Prevalence of the Trichomonas Vaginalis Infection in A Tertiary Care Hospital in Rural Bangalore, Southern India
Dharma Vijaya MN1, KM Umashankar2, Abed Gulab Nagure4, G. Kavitha5
1 Associate Professor, Department of Obstetrics and Gynaecology, MVJ Medical College, Bangalore, India.
2 Assistant Professor, Department of Obstetrics and Gynaecology, MVJ Medical College, Bangalore, India.
3 Assistant Professor, Department of Obstetrics and Gynaecology, MVJ Medical College, Bangalore, India.
4 Senior Resident, Department of Obstetrics and Gynaecology, MVJ Medical College, Bangalore, India.
5 Senior Resident, Department of Obstetrics and Gynaecology, MVJ Medical College, Bangalore, India.
Name, Address, E-Mail Id of The Corresponding Author: Dr Umashankar KM, Assistant Professor, Department of Obstetrics and Gynaecology, No 106 4th Main Road Nr Colony Bangalore, India.
Phone: 9986909374
E-mail: ukumashankar@gmail.com
Background: The infection with Trichomonas Vaginalis is one of the most common sexually transmitted diseases (STDs) in humans. The prevalence of this infection has been reported to be between 2 to 8%, depending on the different socio-cultural conditions. This study aimed to determine the prevalence of T. vaginalis in the women who were referred to the gynaecologic clinics at the MVJ medical college, Bangalore, India.
Methods: This descriptive, cross-sectional study was conducted on 750 women who were referred to the gynaecologic clinics from October 2010 to September 2012. Vaginal samples were obtained from them and they were examined by wet mount and culture methods for the detection of T. vaginalis.
Results: Sixteen out of the 750 vaginal swab specimens (2.1%) were culture positive for T. vaginalis and 13 among these positive specimens (1.7%) were wet mount positive. Only 12 of the 42 patients who were clinically diagnosed as having the T. vaginalis infection, were confirmed by the culture method. Five hundred and fifty of the participants (73.3%) had at least one of signs and symptoms of trichomoniasis. No statistical correlation was observed between the clinical manifestations and the parasitological results (p>0.05).
Conclusion: This study showed a low prevalence of the T. vaginalis infection in the study population. Since the clinical signs of trichomonal vaginitis are the same as those of other STDs, a confirmatory laboratory diagnosis is necessary. Wet smears, as well as culture, are sensitive for the detection of T. vaginalis.
Trichomonas Vaginalis infection, Wet mount, Culture
Introduction
Trichomonas Vaginalis is a flagellated protozoan that causes trichomoniasis in human, which is a sexually transmitted disease (STD) [1]. The World Health Organization (WHO) has estimated that more than 170 million people are infected annually with T. vaginalis throughout the world [2]. In the United States, the prevalence of T. vaginalis among sexually active women was appraised to be 2 to 3 million people with symptomatic infections annually [3]. Several studies have determined the prevalence of trichomoniasis to be between 2-8%, that according to the cultural and social status, can also reach over 30%.
A descriptive, cross-sectional study was carried out on 750 women who attended the Department of Obstetrics and Gynaecology, MVJ Medical College, from October 2010 to September 2012. T. vaginalis was detected in 16 out of the 750 participants (2.1%) (95% CI, 1.1-3.1%) by using culture methods, whereas only 13 of the 16 infected people were found to be positive by the wet mount technique (1.7%).
The ages of the infected individuals ranged from 25 to 46 years, with a mean age of 34 years. The highest infection rate was in the age group of 25-34 years (10/16, 62.5%), that was statistically significant (p<0.05). Fifteen of those who were infected were married housewives and one was widowed. Forty-two women who were infected with [Table/Fig-1] shows T. vaginalis was detected in 16 out of 750 participants (2.1%) by using culture methods whereas only 13 of 16 infected people were positive with the wet mount technique (1.7%) T. vaginalis were detected by clinical examinations, whereas 12 of them were confirmed by the culture and the wet mount methods. Four asymptomatic, infected women were not identified by clinical examinations. The sensitivity, specificity and the positive and the negative predictive values of the clinical diagnosis as compared to those of the culture method were 75%, 95%, 28% and 99%, respectively. There was no statistical correlation between the clinical and the parasitological diagnosis methods.
Detection of Trichomonas Vaginalis in vaginal secretion by parasitological method
| Method | Positive n(%) | Negative n(%) | Total |
|---|
| Culture | 16 (2.1) | 734 (97.9) | 750 |
| Wet mount | 13 (1 .7) | 737 (98.3) | 750 |
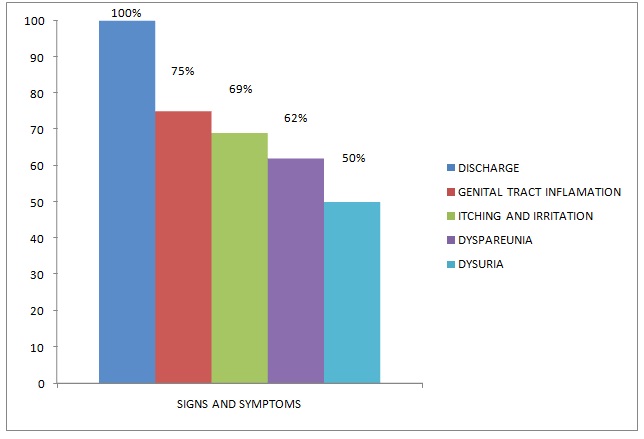
The most common sign was a vaginal discharge (71.3%). The most predominant signs and symptoms included a vaginal discharge, itching, dysuria and inflammation of the genital tract, [Table/Fig-2].
The predominant clinical signs and symptoms of patients infected with Trichomonas Vaginalis
Discussion
Trichomoniasis is the most common non-viral, sexual infection of the genitourinary tract. This infection is mainly transmitted through sexual activities, although a non-sexual transmission has also been reported. In the United States, the prevalence of trichomoniasis has been estimated to be 25% among those who were referred to the STD clinics and it was found to be higher in certain population groups such as in African American women (38%) [2]. For instance, the prevalence of trichomoniasis among HIV-positive women in Zaire and among pregnant women in a rural area in south Africa was estimated as 38% and 65%, respectively [1,2]. In Islamic countries, the prevalence of trichomoniasis ranges from 1.2% in Libya and Jordan to 3.2% in Turkey to 28.1% in Saudi Arabia [4–6]. In this study, the prevalence of trichomoniasis was found to be 2.1% on using the culture method as the gold standard. The difference in the results may be due to the selection of different population groups. Diagnosis of trichomoniasis based on only clinical symptoms should not be done due to the two reasons. First, clinical symptoms of trichomoniasis may be similar to those of other STDs. Second, clinical symptoms such as strawberry cervix and spumy discharge are seen in 2% and 12% of T. vaginalis infected patients, respectively [7–8]. Some studies have indicated that the diagnoses which were based solely on the clinical examinations showed 88% false negative and 29% false positive results [5]. As the most important point of this study, 73.3% of the participants had clinical signs and symptoms. Forty-two of them were clinically diagnosed as infected with T. vaginalis, among which only 12 were confirmed by the culture technique. Also 4 of the infected patients were asymptomatic, who were not diagnosed by clinical examinations. In this study, the positive predictive value for the clinical diagnosis of the T. vaginalis infection was 28% and so the use of laboratory methods was necessary. The most common method for the diagnosis of T. vaginalis is wet mount [Table/Fig-3,5 & 4], but its sensitivity has been reported to be only between 38% and 82%. Molecular methods which are based on PCR are accurate methods with sensitivities of 80% to 100%, but they are not used routinely in all the laboratories, [7].
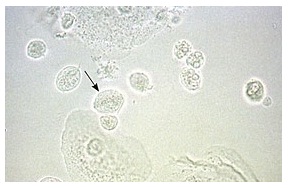
Wet mount of trichomono vaginalis showing trichomonos with flagella
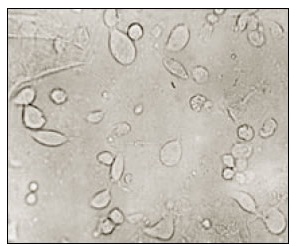
Vaginal wet-mount preparation showing motile trichomonads with flagella (slightly larger than a leukocyte)
Trichomonovaginalis on culture plate

In conclusion, the results of this study showed that the prevalence of the T. vaginalis infection in the study population was relatively low Since the clinical signs of trichomonal vaginitis are the same as those of other STDs, a confirmatory laboratory diagnosis is necessary.
[1]. Schwebke JR, Burgess D, TrichomoniasisClin Microbiol Rev 2004 17(4):794-803. [Google Scholar]
[2]. World Health Organization. Geneva, Switzerland: WHO; 2001. Global prevalence and incidence of selected curable sexually transmitted infections [Google Scholar]
[3]. Jhon DT, Petri WA, Markell and Voge’s Medical Parasitology 2006 Ninth edSt.LouisSaunders [Google Scholar]
[4]. Kassem HH, Majoud OA, Trichomoniasis among women with vaginal discharge in Benghazi city, LibyaJ Egypt Soc Parasitol 2006 36(3):1007-16. [Google Scholar]
[5]. Mahafzah AM, Al-Ramahi MQ, Asa’d AM, El-Khateeb MS, Prevalence of sexually transmitted infections among sexually active Jordanian femalesSex Transm Dis 2008 35(6):607-10. [Google Scholar]
[6]. Selvitopu A, Ozcelik S, Degerli S, The incidence of Trichomonasvaginalis in vaginal specimens from gynecologic patientsTurkiye Parazitol Derg 2006 30(3):175-7. [Google Scholar]
[7]. Vatanshenassan M, Rezaie S, Mohebali M, Niromand N, Kazemi B, Babaei Z, Rezaeian M, Trichomonasvaginalis: investigation of a novel diagnostic method in urine samples using cysteine proteinase 4 gene and PCR techniqueExp Parasitol 2010 126(2):187-90. [Google Scholar]
[8]. Petrin D, Delgaty K, Bhatt R, Garber G, Clinical and microbiological aspects of Trichomonas VaginalisClin Microbiol Rev 1998 11(2):300-17. [Google Scholar]