subjects were categorised
| Score | Category |
|---|
| 0-5 (< 5) | Normal |
| 6-15 (> 5) | Depression Present |
Translation of the tool: The tool was translated from English to Telugu and back to English by language experts. The validity of the translated tool was established by two other experts by using verbatim.
The statistical methods which were used: The data was analysed by using SPSS (Statistical Package for Social Sciences), version 17 and the results were recorded as frequencies, means ± Standard deviations (SD) and p - values. Tables were used for a comprehensive viewing of the results. The Chi-square test was used for the categorical variables. A p-value of < 0.05 was taken as the criteria of significance for all purposes. In this study, the different variables like age, sex, education, socio-economic status, living arrangement, economic dependency, dependency for the activities of daily living and the Yesavage’s Geriatric Depression Scale (GDS) –Shorter version score ( 0 – 5 depression not present (normal) and 6 – 15 depression present) were taken into consideration.
Results
A majority (48.8%) of the subjects were in the age group of 60 – 69 years. The prevalence of depression in the current study was 47.0%. In the present study, the prevalence of depression was found to increase with increasing age. It was 40.0% in the age group of 60-69 years, while it was 53.3% in the age group of 70-79 years and it was 54.3% in the 80 years and above age group. The difference in the prevalence of depression between the different age groups was found to be statistically significant [Table/Fig-3]. A significantly higher prevalence of depression was found in females (56.5%) than in males (37.5%). In males, the mean depression score was 5.53 + 3.28, while it was 6.80 + 3.10 in females [Table/Fig-4]. Among the illiterates, 59.0% had depression, while 35.1% of those who had studied upto the primary school level had it [Table/Fig-3]. This difference was statistically significant. The depression status was 25.0% among the elderly of the upper socio-economic status, while it was 86.1% among the below poverty subjects and this difference was statistically significant [Table/Fig-3].
Prevalence of depression based on various variables.
| Variable | Normal (n=212) | Depression present (n=188) | χ2 value | p - value | Significance |
|---|
| No | % | No | % |
|---|
| Age (years) | | | | | | | |
| 60 – 69 | 117 | 60.0 | 78 | 40.0 | | | |
| 70 – 79 | 63 | 46.7 | 72 | 53.3 | 6.16 | p < 0.05 | S |
| > 80 | 32 | 45.7 | 38 | 54.3 | | | |
| Sex | | | | | | | |
| Male | 125 | 62.5 | 75 | 37.5 | 14.49 | p < 0.001 | S |
| Female | 87 | 43.5 | 113 | 56.5 | | | |
| Literacy status | | | | | | | |
| Illiterate | 103 | 41.0 | 148 | 59.0 | | | |
| Primary | 48 | 64.9 | 26 | 35.1 | 42.79 | p < 0.001 | S |
| Secondary | 50 | 82.0 | 11 | 18.0 | | | |
| Higher secondary & above | 11 | 78.6 | 3 | 21.4 | | | |
| Socio-economic status | | | | | | | |
| Upper high | 6 | 75.0 | 2 | 25.0 | | | |
| High | 29 | 93.6 | 2 | 6.4 | 75.57 | p < 0.001 | S |
| Upper middle | 63 | 75.0 | 21 | 25.0 | | | |
| Lower middle | 70 | 60.3 | 46 | 39.7 | | | |
| Poor | 38 | 32.2 | 80 | 67.8 | | | |
| Very poor/Below poverty line | 6 | 13.9 | 37 | 86.1 | | | |
| Living arrangement | | | | | | | |
| Alone | 7 | 12.7 | 48 | 87.3 | | | |
| With spouse | 56 | 61.5 | 35 | 38.5 | | | |
| With spouse & children | 80 | 74.8 | 27 | 25.2 | 61.53 | P < 0.001 | S |
| With children | 57 | 45.6 | 68 | 54.5 | | | |
| With others | 12 | 54.5 | 10 | 45.5 | | | |
| Economic dependency | | | | | | | |
| Independent | 99 | 52.7 | 89 | 47.3 | | | |
| Partially dependent | 18 | 36.7 | 31 | 63.3 | 7.05 | P < 0.05 | S |
| Totally dependent | 95 | 58.3 | 68 | 41.7 | | | |
| Dependency in activities of daily living | | | | | | | |
| Independent | 207 | 55.2 | 168 | 44.8 | | |
| Partially dependent | 5 | 21.7 | 18 | 78.3 | 12.64 | P < 0.001 | S |
| Totally dependent | 0 | 0.0 | 2 | 100.0 | | | |
Mean, SD and t-value of the scores of Depression according to sex
| Sex | Depression present | t-value |
|---|
| Mean | SD |
|---|
| Men | 5.53 | 3.28 | 3.97* |
| Women | 6.80 | 3.10 |
| Total | 6.16 | 3.40 | |
*Significance at 0.001 level.
The depression was more prevalent among the subjects who were living alone (87.3%) and it was least among the subjects who were living with their spouses and children (25.2%) [Table/Fig-3]. The difference in the prevalence of depression between the various groups was statistically significant.
The depression status was high (47.3%) among the economically independent elderly, while it was 41.7% among the totally dependent individuals and it was statistically significant [Table/Fig-3]. Among those elderly who were depending totally for their activities of daily living, the depression status was 100.0%, while it was 44.8% only in those elderly who could carry out their activities of daily living independently [Table/Fig-3]. The difference was also statistically significant.
Discussion
The overall prevalence of depression was found to be 47.0%. Hughes et al., and Venkoba Rao’s studies revealed the prevalence of depression to be 61.5% and 43.0% respectively [10,11]. Various studies have revealed that the prevalence rates for depression in the community samples of the elderly in India varied from 6% to 58% [12–15].
In the present study, the prevalence of depression was found to increase with increasing age. Some of the reasons for the sudden increase in the prevalence after the age of 69 years may be an increased economical and physical dependency, loss of the spouse, negligence by the family members and loss of self esteem. Similar findings were found in Jariwala Vishal et al’s and Raj Kumar et al’s studies [12,14].
The prevalence of depression was found to be significantly more in elderly females (56.5%) than in the male subjects (37.5%). The mean score of the depression was high in females (6.80 + 3.10) as compared to that in males (5.53 + 3.28) and the overall mean score of depression in the study subjects was 6.16 + 3.40. More prevalence of widowhood than among the male counter parts, living alone or negligence by the family members, a poor status in the family, increased physical dependency, lack of income and poor health may be the reasons for the increased prevalence of depression among the elderly females. The differences in the prevalence and the mean scores of depression between the male and female subjects were statistically significant (t = 3.97; p <0.001). Ramachandran et al., study observed that depression was significantly more frequent in females than in males, which was similar to the findings of the present study [16]. Goswami et al., study found that the prevalence of depression was 44.5% and 63.2% among male and female subjects respectively [17]. In the study of Jain RK, the prevalence of depression was found to be 45.9% in males and 57.8% in females, with the mean score being 5.10+8.26 [18]. Findings which were similar to those of the current study were also observed in the studies which were conducted by Jariwala Vishal et al., Nandi PS et al., and Rajkumar et al., [12–14].
In the present study, the prevalence of depression was found to be inversely proportional to the literacy status. There was a gradual decrease in the prevalence of depression as the literacy status increased. Various studies which were conducted in India revealed similar findings as those of the current study [14,16]. There was a gradual increase in the prevalence of depression from the higher to the lower socio-economic status. The prevalence was significantly high among the subjects who were living below the poverty line (86.1%), while it was 25.0% among the upper high socio-economic group. Similar findings were also observed in Raj kumar et al., Ramachandran et al., and Jain RK’s studies [14,16,18]. The sudden spurt in the prevalence among the subjects of the lower socio economic status reflected the role of economic dependency and thereby, negligence by the family members. The associated high prevalence of illiteracy in this group might be an additional factor for the increased economical dependency. The difference in the prevalence of depression between the subjects of different socio-economic statuses was statistically significant (χ2= 75.57; p <0.001).
In the present study, the prevalence of depression varied among the subjects who had different living arrangements. The subjects who were living alone had a significantly high prevalence of depression (87.3%) as compared to the other subjects. The lowest prevalence (25.2%) was found among the subjects who lived with their spouses and children. This reflected ‘the loss of spouse’ as one of the most important factors which were responsible for the increased prevalence of depression. The negligence by children, feeling of loneliness, a poor status in the family and a sense of insecurity may be the reasons for the increased prevalence of depression in these subjects as compared to those in those who were living with their spouses and children. Several studies also found that the prevalence of depression was significantly high among the elderly who lived alone [19,20]. The difference in the prevalence of depression between the subjects who had different living arrangements was found to be statistically significant (χ2 = 61.53; p <0.001).
In the present study, 47.3% of the economically independent subjects had depression. It was 63.3% among the partially dependent subjects and it was 41.7% among the totally dependent subjects. The reasons for the increased prevalence of depression among the partially dependent subjects may have been a poor status in the family, lack of sufficient money for their medical needs, loss of the spouse, loneliness, dissatisfaction with the quality of life, poor health and dependency for the activities of daily living. Among the totally dependent subject(s), the lack of responsibilities, the presence of an earning spouse, good family relationships and proper care from the spouse and/or children and a feeling of security may have been the reasons for the lesser prevalence of depression. The study of Jain RK showed that the socio-economic status, illiteracy, and dependency had a statistically significant effect on the depression, which is similar to that which was seen in the current study [18]. The difference in the prevalence of depression between the subjects of different categories with regards to the economic dependency was found to be statistically significant (χ2= 7.05; p <0.05).
In the present study, it was found that the prevalence of depression increased as the dependency in the activities of daily living increased. 44.8% of the subjects who were capable of carrying out the activities of daily living independently had depression, while it was 78.3% of the partially dependent subjects. All the subjects (100.0%) who were totally dependent on others for the activities of daily living had depression. The increased dependency for the activities of daily living and the associated economic dependency, a poor status in the family, loss of the caring spouse, a lack of leisure time activities, an increased feeling of loneliness and poor health may have been the reasons for the increased prevalence of depression as the dependency increased. The difference in the prevalence of depression between the subjects of different categories with regards to the activities of daily living was found to be statistically significant (χ2= 12.64; p <0.001).
Conclusion
The prevalence of depression was found to be positively associated with the female sex, increasing age, the educational status, a low socio-economic status, those who were living alone, economic dependency and dependency for the activities of daily living. Doing research on the treatments for depression, integrating them in the training programmes for the community and for the general health workers and collaborating with non-governmental organisations, are the key factors for meeting the mental health needs of the elderly subjects.
*Significance at 0.001 level.